
Prevent Peri-Implant Mucositis
Taking an individualized approach to prevention and therapy can improve outcomes when treating this precursor to peri-implantitis.
Taking an individualized approach to prevention and therapy can improve outcomes when treating this precursor to peri-implantitis.

Infections around dental implants have been referred to by several names. Peri-implantitis and peri-implant disease are nonspecific terms used to describe infection or inflammation in the soft and hard tissue around a dental implant. Reportedly, such inflammation occurs in 48% of implant cases, even 14 years post-surgery.1 Considering the scope of the problem, publications have called for the use of specific terminology, identification and action when dental implants present with infection and inflammation.2,3 Peri-implant mucositis occurs when inflammation is present in the mucosa surrounding the dental implant with no sign of supporting bone loss, as it most often precedes bone loss.4 True peri-implantitis occurs when inflammation spreads from the soft tissue to the underlying bone, resulting in bone loss. Considering the effects of oral inflammation on the systemic health, dentists serve important patient needs by arresting peri-implant mucositis, halting the disease process.5

Peri-implantitis mucositis and gingivitis share similar clinical presentations. In both conditions, underlying vessels dilate and become engorged with blood and the soft tissue color changes from pale pink to deep red or cyanotic hue. Interdental papillae take on blunted appearance, and the gingival margin may present as rolled or thickened; this is a departure from the healthy, knife-edged gingival margin (Figure 1A and Figure 1B). Bleeding on probing or spontaneous bleeding is often present. When bone loss is present around a dental implant, the condition is peri-implantitis — just as when bone loss is present around a tooth, the condition is periodontitis.
Peri-implant mucositis has a very similar clinical presentation to peri-implantitis (Figure 2A and Figure 2B). Table 1 provides a comparison between peri-implant mucositis and peri-implantitis.6 When differentiating between peri-implant mucositis and peri-implantitis, assessing inflammation around a dental implant requires a combination of diagnostic tools, including radiography and probing. In diagnosing peri-implant mucositis, peri-implant inflammation must first be identified, followed by the use of radiography to rule out bone loss.7 Radiographs of a patient with peri-implant mucositis will not show any radiolucent areas surrounding the implant.

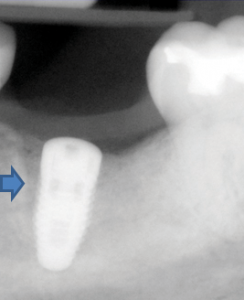
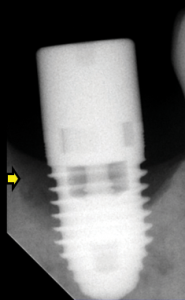
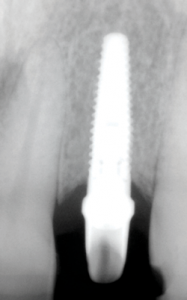
A baseline radiograph should be used as a reference when identifying bone loss. Unfortunately, such images are often not available. An option is to use a threshold vertical distance of 2 mm from the expected marginal bone level following the expected post-placement related remodeling (Figure 3A through Figure 3C). Subtraction programs are available to define radiographic changes in digital images. In the absence of such programs, radiographs taken perpendicular to the implant showing clear thread demarcation can be compared across time points to identify bone loss.
key takeaways
- Peri-implant mucositis occurs when inflammation is present in the mucosa surrounding the dental implant with no sign of supporting bone loss, as it most often precedes the bone loss seen in peri-implantitis.4
- In order to identify peri-implant mucositis, peri-implant inflammation must first be identified, followed by the use of radiography to rule out bone loss.7
- Probing is a necessary diagnostic tool in assessing periodontal or peri-implant health. Probing depth is defined as the distance from the base of the sulcus/pocket around the implant to the crest of the soft tissue.
- Because identifying increasing probing depths can be helpful to early diagnosis, a comparison to baseline probing (when the final restoration was placed) is useful.
- Prospective studies demonstrate that patients with generalized aggressive periodontitis are more susceptible to peri-implantitis. Based on these and other studies, a history of periodontitis warrants more vigilant screening for peri-implant mucositis.25
- Because peri-implantitis can progress faster than typical periodontitis, prevention and early detection and treatment of peri-implant mucositis and peri-implantitis are seminal to optimal outcomes.
DIAGNOSTIC METHODS

The probe is a key instrument when assessing periodontal health. Probing with light force (25N) protects soft tissue adjacent to the implant. Care must be taken when using metal probes to prevent scratching the implant surface; choosing plastic periodontal probes can help in this regard. Scratches will yield irregularities along the implant that provide surfaces upon which plaque can accumulate. Probing depth is defined as the distance from the base of the sulcus/pocket around the implant to the crest of the soft tissue. Because identifying increasing probing depths can be helpful to early diagnosis, a comparison to baseline probing (when the final restoration was placed) is useful. As a rule, clinical examination probing depths greater than 5 mm are associated with peri-implant mucositis. Bleeding and suppuration indicate the need for further evaluation to rule out peri-implantitis.7 A clinical finding of bleeding on probing or suppuration, however, cannot be used to distinguish between peri-implant mucositis and peri-implantitis. These findings suggest the need for further diagnostics, as peri-implantitis is defined as progressive bone loss confirmed by probing or radiography — or both.

Peri-implant disease diagnostics are an exciting and quickly expanding area of study. A recent meta-analysis reported that peri-implant crevicular fluid is useful in identifying infection.8 Crevicular fluid is a serum filtrate that seeps through the gingival epithelium in the crevice or sulcus surrounding teeth and dental implants alike. Fluid volume increases with inflammation, additionally, high molecular weight elements cells, such as neutrophils and leukocytes, are present alongside the normal electrolytes, organic compounds and debris. Crevicular fluid is useful in disease identification because in disease states it contains characteristic inflammatory mediators, such as interleukin (IL)-1β and tumor necrosis factor (TNF)-α. These mediators occur in different concentrations in healthy tissue compared to tissue with peri-implant mucositis versus tissue with peri-implant bone loss. Because crevicular fluid is a filtrate of serum, individuals with systemic diseases involving inflammation, such as rheumatoid arthritis, show a similar upregulation of these inflammatory mediators in serum and crevicular fluid. Investigating how this baseline increase in circulating inflammatory mediators may predispose an individual to oral inflammation such as peri-implant mucositis, and dissecting between an uptick in these mediators caused by local factors versus systemic ones, continue to be a hotly researched subjects.
As personalized medicine broadens its profile across health care, another expanding area of research involves identifying genetic markers that predispose certain individials for peri-implantitis. Although it is not ready for chairside application, genetic marker identification holds promise.9 Broader understanding of underlying immunologic inflammatory profiles could be helpful in developing treatment strategies specific to a particular individual’s immunologic “soft spots.”
Culture, direct microscopy immunoserological identification, and nucleic acid-based methods may be performed to ascertain the microbial species responsible for triggering inflammation. Clinical oral microbiology laboratories may employ one or a combination of these methods, depending on the pathogens that need to be identified. Rarely does one detection method prove optimal for all situations.
PATHOGENESIS
Tissues surrounding an implant are not contiguous with a periodontal ligament as they are around a natural tooth. Despite this difference in attachment, peri-implant mucositis is histologically and anatomically similar to gingivitis in that both are reversible conditions. Furthermore, the plaque biofilm that triggers gingivitis also initiates peri-implant mucositis. Similar to natural teeth following a dental prophylaxis, the exposed titanium surface of a newly placed dental implant accumulates sticky glycoproteins and forms a salivary pellicle. Microbial colonization begins and develops into a biofilm.10 The biofilm development is also similar between these two conditions. Initial colonizers are Gram-positive aerobic coccus bacteria, but as the biofilm develops, there is a shift toward Gram-negative anaerobic bacteria. Unlike gingivitis around natural teeth in the pathogenesis of periodontitis, studies have suggested that Staphylococcus species not normally found proximate to natural teeth may play a role in peri-implant disease.1,11
In peri-implant mucositis, just as in gingivitis, bacterial biofilm triggers a similar host immune response. In both conditions, as soft tissue inflammation progresses, blood vessels adjacent to the pocket epithelium become enlarged and more permeable. Increased vessel permeability causes neutrophils to migrate out of the vessels into the pocket area. Collagen surrounding the blood vessels is broken down. Lymphocytes and macrophages accumulate in the newly created space. Fibroblasts show pathologic changes, and collagen is lost apical to the pocket epithelium. Histologic evaluation shows the underlying connective tissue adjacent to the pocket epithelium exhibits more B-lymphocytes, which subsequently transform into plasma cells.12 The ever-deepening pocket creates a reservoir to retain bacteria, and pH and redox characteristics provide favorable conditions. The products of these pathogens further challenge the host immune defense, as underlying connective tissue continues to hydrolyze, deepening the pocket in an apical direction. At this point, the condition has progressed from peri-implant mucositis to peri-implantitis and supporting bone is also broken down.3,13
To further underscore the importance of prevention and early detection in implant cases, the reported rate at which inflammation spreads to the supporting bone is faster in peri-implantitis compared to periodontitis.14 This is due to structural differences between periodontal and peri-implant tissues. Unlike natural teeth, dental implants do not have cementum or Sharpey’s fibers and are not bounded by a periodontal ligament. Bone contacts the implant surface directly in an osseointegrated implant. As such, the pathway of inflammation goes directly from the soft tissue to the hard tissue without first encountering ligamentous structures or cementum. In both conditions, the inflammatory process eventually reaches the alveolar bone crest and osteoclastic bone resorption occurs. The inflammatory cells activate cytokines such as IL-1, TNF-α, and IL-6.15 It is important to note that these very same inflammatory mediators are present locally in the gingival crevicular fluid, highlighting its critical role in diagnosis.
Until such time that adequate research enables immunologic and inflammatory mediators to be identified and controlled further upstream, a dentist’s key goal is to disrupt the trigger that “kickstarts” this inflammatory cascade locally around the implant. Just as the primary objective to treat gingivitis is to remove plaque biofilm from the tooth surface, so, too, it is in peri-implant mucositis. And just as the prevention of gingivitis stems from interrupting biofilm accumulation, identifying and removing plaque-retentive sites around dental implants are crucial steps in preventing peri-implant mucositis.
ORAL HYGIENE INSTRUCTION
Peri-implant mucositis is reversible by removing the plaque biofilm that triggers the inflammatory cascade.16 Any factors that contribute to poor plaque control or plaque retention increase the risk for peri-implant mucositis. Patients’ lack of compliance with oral hygiene is the most obvious cause, but further investigation is warranted. Mental or physical disabilities may preclude adequate self-care. In the case of physical disability, providing mechanical toothbrush recommendations may be helpful.17,18 With more compromised patients, providing instructions to the caregiver or case manager may be useful.
There is a significant evidence base of controlled, prospective studies that provide information about the efficacy of various dentifrices and mouthrinses around implants.19 Judging from the similar pathogenesis between gingivitis and peri-implant mucositis, toothpastes containing either stannous fluoride or triclosan with a copolymer have statistically significant antiplaque and antigingivitis activity.20 Similarly, investigation into stannous fluoride-sodium hexametaphosphate toothpaste showed a high level of antiplaque and antigingivitis activity.21,22 That said, in some situations fluoride has been shown to cause corrosion of implant surfaces.23
A previous history of periodontitis is also associated with peri-implant inflammation. Compared to control patients, soft tissues isolated from patients with a history of periodontal disease show greater periopathogens and superinfecting bacteria.24 Prospective studies demonstrate that patients with generalized aggressive periodontitis are more susceptible to peri-implantitis. Based on these and other studies, a history of periodontitis warrants more vigilant screening for peri-implant mucositis.25
RISK ASSESSMENT
Patients presenting with conditions or habits, such as smoking, that inhibit the body’s mechanisms to fight off bacterial insult are also at increased risk of peri-implantitis.26,27 Conditions that contribute to systemic inflammation can exacerbate local inflammation around implants. Among these, diabetes is one of the more familiar maladies, as poor glycemic control appears to aggravate peri-implant disease. This is likely because elevated blood glucose impairs host defenses and neutrophilic functions.28 As such, when the initial plaque biofilm insult occurs, the host is less capable of maintaining homeostasis. Similarly, genetic factors such as the IL-1 gene polymorphism may be risk factors,22 but the research is unclear.27 Chronic inflammatory diseases, such as rheumatoid arthritis, that exacerbate local inflammation triggered by biofilm insult, appear to be risk factors in peri-implantitis.27
Broken or poorly designed prosthetics or substandard nearby restorations may interfere with oral hygiene measures. One way to identify a plaque-retentive restoration is to look for areas that catch impression material while taking routine models. Additionally, loose restorative components create space for pellicle adhesion and trigger the start of the inflammatory cascade leading to peri-implant mucositis. There are no randomized clinical trials that directly prove crown design is linked to peri-implant mucositis, however.29,30 Excess cement that remains in place following crown placement not only directly irritates surrounding mucosa, it also contributes to poor plaque control. The rough surface of cement accumulates plaque biofilm and promotes biofilm proliferation.31 In addition to targeted cement removal, restorations — such as screw-retained crowns — can be strategically planned to minimize this risk.
Frank occlusal overloading or excessive off-axis loading may increase the risk for peri-implant disease. Occlusal loading of implants appears concentrated at the bony crestal areas.32,33 There is also evidence to suggest that overloading and poor oral hygiene may be cofactors that contribute to bone loss around implants.34
PREVENTIVE INTERVENTION
Because peri-implantitis can progress faster than typical periodontitis, prevention and early detection and treatment of peri-implant mucositis and peri-implantitis are seminal to optimal outcomes. As the underlying molecular mechanisms of peri-implantitis are not well understood, preventive intervention cannot rely solely on toothpastes and mouthrinses. Disrupting the causative plaque biofilm from the implant surface can reverse the effects of peri-implant mucositis and prevent disease progression.2 Mechanical scaling and root planing has been shown to successfully reverse peri-implant mucositis.35 Although laser therapy has been investigated, its superiority over conventional means has not been established.36
In addition, the use of cotton pellets soaked in chlorhexidine may be useful in removing biofilm without damaging the implant’s titanium surface — although evidence regarding the efficacy of locally delivered and systemic antibiotic therapies as adjuncts to mechanical plaque removal is mixed.37 Pathogenic bacteria have been noted to be resistant to various antibiotics, such as clindamycin, amoxicillin, metronidazole and doxycycline.38 Oral health professionals who note the signs and symptoms of peri-implant disease early and individualize treatment strategies are best prepared to help patients optimize their periodontal health.
References
- Roos-Jansaker AM, Lindahl C, Renvert H, Renvert S. Nine- to fourteen-year follow-up of implant treatment. Part II: presence of peri-implant lesions. J Clin Periodontol. 2006;33:290–295.
- Mombelli A, Lang NP. The diagnosis and treatment of peri-implantitis. Periodontol 2000. 1998;17:63–76.
- Lindhe J, Meyle J; Group D of European Workshop on Periodontology. Peri-implant diseases: Consensus report of the Sixth European Workshop on Periodontology. J Clin Periodontol. 2008;35(8 Suppl):282–285.
- American Academy of Periodontology. Glossary of Periodontal Terms. Available at: perio.org/sites/default/files/files/PDFs/Publications/GlossaryOfPeriodontalTerms2001Edition.pdf. Accessed December 14, 2015.
- Sanz M, Chapple IL. Clinical research on peri-implant diseases: consensus report of working group 4. J Clin Periodontol. 2012;39(Suppl 12):202–206.
- Atieh MA, Alsabeecha NHM, Faggion Jr CM, Duncan WJ. The frequency of peri-implant disease: a systematic review and meta-analysis. J Periodontol. 2013;84:1586–1598.
- Albrektsson T, Dahl E, Enbom L, et al. Osseointegrated oral implants. A Swedish multicenter study of 8139 consecutively inserted Nobelpharma implants. J Periodontol. 1988;5:287–296.
- Faot F, Nasciemento GG, Bielemann AM, Campao TD, Leite FR, Quirynen M. Can peri-implant crevicular fluid assist in the diagnosis of peri-implantitis? A systematic review and meta-analysis. J Periodontol. 2015;86:631–645.
- Hall J, Britse AO, Jemt T, FribergB, A controlled clinical exploratory study on genetic markers for peri-implantitis. Eur J Oral Implantol. 2011;4:371–382.
- Van Dyke TE, van Winkelhoff AJ. Infection and inflammatory mechanisms. J Clin Periodontol. 2013;84:1–7.
- Zitzmann NU, Berglundh T. Definition and prevalence of peri-implant diseases. J Clin Periodontol. 2008;35:286–291.
- Marchetti, C, Farina A, Cornaglia AI. Microscopic, immunocytochemical and ultrastructual properties of peri-implant mucosa in humans. J Periodontol. 2002;73:555–563.
- Lang NP, Berglundh T. Peri-implant diseases: Where are we now? Consensus of the Seventh European Workshop on Periodontology. J Clin Periodontol. 2011:38(Suppl. 11):178–181.
- Schou S, Holmstrup P, Reibel J, Juhl M, Hjorting-Hansen E, Kornman KS. Ligature-induced marginal inflammation around osseointegrated implants and ankylosed teeth: Stereologic and histologic observations in cynomolgus monkeys. J Periodontol. 1993;64:529–537.
- Lindhe J, Berglundh T, Ericsson I, Liljenberg B, Marinello C. Experimental breakdown of peri-implant and periodontal tissues. A study in the beagle dog. Clin Oral Implants Res. 1992;3:9–16.
- Salvi GE, Aglietta M, Eick S, Sculean A, Lang NP, Ramseier CA. Reversibility of experimental peri-implant mucositis compared with experimental gingivitis in humans. Clin Oral Implants Res. 2012;23:182–190.
- Dentino AR, Derderian G, Wolf M, et al. Six-month comparison of powered versus manual toothbrushing for safety and efficacy in the absence of professional instruction in mechanical plaque control. J Periodontol. 2002;73:770–778.
- Rosema NAM, Timmerman MF, Verseteeg PA, Helderman WH, Van der Velden U, Van der Weijden GA. Comparison of the use of different modes of mechanical oral hygiene in prevention of plaque and gingivitis. J Periodontol. 2008;79:1386–1394.
- Ata-Ali J, Ata-Ali F, Galindo-Moreno P. Treatment of peri-implant mucositis: a systematic review of randomized controlled trials. Implant Dent. 2015;24:13–18.
- Gunsolley JC. A meta-analysis of six-month studies of antiplaque and antigingivitis agents. J Am Dent Assoc. 2006;137:1649–1657.
- Mallatt M, Mankodi S, Bauroth K, et al. A controlled 6-month clinical trial to study the effects of a stannous fluoride dentifrice on gingivitis. J Clin Periodontol. 2007;34:762–767.
- Archila L, He T, Winston JL, et al. Antigingivitis efficacy of a stabilized stannous fluoride/sodium hexametaphosphate dentifrice in subjects previously nonresponsive to a triclosan/copolymer dentifrice. Compend Contin Educ Dent. 2005;26(9 Suppl 1):12–18.
- Muguruma T, Iijima M, Brantley WA, et al. Effects of sodium fluoride mouth rinses on the torsional properties of miniscrew implants. Am J Orthod Dentofacial Orthop. 2011;139(5):588–593.
- Botero JE, Gonzalez AM, Mercado RA, et al. Subgingival microbiota in peri-implant mucosa lesions and adjacent teeth in partially edentulous patients. J Periodontol. 2005;76:1490–1495.
- Swierkot K, Lottholz P, Flores-de-Jacoby L, Mengel R. Mucositis, peri-implantitis, implant success, and survival of implants in patients with treated generalized aggressive periodontitis: 3- to 16-year results of a prospective long-term cohort study. J Periodontol. 2012;83:1213–1225.
- Strietzel FP, Reichart PA, Kale A, Kulkarni M, Wegner B, Kuchler I. Smoking interferes with the prognosis of dental implant treatment: A systematic review and meta-analysis. J Clin Periodontol. 2007;34:523–544.
- Clementini M, Rossetti PH, Penarrocha D, Micarelli C, Bonachela WC, Canullo L. Systemic risk factors for peri-implant bone loss: a systematic review and meta-analysis. Int J Oral Maxillofac Surg. 2014;43:323–334.
- Salvi GE, Carollo-Bittel B, Lang NP. Effects of diabetes mellitus on periodontal and peri-implant conditions: Update on associations and risks. J Clin Periodontol. 2008;35:398–409.
- Belser UC, Bernard JP, Buser D. Implant-supported restorations in the anterior region: prosthetic considerations. Pract Periodontics Aesthet Dent. 1996;8:875–883.
- Brägger U, Hirt-Steiner S, Schnell N, et al. Complication and failure rates of fixed dental prostheses in patients treated for periodontal disease. Clin Oral Implants Res. 2011;22:70–77.
- Wilson TG Jr. The positive relationship between excess cement and peri-implant disease: A prospective clinical endoscopic study. J Periodontol. 2009;80:1388–1392.
- Rungsiyakull C, Rungsiyakull P, Li Q, Li W, Swain M. Effects of occlusal inclination and loading on mandibular bone remodeling: A finite element study. Int J Oral Maxillofac Implants. 2011;26:527–537.
- Stanford CM, Brand RA. Toward an understanding of implant occlusion and strain adaptive bone modeling and remodeling. J Prosthet Dent. 1999;81:553–561.
- Fu JH, Hsu YT, Wang HL. Identifying occlusal overload and how to deal with it to avoid marginal bone loss around implants. Eur J Oral Implantol. 2012;5(Suppl):S91–103.
- Renvert S, Roos-Jansaker AM, Claffey N. Non-surgical treatment of peri-implant mucositis and peri-implantitis: a literature review. J Clin Periodontol. 2008;35(8Suppl):305–315.
- Kotsakis GA, Konstantinidis I, Karoussis IK, Ma X, Chu H. A systematic review and meta-analysis of the effect of various laser wavelengths in the treatment of peri-implantitis. J Periodontol. 2014;85:1203–1213.
- Esposito M, Grusovin MG, Worthington HV. Treatment of peri-implantitis: what interventions are effective? A Cochrane systematic review. Eur J Oral Implantol. 2012;5 (Suppl):S21–41.
- Rams TE, Degener JE, van Winkelhoff AJ. Antibiotic resistance in human peri-implantitis microbiota. Clin Oral Implants Res. 2014;25:82–90.
