

Restoring Function and Aesthetics: A Full-Mouth Rehabilitation Success Story
This case study showcases the comprehensive crown lengthening treatment of a 52-year-old patient requiring full-mouth rehabilitation due to severe dental erosion and wear. Through interdisciplinary collaboration and precise surgical techniques, the patient’s dentition was restored, significantly improving both functional and aesthetic outcomes.
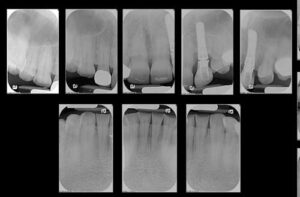
The following case illustrates crown lengthening treatment of the maxillary and mandibular dentition (Figure 1 through Figure 12). A 52-year-old man presented to the graduate prosthodontics clinic at the University of Texas Health Science Center at San Antonio School of Dentistry interested in an implant- and tooth-supported full-mouth rehabilitation. He had a medical history significant for hypertension, type 2 diabetes mellitus, hypercholesterolemia, and anxiety. He presented with severe erosion of the palatal surfaces of the maxillary dentition, localized severe attrition, and localized moderate abrasion. The patient was classified as a Turner Category 3 (ie, excessive wear without loss of occlusal vertical dimension, with limited restorative space). He had excessive gingival display at full animation secondary to a hyperactive upper lip.



After a thorough examination, a comprehensive treatment plan was developed, and the patient was referred to the graduate periodontics clinic. Surgical procedures were performed using IV conscious sedation. The treatment plan included:
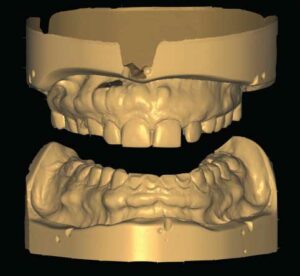
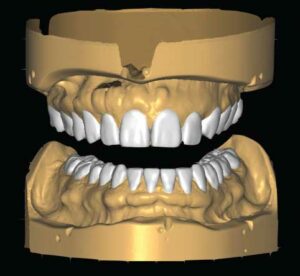
- Virtual wax-up of the definitive contours of the maxillary and mandibular teeth
- Maxillary and mandibular functional crown lengthening, with extractions of retained primary tooth #J and 19, and site development for future implant placement
- Delayed implant placement at sites #13 and 19
- Implant- and tooth-supported prostheses for the maxillary and mandibular dentition
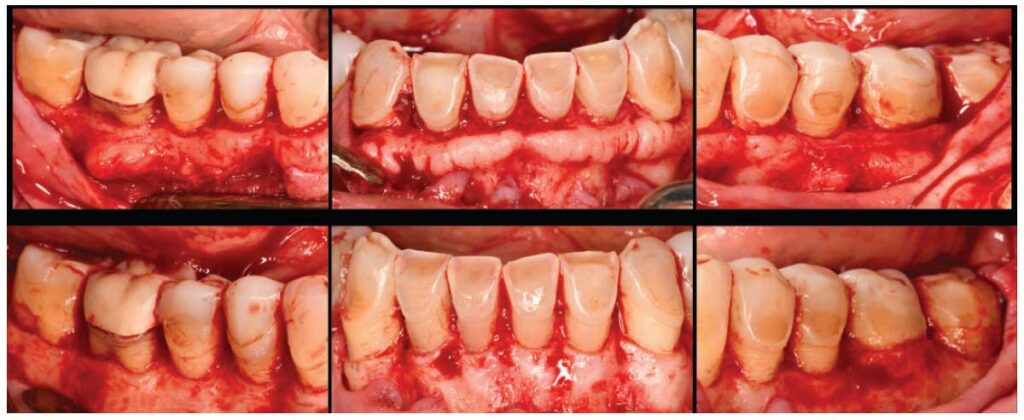
Surgical therapy was performed to establish the coronal tooth structure required to restore worn dentition with full-coverage restorations. A surgical guide delineating the desired final position of the gingival margins was provided by the restorative dentist and used intraoperatively. Functional crown lengthening was performed in all four quadrants to achieve proper tooth dimensions for the provisional and definitive prostheses. Teeth #J and 19 were extracted, and ridge preservation was performed to prepare for future implant placement.

Post-operative instructions were reviewed. The patient returned for follow-up at two weeks, one month, and two months. The final marginal position allows for improved hygiene and restorative access. If functional crown lengthening was not successfully performed, crown preparations would lack proper retention and resistance forms and extend apically to bone, damaging the gingival complex. Future implants would have also been placed too shallow, given the tight interdental space at initial presentation. The patient will continue restorative care and yearly recalls at the graduate prosthodontics clinic.

Clinically, treatment planning predicated on a basic understanding of the biologic influences on the periodontal/restorative interface can provide lasting results. Identifying the correct, underlying etiology for the patient’s initial presentation will dictate surgical and restorative treatment. As part of this effort, the relationship of the hard and soft tissues must be respected to prevent the dentogingival complex from breaking over time.



When managed successfully, esthetic and functional crown lengthening procedures can transform the smile and facial profile. As demonstrated by the clinical report presented here, an interdisciplinary team can outline proper workflows and navigate challenges in cases requiring surgical crown lengthening.
