
Revolutionizing Digital Impressions
Enhance your clinical efficiency with intraoral scanning technology.
Fundamental to numerous dental procedures, dental impressions are the negative replicas of oral structures.1 Conventional impression techniques have been used since the 18th century to register the three-dimensional (3D) geometry of dental tissues. However, volumetric changes of impression materials and expansion of dental stone lead to inaccuracies.2 Apart from these limitations, patient discomfort due to the taste and texture of material, increased gag reflex, managing patient movement, increased chairside time, and the need for additional steps — including pouring and trimming the model — make this technique less favorable.3
To overcome these limitations, intraoral scanners (IOS) were developed, transforming modern dental practice. The integration of IOS technology aligned with advancements in computer-aided design and manufacturing (CAD/CAM) systems offer numerous benefits to oral health professionals.4
IOS and CAD/CAM significantly reduce chairside time, allow effective communication with dental laboratories, and decrease total treatment time. The impression files can be stored and retrieved according to the user’s needs.2 Patients also prefer this technology due to increased comfort. Wismeijer et al5 compared the implant impressions using conventional techniques vs IOS and found that patients preferred IOS. According to a recent study, students preferred making digital impressions compared to the conventional approach due to ease of use and faster adaptability to the method.6
Mechanisms of Action
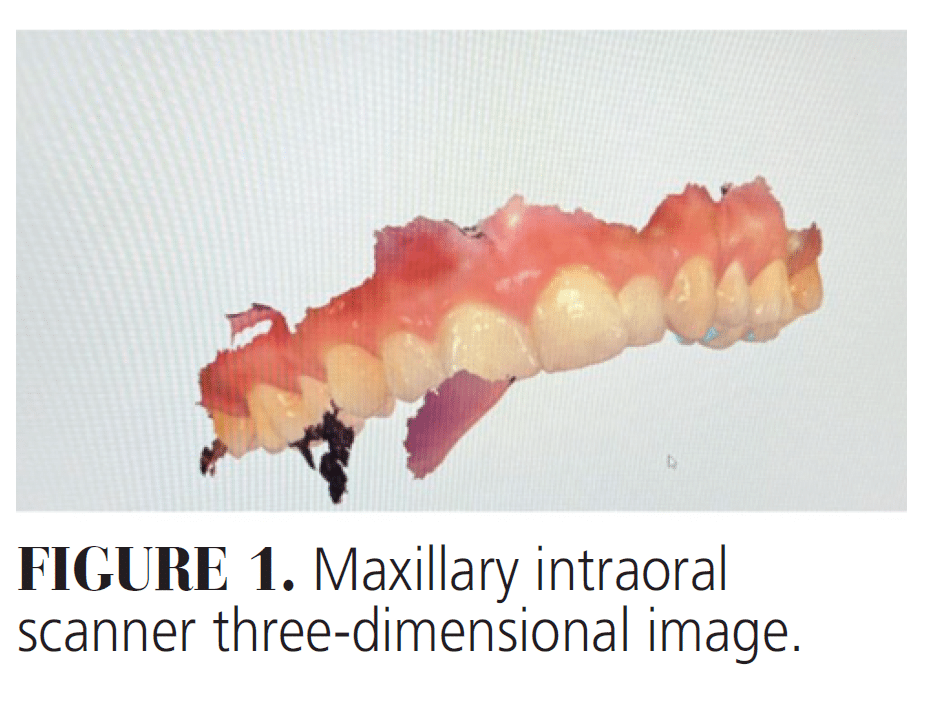 The IOS consists of a handheld camera (hardware), a computer, and software. The scanner operates on the principle of confocal laser scanning, also known as the “point-and-stitch reconstruction” technique. The process begins when light is directed toward an object and subsequently reflected. To capture a specific area, the scanning tip is moved back and forth until a complete image is obtained. The system selectively captures only the most focused light, discarding out-of-focus light. By passing the tip over the object multiple times, the entire image is converted from a single point to a series of points resulting in hundreds of segments, which are then superimposed and stitched together to form a comprehensive 3D image (Figure 1).7,8 The accuracy of structure capture is enhanced through advanced optics, including lenses and mirrors.
The IOS consists of a handheld camera (hardware), a computer, and software. The scanner operates on the principle of confocal laser scanning, also known as the “point-and-stitch reconstruction” technique. The process begins when light is directed toward an object and subsequently reflected. To capture a specific area, the scanning tip is moved back and forth until a complete image is obtained. The system selectively captures only the most focused light, discarding out-of-focus light. By passing the tip over the object multiple times, the entire image is converted from a single point to a series of points resulting in hundreds of segments, which are then superimposed and stitched together to form a comprehensive 3D image (Figure 1).7,8 The accuracy of structure capture is enhanced through advanced optics, including lenses and mirrors.
This scanning process is complemented by real-time data capture, allowing for immediate verification and modification of the impressions as needed. The open standard tessellation language (STL) or locked STL‐like format is the most widely used digital format for storing the images. It describes a succession of triangulated surfaces in which each triangle is defined by three points and a normal surface.2 Recent advancements have led to the development of wireless IOS, offering greater flexibility and ease of use during the scanning process.9
Clinical Applications
IOS can be conveniently used to evaluate dental wear and caries detection. A study reported that an IOS evaluates dental wear to the precision of 20 µm.10
IOS technology is used to measure arch width and length before and after treatment, as well as tooth size and any discrepancies between them. Few fixed orthodontic appliances are manufactured digitally, bypassing the complications of conventional techniques. Actual visualization of the treatment plan and the associated changes before starting treatment further helps increase patient acceptance. Digital impression technology has also impacted orthodontics through aligner therapy.11
IOS has transformed impression-taking approaches for fabricating multi-unit fixed partial dentures. This technology has gained worldwide adoption due to its time efficiency and enhanced patient-reported outcomes. Research demonstrates that digital impression methods are more time efficient and yield better patient-reported treatment outcomes compared to conventional techniques that use polyvinyl siloxane, alginate, and other impression materials.12 Furthermore, studies indicate that crowns fabricated from direct IOS impressions demonstrate superior marginal fit and dimensional accuracy when compared to those made using indirect digital impressions obtained through laboratory scanners.13
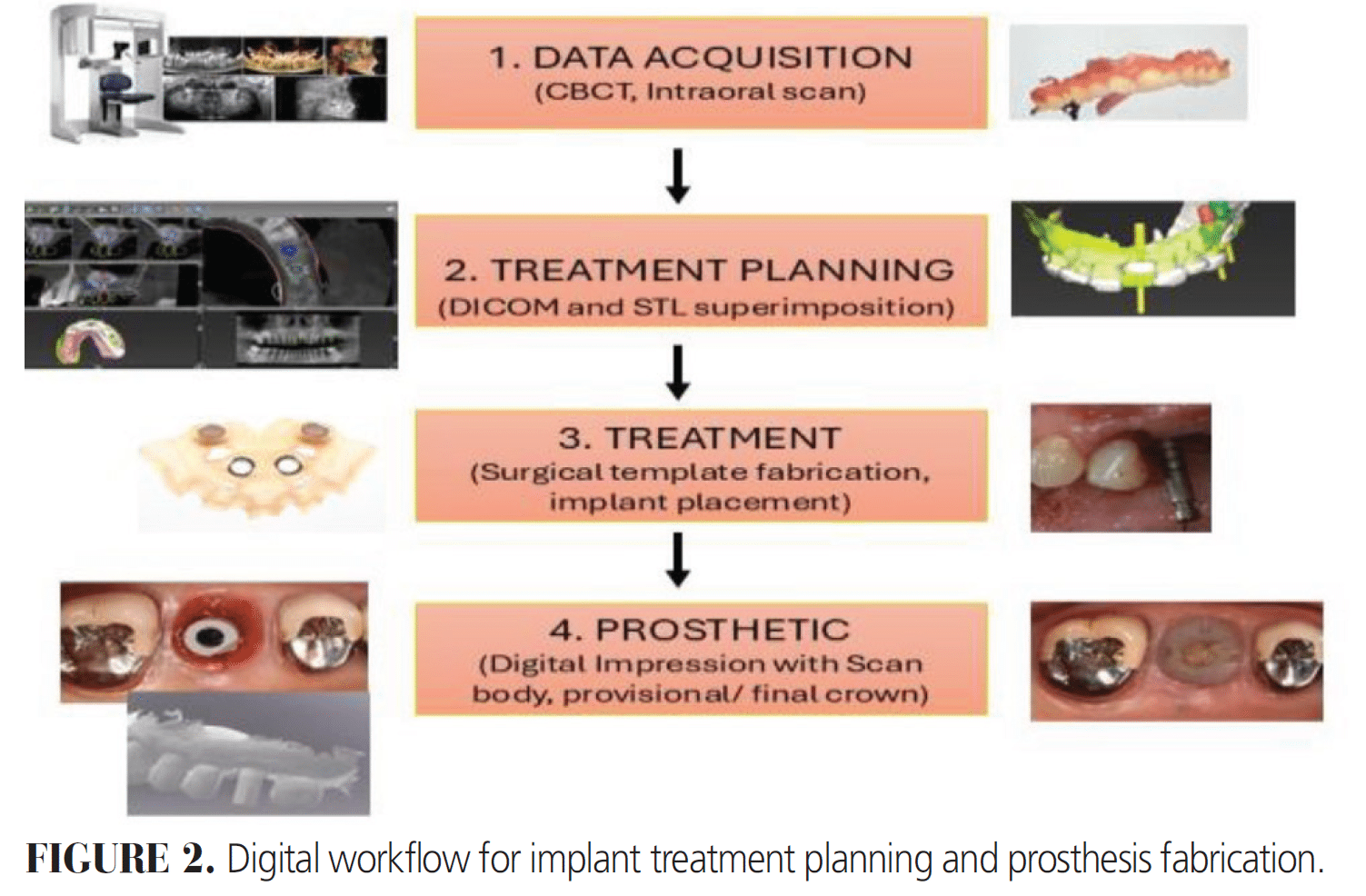
Digital impressions aid in implant treatment planning by recording accurate impressions and superimposition of these STL files with cone-beam files using digital software (Figure 2). In addition, implant positions can be recorded accurately, with intraoral scan bodies (ISBs) playing a crucial role (Figure 2). ISBs are typically made of polyetheretherketone and titanium. They consist of a scan region, body, and base, with dull, smooth, and opaque surfaces being easier to capture digitally. Michelinakis et al14 reported higher success rates for digital impressions on single implant sites and comparable accuracy to conventional techniques for fixed partial prostheses. However, challenges persist, particularly in edentulous patients in which conventional reference points are absent.
The accuracy of digital impressions is influenced by factors including room illumination, temperature, operator skill, and scanning technology. While digital workflows show promise, the variation in accuracy between partial- and complete-arch digital scanning remains a hurdle.14 Ongoing research and technological improvements continue to address the current limitations of digital impressions in implant dentistry, particularly in complex cases, aiming to enhance the accuracy and reliability of digital workflows across all clinical scenarios.15
Accuracy
A systematic review by Ma et al16 evaluated the trueness and precision (accuracy measurement) of IOS impressions in clinical settings. The study found that while IOS can achieve high accuracy, outcomes vary based on factors such as scanning strategies and operator expertise.
In full-arch restorations, IOS procedures require significantly less time than conventional methods, with comparable prosthetic survival rates and stable marginal bone levels. However, due to the size limitation of the IOS scanning tip, the scanner can only scan a segment of the arch at a time. Hundreds of segments are superimposed and stitched together to generate the final 3D model. During this stitching process, superimposing error accumulates and creates inaccuracy, especially in long-span or full-arch cases.8
The characteristics of ISBs are crucial to successful outcomes. Gehrke et al17 highlighted that the precision of virtual scans depends on ISB design, material, and surface properties. However, limited reports discuss these features, indicating a need for further research. The proficiency of the clinician using the IOS significantly impacts the quality of the digital impression. Proper training and experience are essential to minimize errors during scanning.
Patient-specific variables, such as oral anatomy and the presence of saliva, can influence scan accuracy. Managing these factors is vital to obtain precise digital impressions. Differences among IOS devices, including scanning technology and software algorithms, can lead to variations in accuracy. Selecting appropriate equipment is key to optimal results.17,18
Disadvantages of Intraoral Scanners
The IOS, despite its many advantages, comes with certain limitations. First, the IOS requires additional training and may pose a steep learning curve for some.19 Additionally, the IOS is costly, which may pose financial challenges to some practices.19,20
Some aspects of use are also daunting. Detecting finish lines is particularly challenging when they are situated subgingivally or when gingival bleeding is present.19,20 The risk of superimposition error in full-arch cases is high.8 Finally patient privacy can be compromised during scan acquisition or laboratory file transfer procedures if proper security protocols are not rigorously implemented and maintained.20
Case Report
A 30-year-old man reported to a dental school setting for #13 implant placement. Upon evaluation, #12 implant, which had been placed several years prior, presented with severe bone loss (Figure 3A and B) and was diagnosed with peri-implantitis. The treatment plan involved extraction/ridge preservation for #13 and removal of #12 implant. However, the patient wanted to save implant #12 and thus a peri-implant debridement with guided bone regeneration was planned.
Three months after the procedure, a cone beam was taken for #13 implant placement that showed sinus pneumatization and progression of bone loss in the #12 implant site (Figure 4). The #12 implant was removed and a sinus augmentation via double window approach was done due to the presence of a sinus septa (Figure 5A-C).

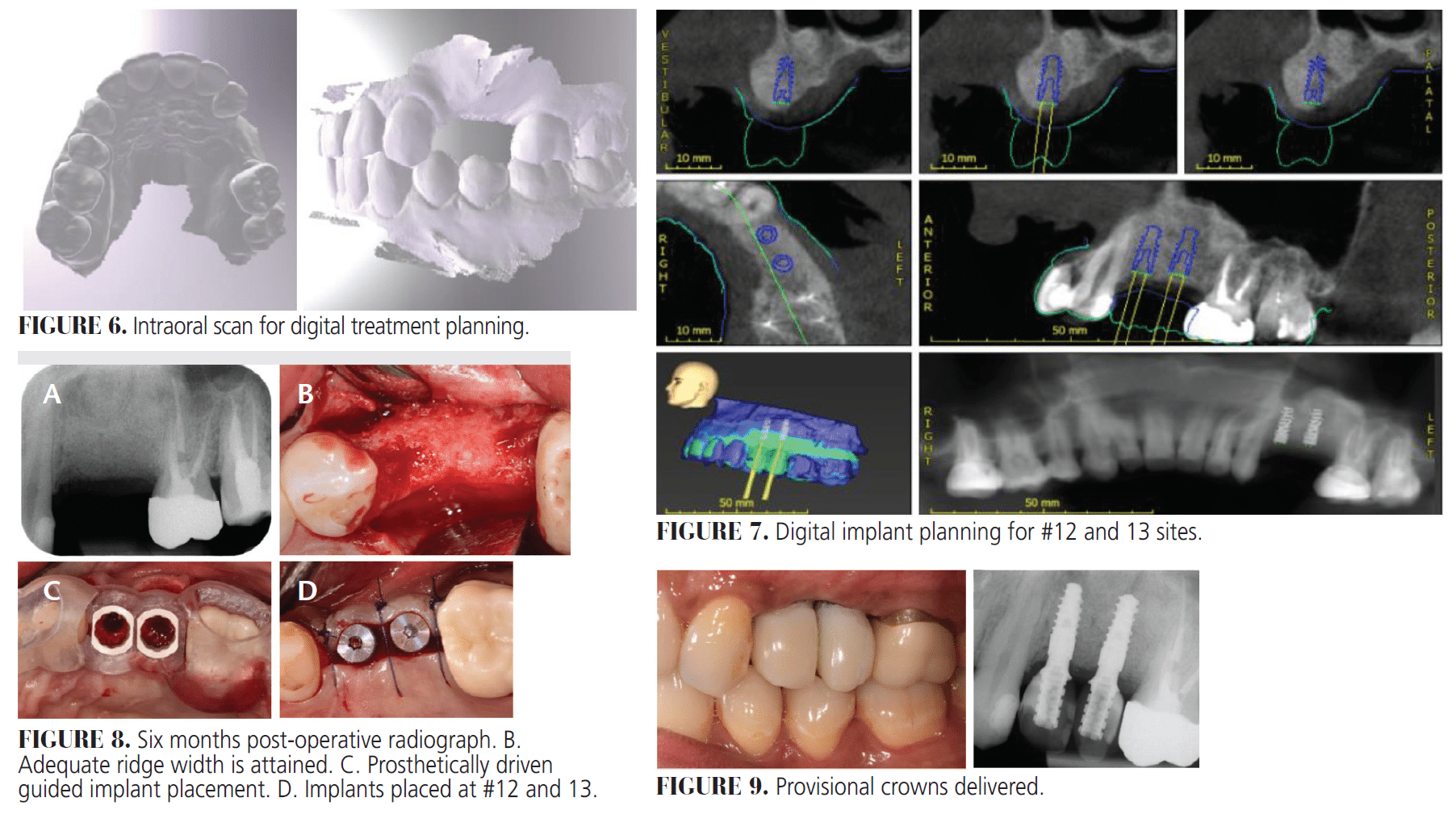
Six months later, another cone beam was taken along with an IOS for digital treatment planning (Figure 6), and a guided implant placement was performed for #12 and 13 sites (Figure 7).
Three months after the placement of the implant, an IOS was taken, and provisional crowns were delivered. Six months following the surgery, adequate ridge width had been attained (Figures 8 and 9). The procedure was well accepted by the patient with minimal complications. IOS and digital treatment planning made this complex procedure seamless and less time consuming.
Conclusions
Digital IOS technology has revolutionized dentistry, bringing significant advancements to the field. This innovation has not only enhanced patient experience but also presents numerous advantages over traditional impression techniques. The introduction of digital models and workflows has dramatically reduced the physical space required for storing plaster models, streamlining dental practices. The applications of this technology span across various areas of dentistry, demonstrating its versatility and importance. From orthodontics to restorative dentistry, digital scanning has found its place across multiple specialties, improving accuracy and efficiency.
Despite its many benefits, technology does face some limitations. The primary constraint is the high cost associated with purchasing the equipment. This financial barrier has restricted widespread adoption, particularly among smaller practices. Nevertheless, as technology continues to evolve and become more accessible, its impact on dental practices and patient care is expected to grow, further solidifying its role in modern dentistry.
References
- Punj A, Bompolaki D, Garaicoa J. Dental impression materials and techniques. Dent Clin N Am. 2017;61:779-796.
- Richert R, Goujat A, Venet L, et al. Intraoral scanner technologies: a review to make a successful impression. J Healthc Eng. 2017;2017:8427595.
- D’Ambrosio F, Giordano F, Sangiovanni G, Di Palo MP, Amato M. Conventional versus digital dental impression techniques: what is the future? An umbrella review. Prosthesis. 2023;5:851-875.
- Duret FJ. Toward a new symbolism in the fabrication of prosthetic design. Cah Prothese. 1985;13:65-71.
- Wismeijer D, Mans R, Van Genuchten M, Reijers HA. Patients’ preferences when comparing analogue implant impressions using a polyether impression material versus digital impressions (Intraoral Scan) of dental implants. Clin Oral Implants Res. 2013;25:1113–1118.
- Lee SJ, Gallucci GO. Digital vs. conventional implant impressions: efficiency outcomes. Clin Oral Implants Res. 2013;24:111-115.
- Hwang HH, Chou C, Chen Y, Yao CJ. An overview of digital intraoral scanners: past, present and future- from an orthodontic perspective. Taiwanese Journal of Orthodontics. 2018;30(3):3
- Li J, Chen Z, Nava P, Yang S, Calatrava J, Wang HL. Calibrated intraoral scan protocol (CISP) for full‐arch implant impressions: An in vitro comparison to conventional impression, intraoral scan, and intraoral scan with scan‐aid. Clin Implant Dent Relat Res. 2024;26:879-888
- Dhull KS, Nagar R, Mathur P, et al. Intraoral scanners: mechanism, applications, advantages, and limitations. J Pharm Bioallied Sci. 2024;16:S1929-1931.
- Kühne C, Lohbauer U, Raith S, Reich S. Measurement of tooth wear by means of digital impressions: an in-vitro evaluation of three intraoral scanning systems. Appl Sci. 2021;11:5161.
- Christopoulou I, Kaklamanos EG, Makrygiannakis MA, Bitsanis I, Perlea P, Tsolakis AI. Intraoral scanners in orthodontics: a critical review. Int J Environ Res Public Health. 2022;19:1407.
- Siqueira R, Galli M, Chen Z, et al. Intraoral scanning reduces procedure time and improves patient comfort in fixed prosthodontics and implant dentistry: a systematic review. Clin Oral Investig. 2021;1:1-5.
- Seshan RR, Karthikeyan HR, Rajan RM, Rajakumaran A, Varadan P, Gopal R. Comparative evaluation of the marginal fit of computer-aided design-computer aided manufacturing fabricated crowns from direct and indirect digital impression: A systematic review. J Conserv Dent Endod. 2024;27:140-145.
- Michelinakis G, Apostolakis D, Kamposiora P, Papavasiliou G, Özcan M. The direct digital workflow in fixed implant prosthodontics: a narrative review. BMC Oral Health. 2021;21:1-24.
- Marques S, Ribeiro P, Falcão C, et al. Digital impressions in implant dentistry: A Literature Review. Int J Environ Res Public Health. 2021;18:1020.
- Ma J, Zhang B, Song H, Wu D, Song T. Accuracy of digital implant impressions obtained using intraoral scanners: a systematic review and meta-analysis of in vivo studies. Int J Implant Dent. 2023;9:48.
- Gehrke P, Rashidpour M, Sader R, Weigl P. A systematic review of factors impacting intraoral scanning accuracy in implant dentistry with emphasis on scan bodies. Int J Implant Dent. 2024;10:20.
- Alkadi L. A comprehensive review of factors that influence the accuracy of intraoral scanners. Diagnostics. 2023;13:3291.
- Mangano F, Gandolfi A, Luongo G, Logozzo S. Intraoral scanners in dentistry: a review of the current literature. BMC Oral Health. 2017;17:149.
- Dhull KS, Nagar R, Mathur P, et al. Intraoral scanners: Mechanism, applications, advantages, and limitations. J Pharm Bioallied Sci. 2024;16(Suppl 3):S1929-1931.
From Decisions in Dentistry. October/November 2025;11(5):6-10.
