

Achieving Predictable Bone Regeneration Without Autogenous Grafts
Combining recombinant human platelet-derived growth factor-BB with composite graft materials offers a promising alternative to traditional autogenous bone harvesting.
PURCHASE COURSE
This course was published in the March/April 2025 issue and expires April 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the March/April 2025 issue and expires April 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 490
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the principles of guided bone regeneration (GBR) and its role in addressing severe horizontal and vertical ridge defects in implant dentistry.
- Identify the benefits and limitations of autogenous bone grafts compared to composite graft materials such as allografts and xenografts in combination with recombinant human platelet-derived growth factor-BB (rhPDGF-BB).
- Recognize the surgical techniques employed in GBR, including cortical perforations, membrane stabilization, and the application of the PASS principle for optimal outcomes.
- Evaluate the clinical considerations, potential advantages, and limitations of using rhPDGF-BB in challenging bone augmentation procedures, particularly in the esthetic zone.
Guided bone regeneration (GBR) has become an integral part of implant dentistry. Initially, only simple bone defects, such as a dehiscence or fenestration, were treated with GBR.1 It is currently used extensively for vertical and horizontal ridge augmentation with reproducible outcomes, high implant success, and low complication rates.1-4 Augmentation remains a challenge due to the complexity of hard and soft tissue management. The predictability of the procedure depends on case selection and the anatomy of the defect.
The so-called knife-edged ridge or Cawood and Howell class IV edentulous ridge5 presents a unique challenge for horizontal ridge augmentation. The height of the ridge is adequate, but the width is insufficient for implant placement. GBR, using anorganic bovine bone mineral in combination with autogenous bone has been shown to be effective in maintaining atrophic ridges in the maxillary and mandibular arch.3,4,6-10
Autogenous Bone
The use of the autogenous bone is still considered the gold standard graft material for GBR due to its osteogenic, osteoconductive, and osteoindutive properties.11 Unfortunately, autogenous bone, commonly harvested from the ramus and symphysis area, is associated with increased patient morbidity.12,13 Furthermore, a recent systematic review reported no significant clinical differences in implant success rates between the use of autogenous bone and other bone substitutes. Likewise, a systematic review of randomized clinical trials of different bone graft materials showed no significant differences in the bone gains between the materials with successful clinical and histological outcomes.11,14-19
Growth Factors
The introduction of growth factors represents a new era in wound healing.20 The rationale behind the use of these natural biological mediators is to regulate crucial cellular events involved in tissue repair, including DNA synthesis, cell replication, chemotaxis, differentiation, matrix synthesis, and tissue vascularization.21 Several preclinical and clinical studies have documented the use of different bioactive factors in enhancing bone regeneration.22 These biologic materials may enhance the development of mature lamellar bone and lead to more predictable support for dental implants. One of the best-documented growth factors proven to have positive effects on a myriad of oral regenerative procedures is recombinant human platelet-derived growth factor-BB (rhPDGF-BB).
PDGF is derived and released from human platelets cells following tissue injury.23 Obtained with recombinant DNA processing, rh-PDGF has been shown to upregulate angiogenesis and promote guided bone regeneration in large horizontal ridge defects.24,25 The main effect of rhPDGF-BB is mitogenesis, angiogenesis, and chemotaxis for cells of mesenchymal origin, increasing the potential for regeneration.23,26-29 Animal and human histological studies revealed bone volume regeneration after implantation of rhPDGF-infused xenograft.30-33
A recent systematic review that assessed the clinical efficacy, safety, and benefits of rh-PDGF in hard and soft tissue regeneration reported that the combined use of the bone grafts substitutes (xenografts, allografts) and rh-PDGF demonstrated clinical benefits for periodontal regeneration, root coverage, alveolar ridge augmentation, and ridge preservation.20
Several case studies using combinations of autogenous bone, anorganoic bovine, bone-derived mineral, and rhPDGF have demonstrated a high success rate.30,34,35 However, the harvesting of autogenous bone involves an additional surgical procedure. Limited information regarding the use of rhPDGF in combination with composite graft materials for horizontal and vertical ridge augmentation in the esthetic zone is available. The following case report details the successful use of rhPDGF in conjunction with allograft/xenograft and a barrier membrane to reconstruct severe bone defects in the esthetic zone.
Case Report
A systemically healthy man presented for implant placement in the anterior area due to significant trauma resulting in the loss of teeth #9 and 10 (Figure 1). A treatment plan was developed to provide GBR to reconstruct the regional anatomy. The patient was premedicated with 2 g amoxicillin 1 hour prior to surgery. Local anesthesia was provided via infiltration using 2% lidocaine (1:100,000 epinephrine). Initial incisions were made mid-crestally from tooth #8 to 11, with vertical release incisions at #8 mesiobuccal line angle and #11 distobuccal line angle followed by full thickness flap reflection.
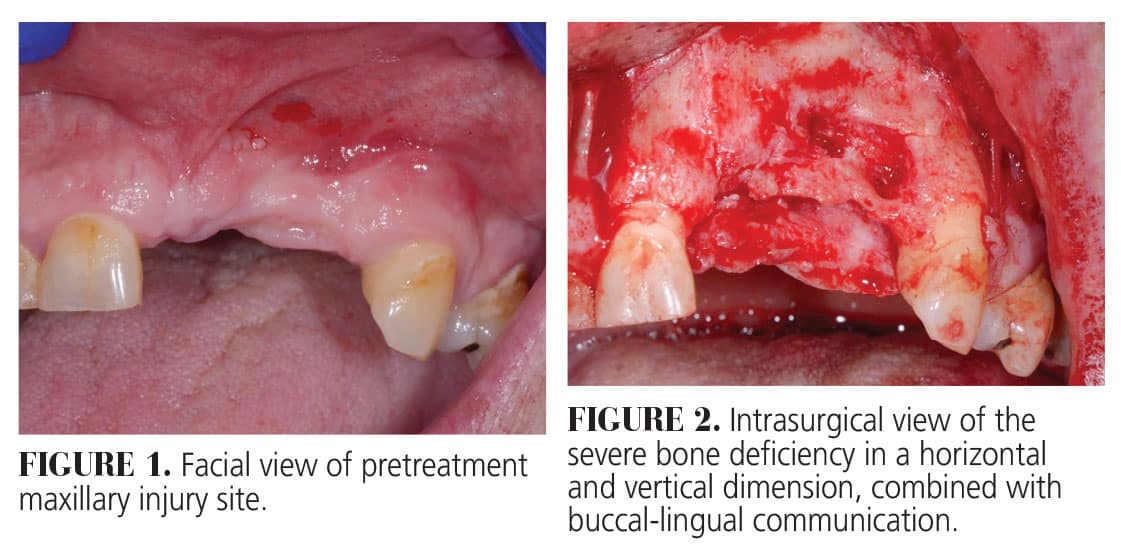
The residual defect was classified as a severe combined horizontal and vertical ridge defect. A through-and-through defect was detected in the left area of the premaxilla (Figure 2). Favorably, the alveolar bone observed on the adjacent natural teeth #8 and11 was intact. Following degranulation, cortical perforations were made to stimulate angiogenesis. A resorbable collagen membrane was trimmed and stabilized on the facial with titanium microscrews, allowing the composite bone graft to be condensed until an ideal geometric form was achieved (Figure 3).
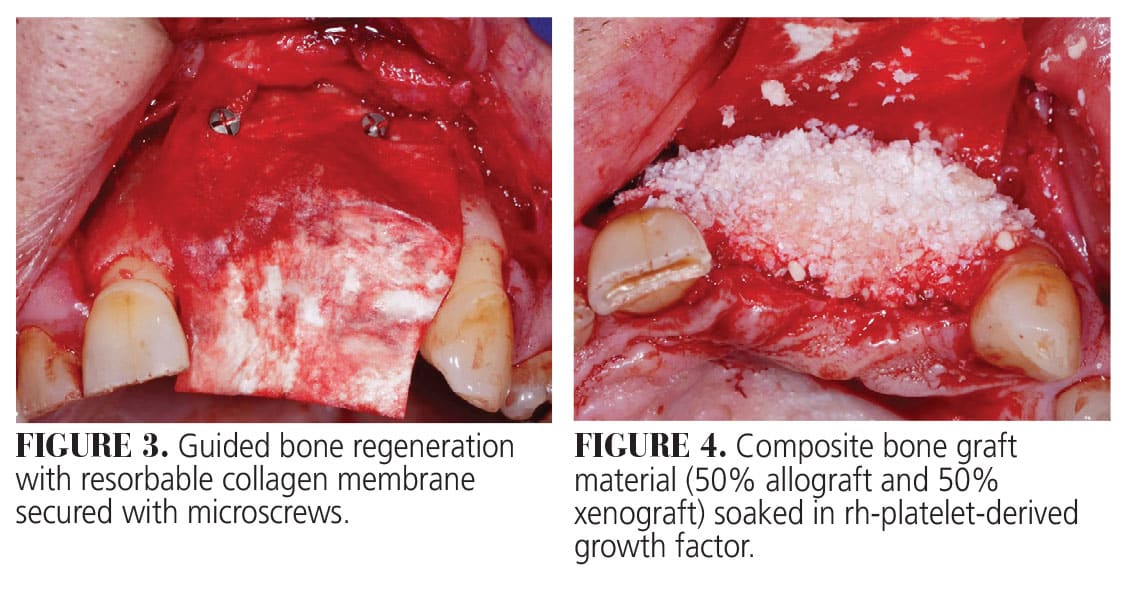
The construct was a composite bone graft consisting of 50% mineralized freeze-dried bone allograft and 50% inorganic bovine bone hydrated for 15 minutes with rhPDGF-BB. Another layer of construct was placed over the composite graft to provide further volume stability (Figure 4). The collagen membrane was then rotated to the palate, extending apically beyond the extent of the defect, and stabilized on the lingual using an additional screw (Figure 5). The flap was released through full/split dissection to ensure tension free primary wound closure using multiple single interrupted and horizontal mattress 5-0 polypropylene sutures (Figure 6).
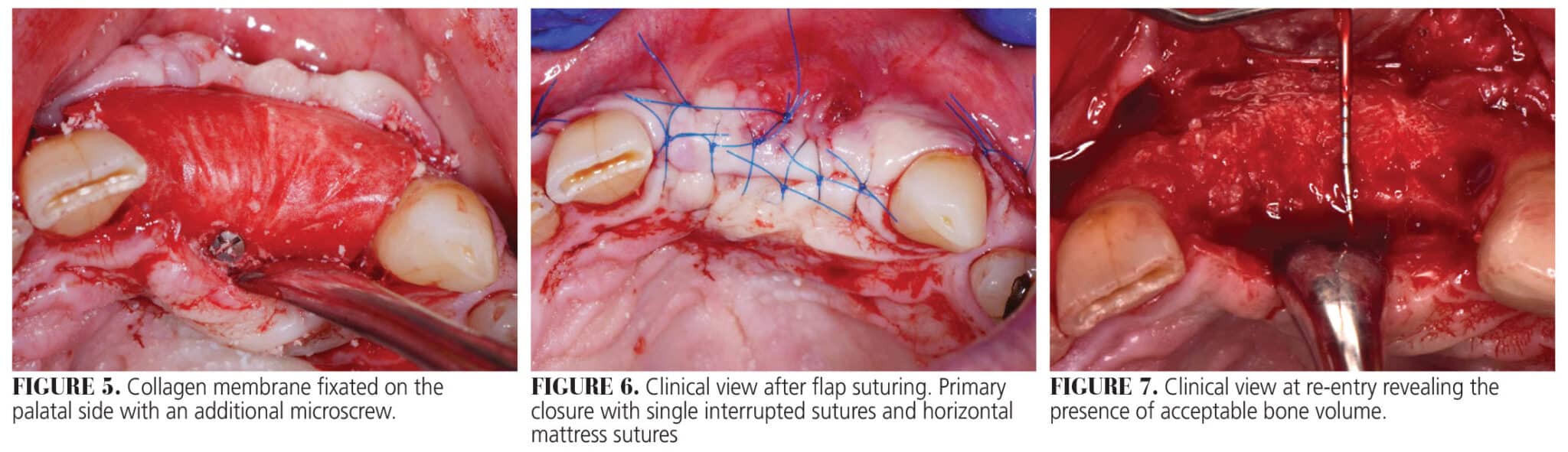
The flap was sutured in two layers. First, a horizonal mattress suture was placed 4 mm from the incision line; second, single interrupted sutures were placed to close the edges of the flap leaving at least 4 mm of the connective tissue layer between the membrane and the oral epithelium. This double layer suture technique approximates the connective tissue of the lingual and buccal flaps, providing a barrier preventing flap exposure. The vertical releasing incisions were closed with single interrupted sutures.
The instructions given prior to the procedure were reviewed again, both verbally and in writing. Post-operative antibiotics consisted of amoxicillin 500 mg q8h × 10 days, bimodal dosing of ibuprofen 600 mg + acetaminophen 650 mg q6h prn and bid rinsing with 0.12% chlorhexidine digluconate. Post-operative follow-up occurred at 3, 8, and 16 weeks and at 6 months. Throughout the duration of healing, the patient reported minimal discomfort and no complications were reported or observed.
Implant surgery was performed at 6 months after the ridge augmentation procedure. Flap reflection revealed outstanding three-dimensional bone gain in a vertical and horizontal direction (Figure 7). The bone was revascularized with excellent bleeding. Implant placement was performed according to the manufacturer instructions. Two tapered 3.8 × 10 mm implants were placed in a two-stage fashion in the position of teeth #9 and 10 (Figure 8). A further horizontal and vertical bone augmentation was performed around the dental implants using the same composite graft soaked in rh-PDGF. The construct was applied to a vertical peri-implant bone defect and covered with a collagen membrane (Figure 9). Primary closure was obtained with single interrupted 5-0 polypropylene sutures.
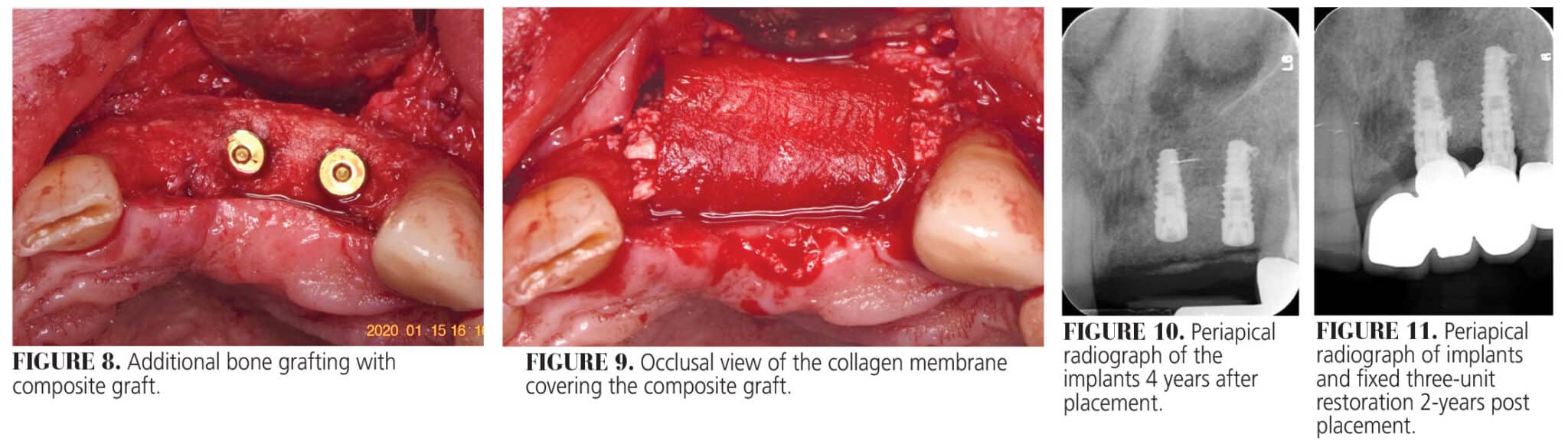
A post-operative radiograph was taken to confirm implant positioning two dimensionally (Figure 10). Two of the fixation tacks placed at the GBR surgery were left submerged as they were covered with osseous tissue, and their maintenance did not influence implant placement.
Exposure of the implants was performed after 3 months to place healing abutments. Bone augmentation procedures often result in coronal shift of the mucogingival junction (MGJ). Therefore, the exposure procedure started with a horizontal incision between the adjacent teeth (#8 and 11), 1 to 2 mm lingual from the previous horizontal midcrestal incision.
The location of the palatal incision depends on the amount of keratinized tissue present on the buccal side. The flap was elevated in a full split thickness to reposition the MGJ apically to its original position prior to the bone augmentation procedure. Furthermore, this buccally repositioned flap allows for the 3 to 4 mm of keratinized tissue to be buccally displaced avoiding the need for a second surgery to increase the amount of keratinized tissue. The cover screws were replaced with tall healing abutments.
Final restoration was completed 5 months later. Figure 11 depict the patient 4 years after placement of the final restoration indicating minimal remodeling of the augmented site. The patient reported no adverse events since the procedure was completed.
Discussion
This case report demonstrates the successful application of a staged surgical approach to achieve combined vertical and horizontal site augmentation. With the advancement of biomaterials, GBR has become the most frequently preformed procedure for most of the horizontal and vertical ridge augmentation procedures. A staged approach was chosen in this case because the initial width of the ridge was not conducive to implant placement. A systematic review reported the average gain in the width following staged horizontal ridge augmentation was 3.9 mm.36 A greater gain in width close to 6 mm was reported by Urban et al.1,35
In this case, the final gain in width was close to 10 mm. We attribute this large gain to the following:
- Composite graft material used consisted of a 50/50 mixture of allograft and xenograft.
- Xenograft material has a high osteointegration capacity promoting host cells and vessel migration.
The inorganic bovine bone mineral has the potential to be colonized by CD44-positive osteocytes to promote neovascularisation. Their osteoconductive properties, combined with their very slow resorbing rate, maintain the volume of the regenerated bone over time.
The allograft contained 50/50 corticocancellous bone chips, providing an osteoconductive scaffold. The lack of osteogenic properties of these materials is overcome by the use of rh-PDGF. This growth factor is naturally produced during the early stages of healing accelerating the regenerative phase with early production of bloods vessels, anastomosis, osteoblasts, and fibroblast migration.37 The use of the rh-PDGF was aimed at promoting angiogenic growth inside the composite graft material and recruiting osteoblasts contributing new bone regeneration. The composite graft was stabilized by the use of a resorbable collagen membrane. The fixation of the membrane on the buccal and palatal aspect with titanium screws immobilized the graft material, allowing the formation of the desired amount of bone. Another factor that contributes to the success of this surgery was the application of the PASS principle (primary wound closure, angiogenesis, clot stability and space maintenance).38
Conclusion
This case report demonstrates that severe ridge deficiency can be reconstructed through advanced GBR surgery without the need for harvesting autogenous bone, therefore reducing the trauma to the patient by avoiding a second surgery site.
Remarkable bone regeneration can be achieved by using rhPDGF in conjunction with a composite graft material immobilized by a resorbable collagen membrane, as seen in the case study. It has further provided evidence regarding the potential use of the rh-PDGF in challenging situations with both vertical and horizontal bone defects. However, limited clinical evidence is available regarding this technique and the long-term success of the regenerated bone, including implant success.
References
- Urban IA, Nagursky H, Lozada JL. Horizontal ridge augmentation with a resorbable membrane and particulated autogenous bone with or without anorganic bovine bone-derived mineral: a prospective case series in 22 patients. Int J Oral Maxillofac Implants. 2011;26:404-414.
- Buser D, Ingimarsson S, Dula K, Lussi A, Hirt HP, Belser UC. Long-term stability of osseointegrated implants in augmented bone: a 5-year prospective study in partially edentulous patients. Int J Periodontics Restorative Dent. 2002;22:109-117.
- Urban IA, Lozada JL, Jovanovic SA, Nagursky H, Nagy K. Vertical ridge augmentation with titanium-reinforced, dense-PTFE membranes and a combination of particulated autogenous bone and anorganic bovine bone-derived mineral: a prospective case series in 19 patients. Int J Oral Maxillofac Implants. 2014;29:185-193.
- Urban IA, Jovanovic SA, Lozada JL. Vertical ridge augmentation using guided bone regeneration (GBR) in three clinical scenarios prior to implant placement: a retrospective study of 35 patients 12 to 72 months after loading. Int J Oral Maxillofac Implants. 2009;24:502-510.
- Cawood JI, Howell RA. A classification of the edentulous jaws. Int J Oral Maxillofac Surg. 1988;17:232-236.
- Urban IA, Montero E, Amerio E, Palombo D, Monje A. Techniques on vertical ridge augmentation: Indications and effectiveness. Periodontol 2000. 2023;93:153-182.
- Urban IA, Monje A, Lozada J, Wang HL. Principles for vertical ridge augmentation in the atrophic posterior mandible: a technical review. Int J Periodontics Restorative Dent. 2017;37:639-645.
- Urban IA, Monje A, Wang HL. Vertical ridge augmentation and soft tissue reconstruction of the anterior atrophic maxillae: a case series. Int J Periodontics Restorative Dent. 2015;35:613-623.
- Canullo L, Trisi P, Simion M. Vertical ridge augmentation around implants using e-PTFE titanium-reinforced membrane and deproteinized bovine bone mineral (bio-oss): A case report. Int J Periodontics Restorative Dent. 2006;26:355-361.
- Simion M, Jovanovic SA, Trisi P, Scarano A, Piattelli A. Vertical ridge augmentation around dental implants using a membrane technique and autogenous bone or allografts in humans. Int J Periodontics Restorative Dent. 1998;18:8-23.
- Jensen SS, Terheyden H. Bone augmentation procedures in localized defects in the alveolar ridge: clinical results with different bone grafts and bone-substitute materials. Int J Oral Maxillofac Implants. 2009;24 Suppl:218-236.
- Nkenke E, Schultze-Mosgau S, Radespiel-Troger M, Kloss F, Neukam FW. Morbidity of harvesting of chin grafts: a prospective study. Clin Oral Implants Res. 2001;12:495-502.
- Raghoebar GM, Louwerse C, Kalk WW, Vissink A. Morbidity of chin bone harvesting. Clin Oral Implants Res. 2001;12:503-507.
- Chavda S, Levin L. Human studies of vertical and horizontal alveolar ridge augmentation comparing different types of bone graft materials: a systematic review. J Oral Implantol. 2018;44:74-84.
- Papageorgiou SN, Papageorgiou PN, Deschner J, Gotz W. Comparative effectiveness of natural and synthetic bone grafts in oral and maxillofacial surgery prior to insertion of dental implants: Systematic review and network meta-analysis of parallel and cluster randomized controlled trials. J Dent. 2016;48:1-8.
- Feuille F, Knapp CI, Brunsvold MA, Mellonig JT. Clinical and histologic evaluation of bone-replacement grafts in the treatment of localized alveolar ridge defects. Part 1: Mineralized freeze-dried bone allograft. Int J Periodontics Restorative Dent. 2003;23:29-35.
- Langer B, Langer L, Sullivan RM. Vertical ridge augmentation procedure using guided bone regeneration, demineralized freeze-dried bone allograft, and miniscrews: 4- to 13-year observations on loaded implants. Int J Periodontics Restorative Dent. 2010;30:227-235.
- Hammerle CH, Jung RE, Yaman D, Lang NP. Ridge augmentation by applying bioresorbable membranes and deproteinized bovine bone mineral: a report of twelve consecutive cases. Clin Oral Implants Res. 2008;19:19-25.
- Zitzmann NU, Scharer P, Marinello CP, Schupbach P, Berglundh T. Alveolar ridge augmentation with Bio-Oss: a histologic study in humans. Int J Periodontics Restorative Dent. 2001;21:288-295.
- Tavelli L, Ravida A, Barootchi S, Chambrone L, Giannobile WV. Recombinant human platelet-derived growth factor: a systematic review of clinical findings in oral regenerative procedures. JDR Clin Trans Res. 2021;6:161-173.
- Giannobile WV, Somerman MJ. Growth and amelogenin-like factors in periodontal wound healing. A systematic review. Ann Periodontol. 2003;8:193-204.
- Donos N, Dereka X, Calciolari E. The use of bioactive factors to enhance bone regeneration: A narrative review. J Clin Periodontol. 2019;46 Suppl 21:124-161.
- Yao W, Shah B, Chan HL, Wang HL, Lin GH. Bone quality and quantity alterations after socket augmentation with rhpdgf-bb or bmps: a systematic review. Int J Oral Maxillofac Implants. 2018;33:1255-1265.
- Snyder MB. Treatment of a large postextraction buccal wall defect with mineralized allograft, beta-TCP, and rhPDGF-BB: a growth factor-mediated bone regenerative approach. Int J Periodontics Restorative Dent. 2012;32:705-711.
- De Angelis N, De Lorenzi M, Benedicenti S. Surgical combined approach for alveolar ridge augmentation with titanium mesh and rhPDGF-BB: a 3-year clinical case series. Int J Periodontics Restorative Dent. 2015;35:231-237.
- Phipps MC, Xu Y, Bellis SL. Delivery of platelet-derived growth factor as a chemotactic factor for mesenchymal stem cells by bone-mimetic electrospun scaffolds. PLoS One. 2012;7:e40831.
- Nevins M, Giannobile WV, McGuire MK, et al. Platelet-derived growth factor stimulates bone fill and rate of attachment level gain: results of a large multicenter randomized controlled trial. J Periodontol. 2005;76:2205-2215.
- McGuire MK, Kao RT, Nevins M, Lynch SE. rhPDGF-BB promotes healing of periodontal defects: 24-month clinical and radiographic observations. Int J Periodontics Restorative Dent. 2006;26:223-231.
- Nevins M, Camelo M, Nevins ML, Schenk RK, Lynch SE. Periodontal regeneration in humans using recombinant human platelet-derived growth factor-BB (rhPDGF-BB) and allogenic bone. J Periodontol. 2003;74:1282-1292.
- Simion M, Nevins M, Rocchietta I, et al. Vertical ridge augmentation using an equine block infused with recombinant human platelet-derived growth factor-BB: a histologic study in a canine model. Int J Periodontics Restorative Dent. 2009;29:245-255.
- Nevins M, Garber D, Hanratty JJ, et al. Human histologic evaluation of anorganic bovine bone mineral combined with recombinant human platelet-derived growth factor BB in maxillary sinus augmentation: case series study. Int J Periodontics Restorative Dent. 2009;29:583-591.
- Nevins ML, Camelo M, Schupbach P, Kim DM, Camelo JM, Nevins M. Human histologic evaluation of mineralized collagen bone substitute and recombinant platelet-derived growth factor-BB to create bone for implant placement in extraction socket defects at 4 and 6 months: a case series. Int J Periodontics Restorative Dent. 2009;29:129-139.
- Simion M, Rocchietta I, Kim D, Nevins M, Fiorellini J. Vertical ridge augmentation by means of deproteinized bovine bone block and recombinant human platelet-derived growth factor-BB: a histologic study in a dog model. Int J Periodontics Restorative Dent. 2006;26:415-423.
- Simion M, Rocchietta I, Monforte M, Maschera E. Three-dimensional alveolar bone reconstruction with a combination of recombinant human platelet-derived growth factor BB and guided bone regeneration: a case report. Int J Periodontics Restorative Dent. 2008;28:239-243.
- Urban IA, Lozada JL, Jovanovic SA, Nagy K. Horizontal guided bone regeneration in the posterior maxilla using recombinant human platelet-derived growth factor: a case report. Int J Periodontics Restorative Dent. 2013;33:421-425.
- Sanz-Sanchez I, Ortiz-Vigon A, Sanz-Martin I, Figuero E, Sanz M. Effectiveness of lateral bone augmentation on the alveolar crest dimension: a systematic review and meta-analysis. J Dent Res. 2015;94:128S-142S.
- Chiantella GC. Horizontal guided bone regeneration in the esthetic area with rhpdgf-bb and anorganic bovine bone graft: a case report. Int J Periodontics Restorative Dent. 2016;36:e9-15.
- Wang HL, Boyapati L. “PASS” principles for predictable bone regeneration. Implant Dent. 2006;15:8-17.
From Decisions in Dentistry. March/April 2025;11(2):36-39.

