
PRF Offers Simple, Autologous Regenerative Power
Platelet-rich fibrin (PRF) enhances wound healing and tissue regeneration using a patient’s own blood. Unlike earlier platelet concentrates, PRF is easy to prepare, requires no additives, and offers a sustained release of growth factors for improved outcomes in dental procedures.
In recent years, regenerative medicine has made a remarkable impact, showing its potential across different fields, including dentistry. Platelet-rich fibrin (PRF), a platelet concentrate derived from the patient’s own blood, has gained significant attention for its wound healing and tissue regeneration properties. This article explores the benefits, applications, and evolving role of PRF in modern dentistry.
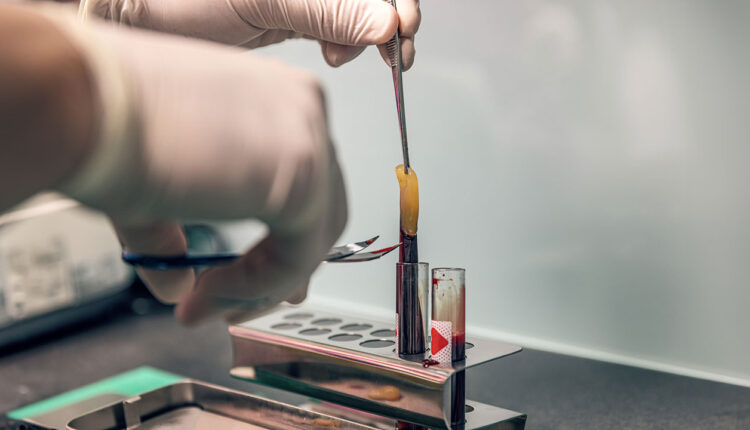
PRF is an autologous concentration of platelets in a fibrin matrix.1 The process entails a simplified method in which a patient’s blood is centrifuged at specific speeds, leading to the formation of PRF clot which is rich in natural platelets, growth factors, and leukocytes. Unlike platelet-rich plasma (PRP), PRF does not require biochemical handling and is therefore simple to prepare and apply.
The initial concept behind creating platelet concentrates was to collect concentrated platelets and natural growth factors in plasma solutions, which could then be applied to surgical sites to enhance local healing.2 This technique, introduced in the late 1990s, became known as PRP.3 PRP consists mostly of platelets that release growth factors to actively start the wound healing process and enhance cell adhesion, proliferation, and migration.4 Around the same time, another platelet concentrate was introduced that used anticoagulants called platelet-rich growth factor (PRGF).5
However, there are several limitations to using PRP and PRGF. Their preparation requires additional coagulation factors such as bovine thrombin or CaCl2. The process also involves two separate centrifugation stages to concentrate platelets without including leukocytes, which sometimes can take up to an hour. The resulting liquid nature of PRP complicates handling, limiting its applications, as it needs to be used with other biomaterials to improve handling. Additionally, PRP has a very short growth factor release profile, hindering its potential for bone regeneration.6 These challenges have led to the creation of a second-generation platelet concentrate, PRF, which is made entirely from autologous sources.7
References
- Coury AJ. Expediting the transition from replacement medicine to tissue engineering. Regen Biomater. 2016;3:111-113.
- Anfossi G, Trovati M, Mularoni E, Massucco P, Calcamuggi G, Emanuelli G. Influence of propranolol on platelet aggregation and thromboxane B2 production from plateletrich plasma and whole blood. Prostaglandins Leukot Essent Fatty Acids. 1989;36:1-7.
- Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, Georgeff KR. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;85:638-646.
- Marx RE. Platelet-rich plasma: evidence to support its use. J Oral Maxillofac Surg. 2004;62:489-496.
- Anitua E, Prado R, Troya M, et al. Implementation of a more physiological plasma rich in growth factor (PRGF) protocol: Anticoagulant removal and reduction in activator concentration. Platelets. 2016;27:459-466.
- Kobayashi E, Flückiger L, Fujioka-Kobayashi M, et al. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin Oral Investig. 2016;20:2353-2360.
- Saluja H, Dehane V, Mahindra U. Platelet-rich fibrin: A second generation platelet concentrate and a new friend of oral and maxillofacial surgeons. Ann Maxillofac Surg. 2011;1:53-57.
This originally appeared in Luan KW, Narvekar A. Unlocking the regenerative power of platelet-rich fibrin. Decisions in Dentistry. 2025;11(2):40-45.
