

The Critical Role of Maintenance
Evidence-based maintenance protocols are essential to protecting long-term implant survival.
Dental implants do not just fail. We fail them — through a disregard of biological, restorative, and maintenance principles.1 True implant success tests the resilience of the peri-implant apparatus. Because implants lack a periodontal ligament, exhibit collagen fibers aligned parallel rather than perpendicular to their surface, and host a unique microbiome in which fewer than 10% of species overlap with periodontal niches, they function within their own ecological and immunologic environment.1,2 This environment is acutely sensitive to both patient self-care and the quality of professional maintenance.
A growing clinical consensus indicates that peri-implant diseases are largely preventable when risk factors are properly managed and robust maintenance protocols are followed.1,3 Without such support, dysbiotic biofilm accumulates, provoking rapid inflammatory change, implant surface degradation, and nonlinear bone loss.3 Peri-implantitis progresses faster than periodontitis, with lesions nearly twice as large and driven by more aggressive cytokine profiles.3 Early and ongoing recare can safeguard implants from this destructive sequelae. Yet it is the standard of maintenance that shapes their prognoses.
Emerging research has refined the understanding of material-tissue interactions, revealing that titanium is not inert; when its protective dioxide layer is disrupted, ions and particles are released, amplifying a local inflammatory reaction known as metallosis.3,4 Tribocorrosion from improper hand or power instrumentation can initiate or accelerate tissue breakdown, making surface-safe debridement essential.
Risk Factors Impacting Maintenance
Active or previous periodontitis captures the biological, mechanical, behavioral, and environmental factors that undermine implant health. Numerous longitudinal studies confirm that patients with successfully treated periodontitis had higher rates of peri-implant mucositis, bone loss, and implant failure than periodontally healthy individuals.3,5 In fact, without maintenance, tissue level implants had a 15-fold increased risk of peri-implant bone loss in periodontally compromised patients in a 20-year follow-up.5 Even with successful treatment, these patients remain vulnerable to biological complications, underscoring the importance of structured, ongoing maintenance for implants.
This inherent vulnerability reinforces the role of soft tissue phenotype, as the peri-implant complex depends on sufficient, resilient mucosal tissue to buffer change. Thin mucosal tissues provide less protection against mechanical forces, poor prosthetic design, and plaque accumulation.1,6 Wider bands of keratinized mucosa are generally associated with improved patient comfort, reduced inflammation, and more stable marginal bone levels, though controversial.3,6
An often-cited meta-analysis revealed that sites with insufficient keratinized tissue are more prone to bleeding, discomfort during brushing, and biofilm retention, all of which can precipitate disease progression.6 When a peri-implant tissue deficiency is identified, augmentation procedures may be performed before implant placement, loading, or during peri-implantitis therapy.
Suboptimal prosthetic designs further complicate maintenance, creating situations where clinicians are unable to diagnose or manage disease effectively. Overcontoured crowns, emergence profiles exceeding 30°, prosthetic splinting, open contacts, and deep restorative margins impede hygiene access and collect biofilm.7
A recent systematic review and meta-analysis found strongly associated overcontoured prostheses to peri-implantitis prevalence, with some reports above 80%.7 Remnants from cement-retained restorations can trigger persistent inflammation with their detection becoming more difficult among deeper margins or multiple or splinted units.3,7 Maintenance therefore begins with a well-designed restoration from a properly placed implant.
From there, broader influences come into play. Cigarette smoking, for example, impairs both perioperative and long-term treatment outcomes with a dose-dependent response.2,3 A 2024 meta-analysis associated vaping with negative esthetic, clinical, and radiographic parameters; it is gaining popularity among young adults.8 Even with discontinued use, disease susceptibility may only begin to re-approximate the risk of a nonsmoker after 21 years.2,3 Early intervention and cessation can be life-changing and should be discussed during subsequent maintenance visits.9
Attention must also be given to systemic factors, which exert equally significant biological pressures. Obesity and uncontrolled type 2 diabetes mellitus (T2DM) create a chronically pro-inflammatory, dysregulated host environment that undermines peri-implant health. Findings from the Academy of Osseointegration and American Academy of Periodontology Consensus on Prevention and Management of Peri-Implant Diseases and Conditions suggest that obesity does not consistently reduce implant survival but is associated with deeper peri-implant pockets, more bleeding on probing, and greater marginal bone loss, increasing the risk of peri-implant diseases.3
Poorly controlled T2DM slows and impairs osseointegration, leading to early implant failure and complications compared to healthy or well-controlled patients.3,9 Nutritional counseling can broaden the impact of recare, supporting not only oral health but mental and systemic wellness.
Yet across all categories, one powerful and modifiable factor remains: adherence to routine professional maintenance. Because even with these comorbidities, patients who were maintained every 3 to 6 months had better therapeutic outcomes.1,3,5,9 These findings demonstrate that maintenance is not merely beneficial but essential, functioning as the primary defense against disease initiation and escalation.
Maintenance and Self-Care Protocols
Implant maintenance necessitates a shift from traditional instrumentation to more biologically compatible techniques. High-abrasion polishing pastes, stainless steel curettes, and certain ultrasonic tips can scratch or strip the protective dioxide layer of an integrated implant, potentially releasing metal particles and altering cellular responses via metallosis.2,4,9 Low-abrasion air-polishing techniques with erythritol powder via guided biofilm therapy consistently demonstrated high effectiveness with minimal surface disruption.4,10 A 2025 randomized clinical trial comparing erythritol-based air polishing with ultrasonic debridement using a polyetheretherketone insert found both modalities reduced probing depths and bleeding on probing, but air polishing achieved patient-preferred comfort with less instrumentation time and greater surface decontamination.11
 Self-care instruction should then complement professional therapy. Patients must be taught techniques compatible with their implant prosthesis. For many, conventional wax or unwaxed floss may not be appropriate, as it can lodge around misfit abutments and exposed threads, acting as plaque-retentive foreign bodies in the peri-implant sulcus.12 Water flossers, by contrast, offer improved plaque removal in both supragingival and subgingival spaces and are more practical for multiple and full-arch implant restorations on a low-to-medium setting.12,13
Self-care instruction should then complement professional therapy. Patients must be taught techniques compatible with their implant prosthesis. For many, conventional wax or unwaxed floss may not be appropriate, as it can lodge around misfit abutments and exposed threads, acting as plaque-retentive foreign bodies in the peri-implant sulcus.12 Water flossers, by contrast, offer improved plaque removal in both supragingival and subgingival spaces and are more practical for multiple and full-arch implant restorations on a low-to-medium setting.12,13
Removable locator- and bar-retained implant-assisted overdentures require daily cleaning and periodic replacement of worn attachments. Patients should be encouraged to debride the intaglio surface with a specialized electric brush head, then rinse it in an antimicrobial solution.14 Fixed full-arch restorations demand meticulous self-care with similar brushing and interproximal aids and should then be removed every 18 months, on average, for complete evaluation and debridement.13,14 These maintenance routines, though time-intensive, protect difficult-to-reach mucosal tissues beneath larger prosthetic surfaces.
Maintenance should extend through every phase of treatment, independent of the final prosthesis. Because healing follows a predictable biological sequence, implant debridement and recare should be timed to align with each stage as follows:
- Two weeks. Inflammation is prevalent, as the epithelial seal is still forming around the implant collar.15 Gentle biofilm disruption and reinforcement of self-care with a hygiene team prevent its early breakdown.
- Six to eight weeks. Woven bone remodeling and connective-tissue organization accelerate along the implant body.15 Localized debridement prevents deeper plaque penetration and ensures all restorative steps occur in a healthy, stable environment.
- Twelve weeks. Lamellar bone has matured and osseointegration is sufficiently established.15 Radiographs and gentler clinical measurements should be taken to guide long-term maintenance planning and self-care, with more thorough surface debridement.
Personalized maintenance reduces probing depths, bleeding, and other negative indices, especially for already ailing implants or periodontal patients.1,9,14 Large cohort data continue to confirm higher implant survival rates among patients who remain in regular maintenance programs.5,14 Implant maintenance is indispensable in preventing disease recurrence and maintaining stability, especially when 60% of treated diseased implants relapse, requiring secondary intervention or removal, in as little as 1 year.16
Case Report
The following case outlines the management of a failing dentition through comprehensive periodontal and implant therapy. A 59-year-old man presented to a private practice dissatisfied with his smile and experiencing increasing discomfort in the posterior region secondary to long-standing, untreated periodontitis (Figures 1-16). His medical history was noncontributory aside from a penicillin allergy. He reported smoking one pack of cigarettes daily for at least 20 years.
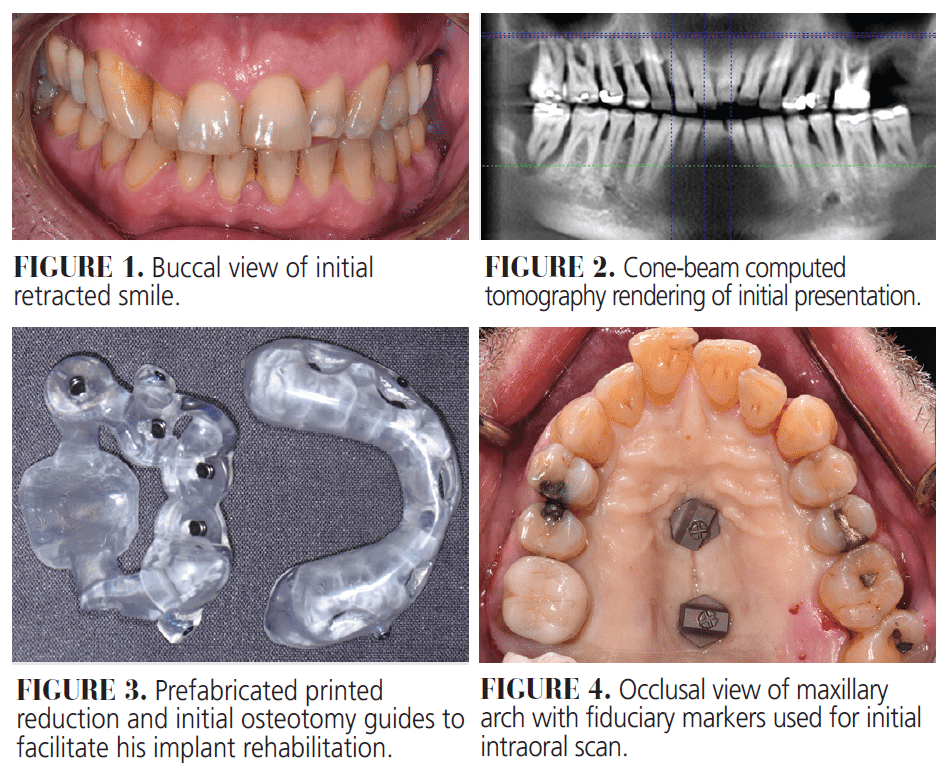
The patient expressed concern about losing additional teeth without a definitive plan in place. Clinical examination revealed generalized pink-red, edematous, and poorly attached periodontal tissues with heavy plaque, calculus, and debris accumulation throughout. Probing depths ranged from 4 to 10 mm with profuse bleeding on probing and/or suppuration. Cone-beam computed tomography (CBCT) imaging revealed generalized moderate-to-severe horizontal bone loss with isolated vertical defects and periapical or furcal lesions.
After a thorough evaluation and discussion of treatment options, a comprehensive plan was developed and informed consent was obtained. Although a removable, implant-assisted prosthesis would have been ideal given his periodontal and smoking histories, the patient declined any removable solution and accepted the associated risks. He agreed to a strict maintenance program. Intraoral scans, CBCT imaging, photographs, and videos, collected as part of his initial consultation, were sent to the laboratory to digitally plan same-day implant placement in the maxillary arch and next-day loading.
- Initial debridement and self-care instruction with the dental hygiene team was performed to reduce inflammation, lower the bacterial load, and reinforce proper oral hygiene.
- Digital implant planning for fabrication of tooth-borne reduction and osteotomy guides was completed to ensure implant positioning and accuracy.
- Full-mouth periodontal and implant therapy was initiated to remove hopeless teeth, control periodontal infection, and prepare the arches for implant-supported rehabilitation.
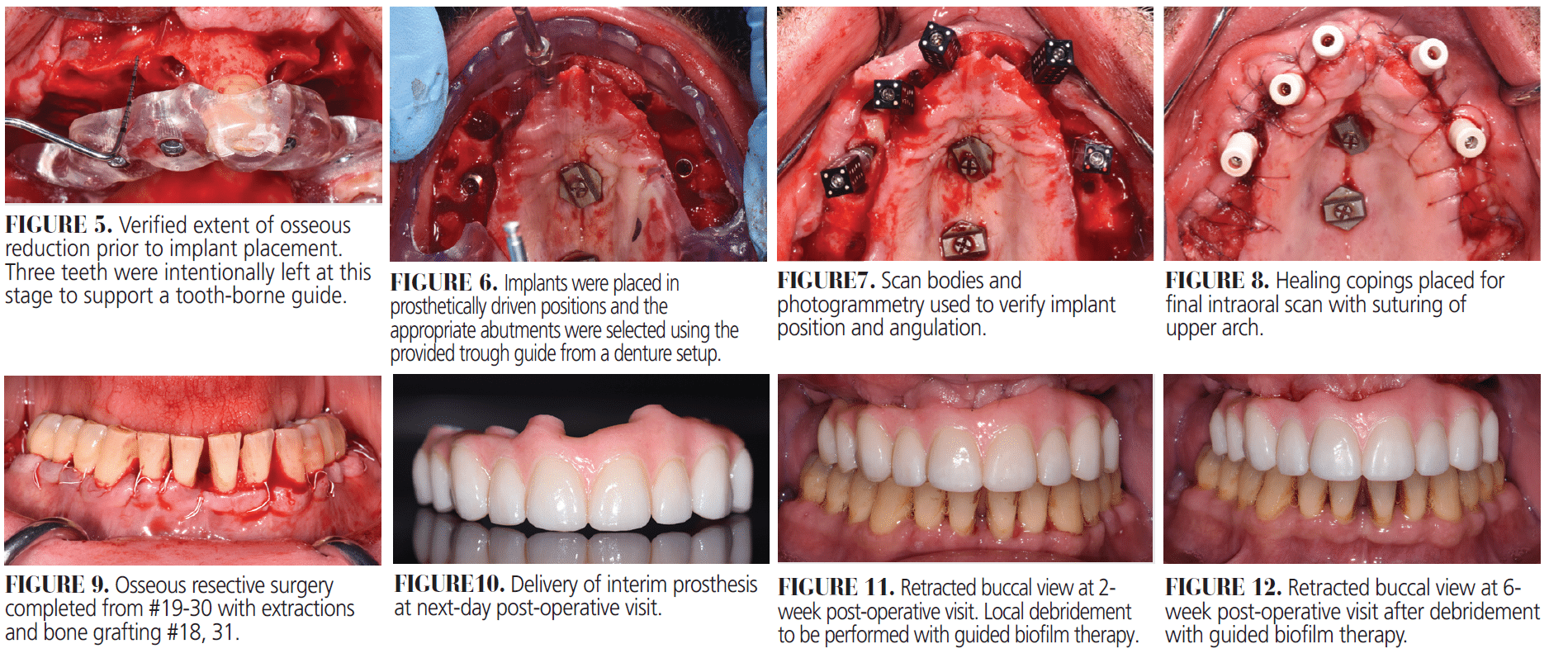
- Extraction of all remaining maxillary teeth and implant placement for next-day conversion using a digital workflow were carried out to remove nonrestorable teeth and provide an immediate functional and esthetic restoration.
- Osseous resective surgery #19 to 30 with extractions and bone grafting of #18; #31 was performed to correct periodontal defects, remove hopeless teeth, and regenerate adequate bone for periodontal stability.
- Follow-up visits with localized debridement using guided biofilm therapy at 2, 6, and 12 weeks were scheduled to control biofilm during healing and support peri-implant health.
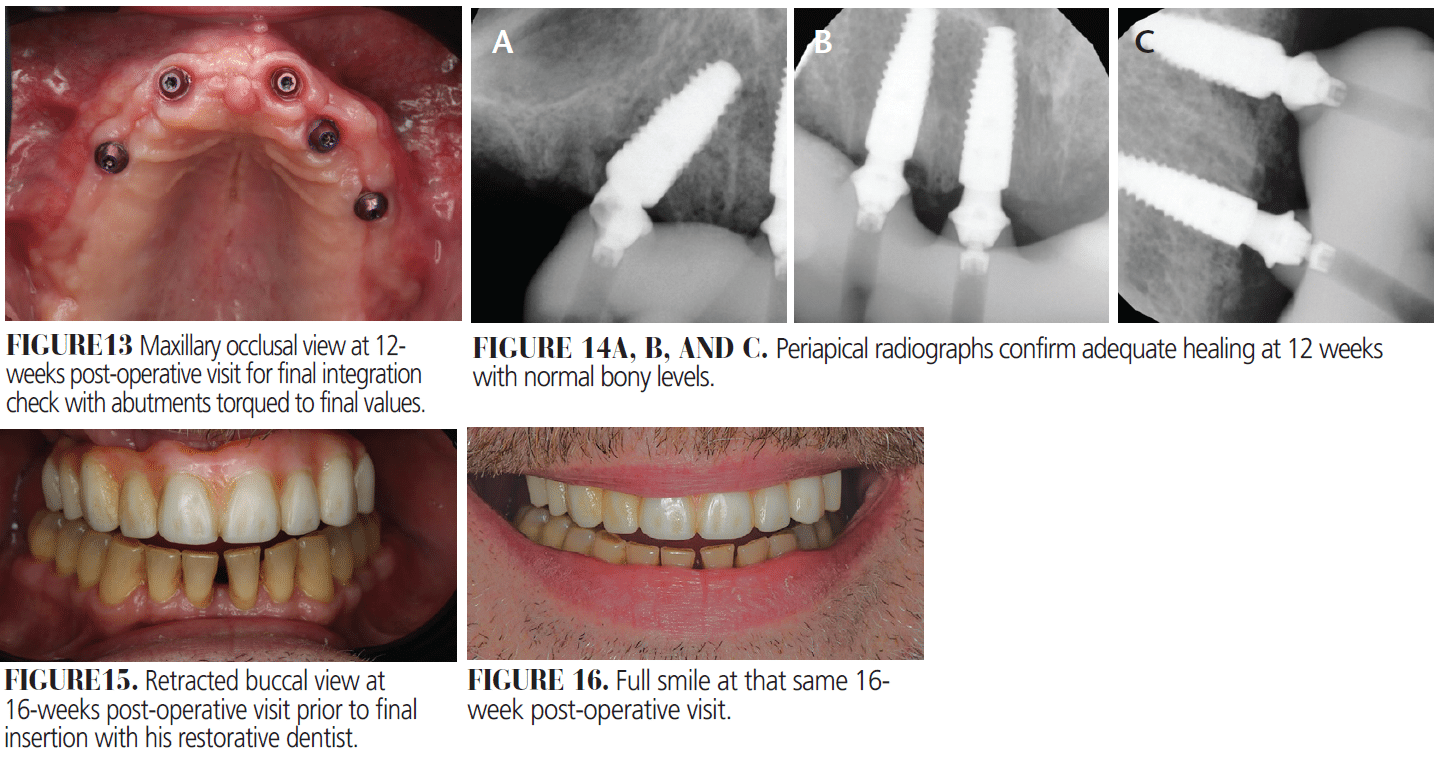
- A final integration check and delivery of the final prototype by the restorative dentist were completed to verify implant integration, confirm abutment stability, and finalize the prosthetic design.
- Periodontal maintenance every 3 months was prescribed to monitor tissue health, maintain implant stability, and prevent recurrence of periodontal disease.
His initial debridement was performed by the dental hygienist, emphasizing the importance of long-term maintenance and patient compliance from treatment onset. He was given a pressure-controlled electric toothbrush with specialized heads, stabilized chlorine dioxide rinse, and a water flosser. Oral hygiene instructions were reviewed and demonstrated at this and subsequent visits. They were provided in written and video formats for improved compliance.
All remaining maxillary teeth were extracted, and alveolar ridge reduction was completed using a prefabricated printed guide to achieve appropriate prosthetic space. Bone-level implants were placed with the aid of a tooth-borne guide for initial osteotomy preparation. Following abutment selection and placement using a denture trough guide, photogrammetry was performed to verify implant position and angulation remotely with the laboratory. Extraction sockets were grafted, flaps were repositioned, and resorbable sutures were placed. A final intraoral scan was taken to initiate fabrication of a milled provisional restoration to enhance form and function. Osseous resective surgery was then completed from #19-30, along with extraction and grafting of hopeless teeth #18 and #31.
The patient returned the next day for delivery of the interim full-arch maxillary restoration. Oral hygiene protocols were reinforced, and he was scheduled for subsequent follow-ups at 2, 6, and 12 weeks for guided biofilm therapy and evaluation. At the final integration check, radiographs confirmed satisfactory healing, and abutments were torqued to their final values. Updated intraoral scans and photogrammetry records were sent to the laboratory to fabricate the final prototype to be delivered by the restorative dentist.
The patient continues to be seen every 3 months for periodontal maintenance. With consistent follow-up, improved oral hygiene practices, and his growing sense of agency and ownership over his oral health, the patient is expected to achieve stable long-term function despite the significant risk factors present at the start of treatment.
Future Directions
A structured post-operative schedule at 2, 6 to 8, and 12 weeks, followed by maintenance every 3 to 6 months depending on risk, reflects tissue healing and is especially important in full-arch implant therapy, where extensive prosthetic surfaces increase hygiene challenges. Early recare enables clinicians to identify inflammation, open contacts, prosthetic convexities, or residual cement before they contribute to irreversible bone loss. Although clinical experience supports this approach, high-quality evidence remains limited. More robust research is needed to evaluate how specific maintenance intervals influence inflammatory markers, microbial changes, radiographic bone stability, and long-term implant survival. Even so, maintenance is as essential to implant therapy as the implant it supports.
References
- Wang HL, Avila-Ortiz G, Monje A, et al. AO/AAP consensus on prevention and management of peri-implant diseases and conditions: Summary report. J Periodontol. 2025;96:519-541.
- Schwarz F, Derks J, Monje A, Wang HL. Peri-implantitis. J Clin Periodontol. 2018;45(Suppl 20):S246-S266.
- Galarraga-Vinueza ME, Pagni S, Finkelman M, Schoenbaum T, Chambrone L. Prevalence, incidence, systemic, behavioral, and patient-related risk factors and indicators for peri-implant diseases: An AO/AAP systematic review and meta-analysis. J Periodontol. 2025;96:587-633.
- Kotsakis G, Olmedo D. Peri-implantitis is not periodontitis: Microbiome-biomaterial interactions. Periodontol 2000. 2021;86:231-240.
- Roccuzzo A, Imber JC, Marruganti C, Salvi GE, Ramieri G, Roccuzzo M. Clinical outcomes of dental implants in patients with and without history of periodontitis: A 20-year prospective study. J Clin Periodontol. 2022;49:1346-1356.
- Lin GH, Chan HL, Wang HL. The significance of keratinized mucosa on implant health: a systematic review. J Periodontol. 2013;84:1755-67.
- Lin GH, Lee E, Barootchi S, Rosen PS, Curtis D, Kan J, Wang HL. The influence of prosthetic designs on peri-implant bone loss: An AO/AAP systematic review and meta-analysis. J Periodontol. 2025;96:634-651.
- Guney Z, Altingoz SM, Has H, Serdar MA, Kurgan S. The impact of electronic cigarettes on peri-implant health: A systematic review and meta-analysis. J Dent. 2024;143:104883.
- Mojaver S, Zad A, Sarmiento H, Fiorellini JP. Efficacy of supportive peri-implant therapy in the management of peri-implant mucositis and peri-implantitis: A systematic review. J Am Dent Assoc. 2025;S0002-8177:00497-0.
- Ravidà A, Dias DR, Lemke R, Rosen PS, Bertolini MM. Efficacy of decontamination methods for biofilm removal from dental implant surfaces and reosseointegration: an AAP/AO systematicreview on peri-implant diseases and conditions. Int J Oral Maxillofac Implants. 2025;4:91-160.
- Maiorani C, Butera A, Pérez-Albacete Martínez C, et al. Effectiveness of erythritol-based air polishing and ultrasonic instrumentation with peek inserts in peri-implant maintenance: a randomized clinical trial including different prosthetic materials. Dent J (Basel). 2025;13:235.
- Tütüncüoğlu S, Cetinkaya BO, Pamuk F, et al. Clinical and biochemical evaluation of oral irrigation in patients with peri-implant mucositis: a randomized clinical trial. Clin Oral Investig. 2022;26:659-671.
- Maghsoudi P, Valkenburg C, Ter Gunne LP, van der Weijden FGA. Retrospective evaluation of peri-implant maintenance in patients with implant-supported fixed prostheses. Int J Dent. 2025;2025:9920951.
- Araújo TG, Moreira CS, Neme RA, Luan H, Bertolini M. Long-term implant maintenance: a systematic review of home and professional care strategies in supportive implant therapy. Braz Dent J. 2024;35:e246178.
- Salvi GE, Bosshardt DD, Lang NP, et al. Temporal sequence of hard and soft tissue healing around titanium dental implants. Periodontol 2000. 2015;68:135-52.
- Monje A, Barootchi S, Rosen PS, Wang HL. Surgical- and implant-related factors and onset/progression of peri-implant diseases: An AO/AAP systematic review. J Periodontol. 2025;96:542-561.
From Decisions in Dentistry. February/March 2026;12(1):14-19.
