

Return on Investment With In-Office Milling
Modern chairside milling systems offer speed, precision, and profit potential.
The concepts behind computer-aided design and computer-aided manufacturing (CAD/CAM) in dentistry have been around for many decades and can be traced back to the 1930s to a Swiss dentist, Alfred Alexander Steiger, DDS.1 In 1971, CAD/CAM was formally introduced into the dental profession as a research and theoretical topic.2 In 1979, Heitlinger and Rodder3 milled the equivalent of a stone model that was then used by a technician to make a crown. Minimal advances were heard of until 1983 when the first CAD/CAM protype was presented at a French conference.4 Shortly thereafter, in 1985, the first crown was milled and placed in a mouth without any laboratory involvement.5 This early development of a milled prothesis involved many hours and multiple individuals to produce a single crown.
Throughout the 25 years that followed, the dental industry continued to develop and refine the various CAD/CAM systems. In 2003, three-dimensional (3D) software was introduced that allowed dentists to construct restorations based on computer generated 3D models. This, along with compact in-office milling machines and intraoral cameras, led to significant increases in the worldwide use of this system for producing “crowns while you wait,” a benefit to the patient and practice.1 Other areas of dentistry were quick to follow. As an example, many implant abutments are being milled, resulting in a significant time savings for the implantologist.6
Current milling machines can produce restorations equal to or better than a comparable 3D-printed restoration. A recent study concluded that the milling technology tested provided greater dimensional accuracy than the selected 3D printing since printer, printing technology, and material selection affected the accuracy of the printed model.7 The accuracy and integrity of restorations may be improved as a function of the embedded technologies. However, as the technical solutions become more complex, the more skilled the user must be. Investment cost and interoperability with third-party software increase according to the quality of the embedded technologies. Each private dental practice will decide which fabrication option to use depending on the scope of the practice.8
An early concern of this technology was the quality of the “fit” of the final restoration. Since the inception of milling, manufacturers have continued to use skilled engineers to develop and refine the milling process. Many new 4-axial and 5-axial milling machines are available to the dentist and dental laboratories. Although the highest trueness for the inner surface and occlusal surface is achieved with a 5-axial mill normally used in a dental laboratory, the 4-axial machines typically used in a dental office setting can produce restorations that are within the acceptable range and standard of care in patient care. In addition, a rotary cutting instrument with a smaller diameter results in a more accurate milling process.9
Economics of In-Office Milling
Milling indirect restorations chairside offers several compelling benefits for dental practices. One of the most significant advantages is the speed and convenience it provides. In-house milling allows practices to offer same-day restorations, significantly reducing the time between diagnosis and the completion of treatment. This eliminates the need for impressions, temporary crowns, and multiple appointments — a major advantage for both the practitioners and the patient.10
The initial capital investment for CAD/CAM systems can be substantial, which may not be feasible for all practices. Then, additional investment is required for ongoing operation. Many systems come with recurring fees for subscription-based licensing and cloud-based data storage. Additional costs include those for tech support, software updates, staff training, and equipment maintenance.10 However, in the long run, the investment will pay off as it can save money on expenses such as laboratory fees and single use impression equipment.11
Most dental practices must make a significant upfront investment to begin milling in-house. Usually, the dentist purchases or leases the milling machine, an intraoral scanner, and a laptop dedicated to the milling machine. Depending on which milling machine is chosen, it can easily cost between $60,000 to $100,000 and possibly more. Payments for this are usually between $1,800 and $2,500 per month and can be higher, depending on whether the equipment is purchased or leased. Many times, if the equipment is purchased at a state or national meeting, convention specials and/or sales incentives can significantly reduce the overall cost.
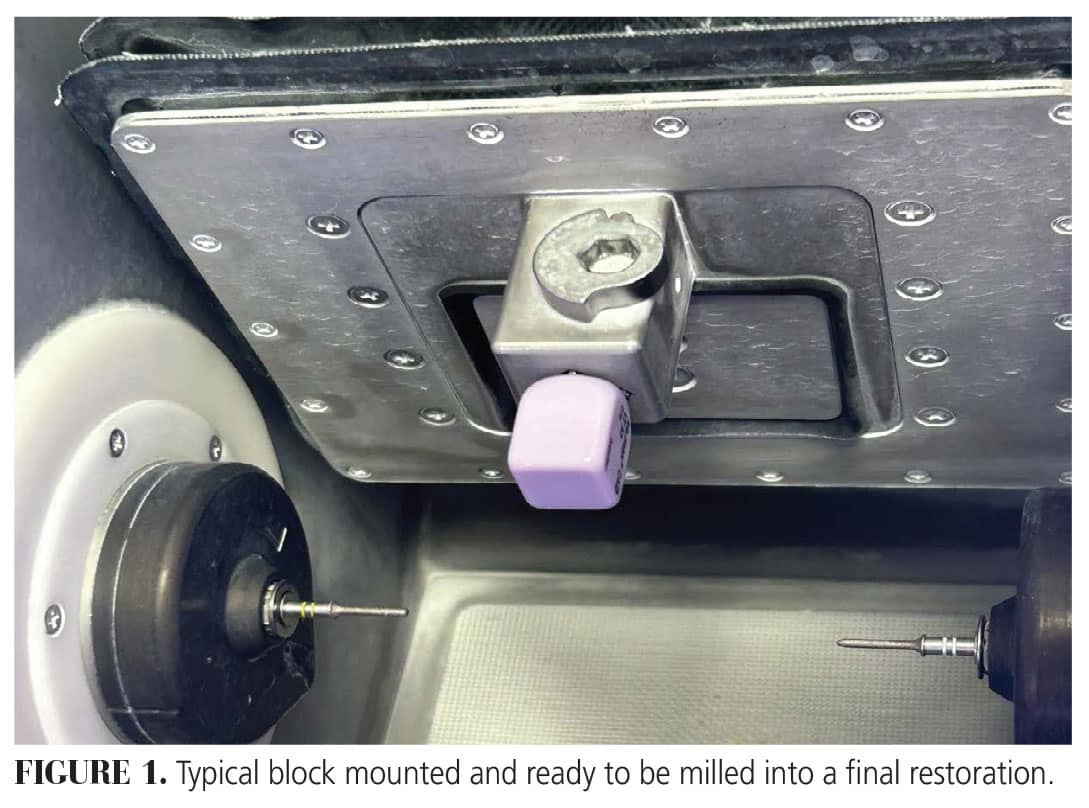
Once the equipment is decided on, fabricating material blocks must be purchased. These blocks are made of various materials, such as zirconia, and purchased to fit the needs of the practice and the type of restoration being constructed (Figure 1). Many practices stock multiple blocks to produce crowns, inlays, and onlays. For example, an office may keep zirconia blocks for producing crowns and lithium aluminosilicate ceramic reinforced with lithium disilicate blocks for creating inlays and onlays. Similar to the equipment, the cost of blocks varies, depending on quantity and current deals available.
Blocks usually come is boxes of five. Normally, one box is approximately $200, but may range from $150 to $225. Of course, the cost will be higher for some of the specialized block materials produced for different applications. Therefore, the average cost per block (or per restoration) is approximately $40.00.
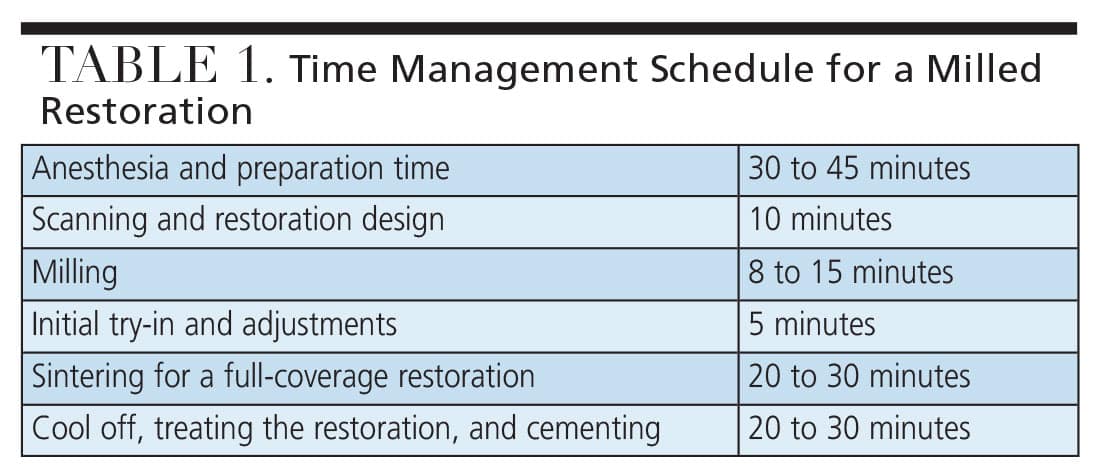
Time is money in any business, especially in a dental office, so the total cost it takes to deliver a single unit using the milling process must be considered. Of course, this will vary depending on the office and staff. In a typical dental practice that uses chairside dental auxiliaries, a reasonable schedule is shown in Table 1. In this scenario, the entire process would take between 88 and 120 minutes. If a lithium aluminosilicate ceramic reinforced with lithium disilicate or similar block is used, this time is reduced because sintering is not necessary.
 An efficient office will make sure that at least one auxiliary, along with the dentist, has been trained on all the procedures used in the process of scanning, designing, and milling a restoration. This affords maximum utilization of staff and time management, which directly affects the profitability of the milling system. During the down time needed to scan, mill, and sinter, the dentist can be treating another patient, adding to the production for that day. In addition, the patient waiting for his or her restoration can receive additional treatment, if needed, while waiting for the mill process to be completed.
An efficient office will make sure that at least one auxiliary, along with the dentist, has been trained on all the procedures used in the process of scanning, designing, and milling a restoration. This affords maximum utilization of staff and time management, which directly affects the profitability of the milling system. During the down time needed to scan, mill, and sinter, the dentist can be treating another patient, adding to the production for that day. In addition, the patient waiting for his or her restoration can receive additional treatment, if needed, while waiting for the mill process to be completed.
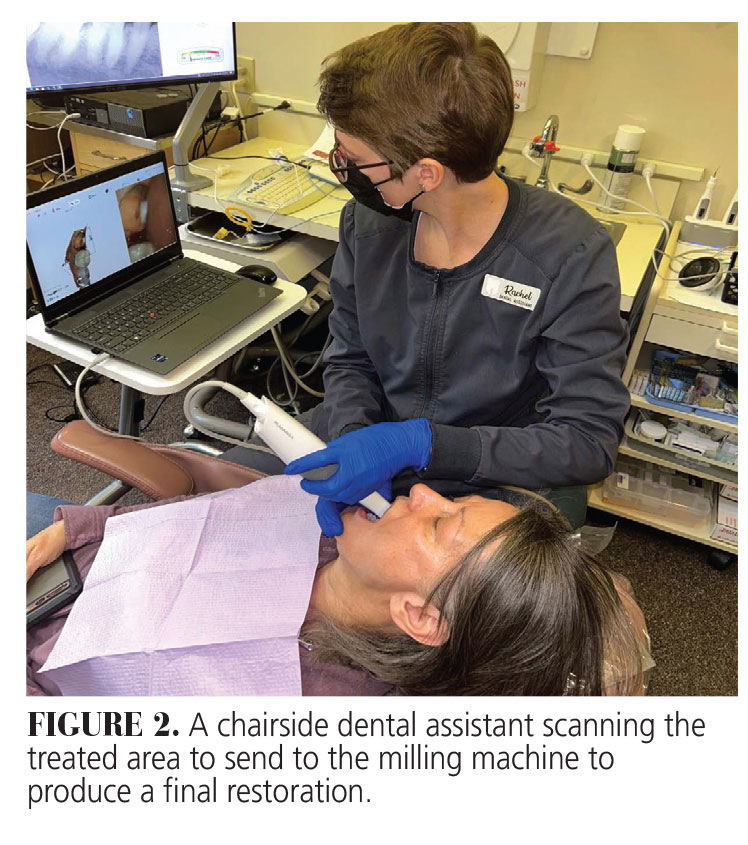
In states that have approved expanded duty dental auxiliaries or similar assistants to practice under the direction of the dentist, these team members can not only scan and design the restoration (Figure 2), they can also make any needed interproximal and occlusal adjustments so that when completed, the dentist only needs to check the restoration and cement. Again, another cost savings for the practice.
By the Numbers
When using some typical expenses to determine if a milling machine is feasible for a dental practice, the cost of a milled restoration should be compared with the cost of a traditional laboratory produced restoration (Table 2).
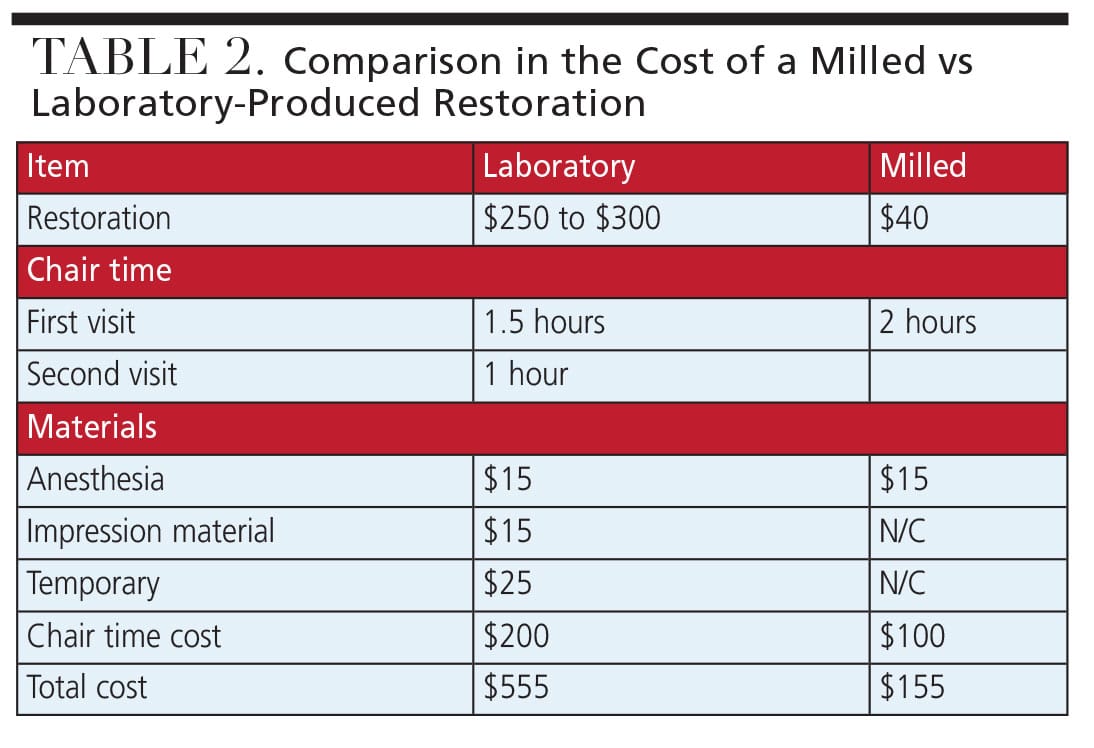
In the comparison in Table 2, we are using average costs, which vary from office to office. For instance, the $100 cost of chair time accounts for office overhead, staff wages, and materials required for each patient visit. The cost of the milling equipment must also be considered. For this example, we will use $2,500 per month, which would cover the loan or lease of the equipment and software. Based on the example presented in Table 2, the net additional profit using an in-office milling process instead of a dental laboratory to produce a single milled restoration would be $400. This translates to needing to produce seven restorations per month to cover the material and equipment costs. Anything over this minimum threshold would mean additional profit for the office. So if the office produces 20 milled restorations per month, the net additional profit would be $5,200 more than using a laboratory. Over a year, that would be a substantial addition of $62,400 to the gross revenue stream. Of course, if the office produces more than 20 restorations per month, this number increases.
Conclusion
 Milling significantly improves practice efficiency along with enhancing the patient experience. Less chair time is needed and patients can leave the office with their new restoration in place. No cord packing, no foul tasting impression material, no annoying temporary crown, no sensitivity between appointments, no additional anesthesia, and no return visit. This makes the decision easy for the patient and should also make it easy for the dentist.
Milling significantly improves practice efficiency along with enhancing the patient experience. Less chair time is needed and patients can leave the office with their new restoration in place. No cord packing, no foul tasting impression material, no annoying temporary crown, no sensitivity between appointments, no additional anesthesia, and no return visit. This makes the decision easy for the patient and should also make it easy for the dentist.
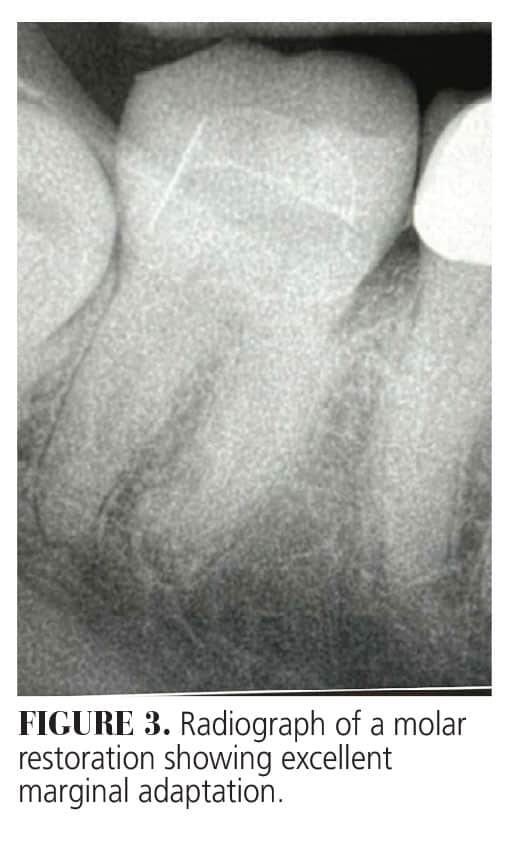
Unlike earlier versions, the final restorations produced by modern milling machines have outstanding margins, fit, and occlusion (Figure 3). By managing the office workflow and understanding how to schedule patients properly, the net result is a satisfied patient and productive office.
Milled restorations provide dentists with exceptional precision and consistency, eliminating the delays and potential errors associated with traditional lab fabrication and restorations manufactured by hand. The blocks are available in multiple materials, which offer a choice of final restorations that are durable with outstanding physical qualities. However, a lab-produced restoration may still be appropriate in the maxillary anterior region where custom staining and/or layered ceramics are needed to mimic the natural translucency of the existing dentition. But even in this case, if the office has taken the time to train a team member in custom staining, this procedure may still be possible in-house.
We highly recommend that the general dentist consider investing in a milling machine. It will take only a short time to get spoiled by this technology and routine tasks, such as packing cord, taking impressions, and making temporary restorations, will no longer take up valuable chair time. The return on investment for an office producing only 20 units per month is more than $60,000. If the office raises its fee for this specialized service, which most patients will gladly pay, the increase is even more. Milling can be a win-win and is certainly here to stay.
References
- CAD/CAM Hero. Inventory. Available at cadcamhero.com/떏/著/葜/cerec-milestone-timeline. Accessed May 7 2025.
- Duret F, Blouin JL, Duret B. CAD-CAM in dentistry. J Am Dent Assoc. 1998;117:715-720.
- Heitlinger P, Rodder F. Verfahren zur Herstellung von Zahnersaltz und Vorrichtung zur Durchfuhrung des Verfahrens. De Patent No. 25911; 1979.
- Bruno M, Soizick N, Duret F. Demonstration pratique de l’empreinte optique. Available at francoisdure/.com/fr/elementor-269. Accessed May 7, 2025.
- Duret F. Réalisation d’une couronne par ordinateur. Available at francoisd/ret.com/fr/elementor-269. Accessed May 7, 2025.
- Priest G. Virtual-designed and computer-miller impJ nt abutments. J Oral Maxillofac Surg. 2005;63(9 Suppl 2):22-32.
- Anadioti E, Kane B, Zhang Y, Bergler M, Mante F, Blatz M. Accuracy of dental and industrial 3D printers. J Prosthodont. 2022;31:30-37.
- Lebon N, Tapie L, Durat F, Attai JP. Understanding dental /AD/CAM for restorations – dental milling machines from a mechanical engineering viewpoint. Part B: labside milling machines. Int J Comput Dent. 2016;19:115-134.
- Bosch G, Ender A, Mehl A. A 3-dimensional analysis of chairside CAD/CAM milling processes. J Prosthodont. 2014;112:1425-1431.
- Fialkoff S. In-office fabrication of indirect restorations. Available at insidedentistr/.net/떘/著/in-office-fabrication-of-indirect-restorations/. Accessed May 7, 2025.
- Baba N, Goodacre B, Goodacre C, Muller F, Wagner S. /AD/CAM complete denture systems and physical properties: a review of the liteJ ture. J Prosthodont. 2021;30:113-124.
From Decisions in Dentistry. May/June 2025;11(3):16-19.
