

Caring for Patients With Autism Spectrum Disorders
Pretreatment planning, proper assessment and effective communication will ensure optimal treatment for this patient population.
Pretreatment planning, proper assessment and effective communication will ensure optimal treatment for this patient population
PURCHASE COURSE
This course was published in the February 2018 issue and expires February 2021. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the February 2018 issue and expires February 2021. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
- Describe autism spectrum disorder (ASD), its prevalence, and barriers to care for this population.
- Explain common patient characteristics, and clinical strategies for ensuring effective treatment for patients with ASD.
- Discuss the importance of treatment planning and effective communication when caring for these patients.
Autism spectrum disorder (ASD) is a complex, lifelong developmental disability that impairs communication, as well as social, behavioral and intellectual functioning.1 As a catchall term, ASD includes autistic disorder, pervasive developmental disorder not otherwise specified, and Asperger syndrome, all of which differ in the number and severity of diagnostic features.2 Data from the U.S. Centers for Disease Control and Prevention (CDC) indicate the prevalence of ASD is approximately one in 68 children (and the rate is 4.5 times higher in boys); in addition, the condition is reported in all racial, ethnic and socioeconomic populations.2 Behaviors can range from aggression and being inattentive or hyperactive, to having a short attention span and/or having difficulty listening. It can also manifest as anxiety, extreme mood swings, being oppositional defiant and/or obsessive-compulsive.3,4 Communication deficits, sensory perception/overstimulation, obsessive routines, repetitive behaviors, unpredictable body movements, and self-injurious behavior can cause some ASD patients to exhibit poor oral hygiene.1 In order to provide effective care, oral health professionals should be knowledgeable about management strategies for patients with ASD.
While patients with ASD vary widely in symptoms and severity, up to 41% have an intellectual disability (IQ < 70), in addition to other coexisting conditions, such as epilepsy.1,2 According to the CDC, the scientific community (1) cannot explain the exact etiology of ASD; (2) agrees the disorder has no known cause; and (3) believes there can be multiple underlying factors.1,2,4 Currently, no medical or genetic test exists for ASD; therefore, diagnosis is based solely upon clinical testing.1,3 This disorder presents in ways ranging from individuals being mentally gifted to intellectually challenged, and the range includes varying levels of impaired social interaction, communication, and restricted or repetitive behaviors.5 Patients who are diagnosed with ASD may create problems for the dental team due to limited oral access, communication barriers, dental anxiety and tantrums.5
Considerations for oral health care include harmful oral habits, such as bruxism, nonnutritive chewing, tongue thrusting, and self-injurious behaviors of picking at the gingiva and lip biting.3 In addition to these considerations, tooth erosion, caries, poor oral hygiene, and limited dietary preferences are characteristic of these patients.4 The dental team should recognize the ways in which ASD patients’ perceptions of the clinical environment may differ from others; the goal is to develop sensory integration to meet ASD patients’ oral health care needs. In addition, oral signs and symptoms exhibited by ASD patients should be recognized and addressed appropriately.5 This article will focus on characteristic differences in ASD patients, as well as clinical considerations that will help improve treatment outcomes.
BACKGROUND
Studies indicate that limited access to dental care and barriers preventing dental treatment are widespread for this patient population.4–8 A survey of caregivers found a failure of patients with ASD to find a dental home with providers who have the knowledge and skill to provide optimal care.4 Patients with ASD can be challenging to work with due to limited communication, higher-than-normal anxiety, lack of making eye contact, and repetitive behaviors.5–7 At particular risk for periodontal disease and high caries rates are ASD patients who are described as extremely uncooperative.4 Individuals with a track record of difficult behavioral patterns are reported to be more likely to lack a dental home, and have longer periods between visits.5 Barriers to care for this population directly increase the number of special needs patients with unmet dental needs.4–7 To improve treatment success, providers should seek to minimize patient apprehension and mistrust by making the environment more inviting and suitable for patients with ASD.4–7
In addition to addressing communication deficits, clinicians must recognize that patients with ASD are likely to have one or more other psychiatric disorders, such as childhood anxiety disorders, depressive disorders, oppositional defiant and conduct disorders, attention-deficit/hyperactivity disorder (ADHD), tic disorders, trichotillomania, enuresis and encopresis.9 In one study, researchers found that more than two thirds of the ASD participants had at least one comorbid disorder, and almost half had two or more. Specifically, 29% were diagnosed with social anxiety, 28% with ADHD, and 28% with oppositional defiant disorder.9 Research indicates high rates of ADHD, and that psychiatric disorders are frequently prevalent and multiple in patients with ASD.3,8–10
This patient population is likely to exhibit behaviors similar to those with ADHD because many individuals with autism are also diagnosed with ADHD.9,11,12 Anxiety in patients with ASD was also found to correlate with reduced salivary flow, as noted by research that demonstrates a relationship between the amount of salivary secretions and overall oral health.13–16 Subjects with ASD had less salivary secretions compared to control groups, and reported more anxiety and stress with dental care.13–16 Regardless of the type and frequency of medications taken, salivary flow was less for subjects with ASD, which, in turn, increases the likelihood of oral disease.13–16
CLINICAL IMPLICATIONS
Sensory-related features of oral care are of prime importance when treating patients with ASD.17 Often, these patients do not like having the tongue touched or the teeth brushed; they may also dislike the taste and texture of all brands of dentifrice, and prove uncooperative during treatment.17 In addition, this population may dislike bright lights, loud sounds, smells, touching the inside of the mouth, or leaning back in the dental chair.13,17,18 Providers should implement strategies to mitigate sensory difficulties, such as reducing unnecessary sights, sounds, odors or other stimuli. Additional anxiety-reducing methods include booking early day appointments when patients are most rested, and blocking the schedule to minimize surrounding stimuli. Another technique is to desensitize the oral cavity through intense pressure therapy in areas away from the mouth.17,19 Finally, providing written instructions for care and appointment reminders will reduce issues with overbrushing and missed appointments.13
When treating patients with ASD, the planning phase should involve interprofessional collaboration as part of a team approach to care.4,8,20 Collaboration advances oral care; an example would be partnering with a registered dietitian and/or physician to manage dietary selections that support oral health.8,20 This may help limit sugary and acidic diets that exacerbate oral disease.17 Occupational therapists are helpful partners in mitigating sensory sensitivities in relation to oral health;17 similar collaborations can also prove beneficial when finding ways to work through patients’ damaging oral habits.3,8
In addition, collaboration with family members and caregivers is necessary to authorize protective stabilization techniques.8,20 For patients who have issues with cooperation, tongue thrusting or nonnutritive chewing, stabilization of the patient’s head, lips and tongue is needed to maintain procedural safety. This can be achieved with rolled towels, pillows and bite blocks.8 Another strategy to comfort this patient population is to leave the lead X-ray apron draped over the patient for the duration of the appointment.21 In order to provide safe care, communicating each step of the procedure to the patient and/or parent/caregiver minimizes anxiety and aids in patient compliance.
ORAL HEALTH PROFESSIONALS’ ROLE
Oral care providers can more effectively communicate treatment and provide a dental environment tailored for patients with ASD by drawing from special techniques, such as desensitizing, developing a sensory adapted environment, utilizing a picture exchange communication system (PECS), and knowing when to refer for advanced behavior guidance techniques.4,8,22,23 This patient group can undergo desensitizing via a minimal threshold examination in which the exam is done with an intraoral mirror while the patient is seated in the dental chair.19,24 Results might take a few sessions,24 but the goal is to create a favorable dental experience starting with the first appointment.18
This initial appointment provides the opportunity to adapt the environment to meet the patient’s sensory needs.4,18 The use of a pretreatment questionnaire completed by the patient, parent or caregiver will shed light on the patient’s abilities and needs.18 A second form to document communication mechanisms, and note what works — as well as triggers, rewards and visit accomplishments — will prove useful.18 These forms will be instrumental in improving dental care and patient cooperation during future appointments.
Clinicians should be prepared for patients whose ability to communicate varies significantly. Individuals exhibiting a measureable level of communication ability can benefit from the show-tell-do approach, voice control, and positive reinforcement behavior management techniques.8,25 In a pilot study for dental preventive procedures, PECS was developed as a nonverbal approach for communicating with patients who have ASD and related developmental disabilities.17,23 This approach is particularly suited for patients who are unable to speak intelligibly or at all, who lack spontaneous or functional speech, or who lack a sufficient method of alternate communication.17,23 Nonverbal patients with more severe levels of autism will likely not respond to conventional behavior management (especially if they are combative), and may require restraints, sedation and/or general anesthesia.25
MEDICATION CONSIDERATIONS
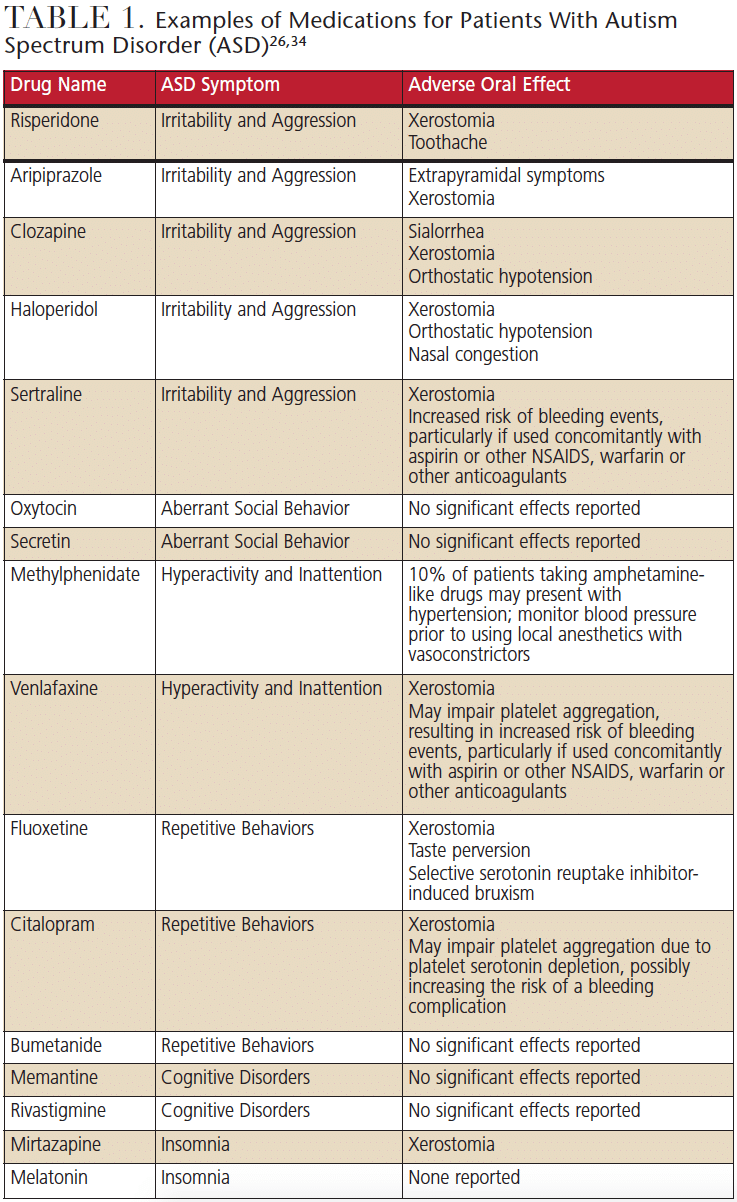
As noted, individuals with ASD often are treated with some type of behavioral therapy; however, some will require pharmacological treatment to function during daily activities. Studies of the use of risperidone, a second-generation antipsychotic, on children with ASD ages 5 to 17 showed a reduction in tantrums, aggressive behaviors and self-injurious behaviors.26–29 Reduced levels of irritability, social withdrawal, hyperactivity and inappropriate speech were also noted. Studies of the psychotropic drug aripiprazole, approved for the treatment of irritability in children ages 6 to 17 with ASD, demonstrated improvement in irritability; however, significant adverse events were found.30–32
In addition to these drugs, individuals with ASD may be prescribed other medications to manage comorbid conditions. In a study of 2853 children ages 2 to 17 enrolled in an autism registry, Coury et al10 noted that multiple medications were used to treat psychiatric or comorbid conditions, including depression, bipolar disorder, ADHD, obsessive-compulsive disorder, anxiety, gastrointestinal problems and sleep disorders. While most subjects were taking more than one medication, others were taking three or more medications. Examples of the drugs patients with ASD may be prescribed appear in Table 1. It is important for clinicians to note the general side effects — and any oral effects — of these drugs, and educate patients and parents/caregivers about managing the oral effects of medications. Although these represent a treatment alternative, many are off-label options, with limited results in terms of efficacy and the potential for adverse events. Continued long-term study and new drug development for the treatment of ASD symptoms are needed.33
CONCLUSION
Dental visits can be extremely stressful for patients with ASD, often leading to incomplete treatment due to anxiety and lack of cooperation. Caring for patients with ASD requires pretreatment planning and proper assessment, including scheduling appointments for the appropriate time, and developing effective patient and parent/caregiver communication. The entire dental staff should be knowledgeable about caring for patients with ASD so the initial impression of clinical care is inviting.
Knowledge and understanding of sensory processing and the sensory aspects of the dental visit may improve patient cooperation, leading to better results. Oral health professionals must work with parents/caregivers to determine which events are stressful for patients with ASD, and develop strategies that are individually tailored. The role of continuing education is essential in overcoming the challenges encountered when treating this patient population.
REFERENCES
- National Institute of Health. Autism Spectrum Disorders (ASD). Available at: https://www.nichd.nih.gov/health/topics/autism/Pages/default.aspx. Accessed January 11, 2018.
- Centers for Disease Control and Prevention. Autism Spectrum Disorder (ASD) Data and Statistics. Available at: https://www.cdc.gov/ncbddd/autism/data.html. Accessed January 11, 2018.
- University of Washington School of Dentistry. Patients with Special Needs Fact Sheets. Available at: dental.washington.edu/dept-oralmed/special-needs/patients-with-specialneeds/. Accessed January 11, 2018.
- Delli K, Reichart PA, Bornstein MM, Livas C. Management of children with autism spectrum disorder in the dental setting: concerns, behavioural approaches and recommendations. Med Oral Patol Oral Cir Bucal. 2013;18:862–868.
- Brickhouse TH, Farrington FH, Best AM, Ellsworth CW. Barriers to dental care for children in Virginia with autism spectrum disorders. J Dent Child (Chic). 2009;76:188–193.
- Chi DL, Momany ET, Mancl LA, et al. Dental homes for children with autism: a longitudinal analysis of Iowa Medicaid’s ISmile Program. Am J Prev Med. 2016;50:609–615.
- Nelson LP, Getzin A, Graham D, et al. Unmet dental needs and barriers to care for children with significant special health care needs. J Pediatr Dent. 2011;33:29–36.
- Moore TA. Dental care for patients with special needs. Decisions in Dentistry. 2016;2(9):50–53.
- Simonoff E, Pickles A, Charman T, Chandler S, Loucas T, Baird G. Psychiatric disorders in children with autism spectrum disorders: prevalence, comorbidity, and associated factors in a population-derived sample. J Am Acad Child Adolesc Psychiatry. 2008;47:921–929.
- Coury DL, Anagnostou E, Manning-Courtney P, et al. Use of psychotropic medication in children and adolescents with autism spectrum disorders. Pediatrics. 2012;130(S69-S76).
- Charles JM. Dental care in children with developmental disabilities: attention deficit disorder, intellectual disabilities, and autism. J Dent Child (Chic). 2010;77:84-91.
- Waldman HB, Meinzer MC, Perlman SP, Wong A. Caring for patients with attentiondeficit/hyperactivity disorder. Decisions in Dentistry. 2017;3(5):52–55.
- Blomqvist M, Bejerot S, Dahllöf G. A cross-sectional study on oral health and dental care in intellectually able adults with autism spectrum disorder. BMC Oral Health. 2015;15:1–8.
- Hidas A, Noy AF, Birman N, et al. Oral health status, salivary flow rate and salivary quality in children, adolescents and young adults with ADHD. Arch Oral Biol. 2011:56:1137–1141.
- Rai K, Hegde AM, Jose N. Salivary antioxidants and oral health in children with autism. Arch Oral Biol. 2012;57:1116–1120.
- Stein LI, Polido JC, Mailloux Z, Coleman GG, Cermak SA. Oral care and sensory sensitivities in children with autism spectrum disorders. Spec Care Dentist. 2011;31:102–110.
- Stein LI, Polido JC, Cermak SA. Oral care and sensory concerns in autism. Am J Occup Ther. 2012;66:e73–e76.
- Nelson TM, Sheller B, Friedman CS, Berneir R. Educational and therapeutic behavioral approaches to providing dental care for patients with autism spectrum disorder. Spec Care Dentist. 2015;35:105–113.
- Nelson T, Chim A, Sheller BL, McKinney CM, Scott JM. Predicting successful dental examinations for children with autism spectrum disorder in the context of a dental desensitization program. J Am Dent Assoc. 2017;148:485–492.
- Schaffer R, Perry M, Dollin SS. Oral health care and autism: creating and implementing training and treatment guidelines – an interprofessional collaboration among dentists, parents and autism professionals. J Interprof Educ Pract. 2015;1:70.
- Cermak SA, Stein Duker LI, Williams ME, Dawson ME, Lane CJ, Polido JC. Sensory adapted dental environments to enhance oral care for children with autism spectrum disorders: a randomized controlled pilot study. J Autism Dev Disord. 2015;45:2876–2888.
- Loo CY, Graham RM, Hughes CV. Behaviour guidance in dental treatment of patients with autism spectrum disorder. Int J Paediatr Dent. 2009;19:390–398.
- Zink AG, Diniz MB, Rodrigues dos Santos MT, Guaré RO. Use of a picture exchange communication system for preventive procedures in individuals with autism spectrum disorder: pilot study. Spec Care Dentist. 2016;36:254–259.
- Kuhaneck HM, Chisholm, EC. Improving dental visits for individuals with autism spectrum disorders through an understanding of sensory processing. Spec Care Dentist. 2012;32:229–233.
- Hernandez P, Ikkanda Z. Applied behavior analysis: behavior management of children with autism spectrum disorders in dental environments. J Am Dent Assoc. 2011;142:281–287.
- LeClerc S, Easley D. Pharmacological therapies for autism spectrum disorder: a review. P T. 2015;40:389–397.
- McCracken JT, McGough J, Shah B, et al. Risperidone in children with autism and serious behavioral problems. N Engl J Med. 2002;347:314–321.
- Troost PW, Lahuis BE, Steenhuis MP, et al. Long-term effects of risperidone in children with autism spectrum disorders: a placebo discontinuation study. J Am Acad Child Adolesc Psychiatry. 2005;44:1137–1144.
- Sharma A, Shaw S. Efficacy of risperidone in managing maladaptive behaviors for children with autism spectrum disorder: a meta-analysis. J Pediatr Healthcare. 2012;264:291–299.
- Marcus RN, Owen R, Manos G, et al. Safety and tolerability of aripiprazole for irritability in pediatric patients with autistic disorder: a 52-week, open-label, multicenter study. J Clin Psychiatry. 2011:72:1270–1276.
- Varni JW, Handen BL, Corey-Lisle PK, et al. Effect of aripiprazole 2 to 15 mg/d on health-related quality of life in the treatment of irritability associated with autistic disorder in children: a post hoc analysis of two controlled trials. Clin Ther. 2012;34:980–992.
- Ching H, Pringsheim T. Aripiprazole for autism spectrum disorders (ASD). Cochrane Database Syst Rev. 2012;5:CD009043.
- Wink LK, Plawecki MH, Erickson CA, Stigler KA, McDougle CJ. Emerging drugs for the treatment of symptoms associated with autism spectrum disorders. Expert Opin Emerg Drugs. 2010;15:481–494.
- Wynn RL, Meiller TF, Crossley HL. Drug Information Handbook for Dentistry. 23rd ed. Hudson, Ohio: Lexi-Comp Inc; 2017.
The authors have no commercial conflicts of interest to disclose.
FEATURED IMAGE BY KATARZYNABIALASIEWICZ/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. February 2018;4(2):47-50.

