

10 Orthodontic Challenges in the Primary and Mixed Dentition
Early identification of occlusal issues in children facilitates timely orthodontic treatment that helps support optimal oral health in the primary and mixed dentition.
Early identification of occlusal issues in children facilitates timely orthodontic treatment that helps support optimal oral health in the primary and mixed dentition
PURCHASE COURSE
This course was published in the September 2018 issue and expires September 2021. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
Malocclusion is relatively common in the United States, and there is wide variability in its severity.1 The evaluation of skeletal and occlusal relationships is an important component of all comprehensive and recall dental examinations. Although orthodontists play a vital role in managing these cases, all dentists and specialists should screen for orthodontic problems, beginning with the primary dentition. Early identification of occlusal issues warrants timely referral to an orthodontist for evaluation, diagnosis and long-term treatment planning. This article will provide an overview of common orthodontic concerns in the primary and mixed dentition, and describe interventions to address these challenges.
This course was published in the September 2018 issue and expires September 2021. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
Educational Objectives
After reading this course, the participant should be able to:
- List common orthodontic challenges and treatment approaches in the primary and mixed dentition.
- Describe the importance of screening for orthodontic problems and common clinical terms used during these examinations.
- Explain common causes of malocclusion in the pediatric population.
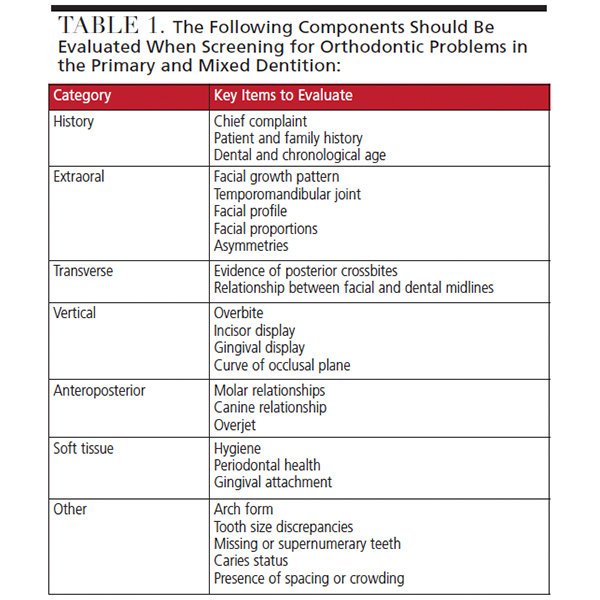
Table 1 lists key items to evaluate when screening for orthodontic issues in the primary and mixed dentition. The clinical exam should be supplemented by appropriate intraoral and extraoral radiographs. A panoramic radiograph is generally recommended in the early mixed dentition around the time the permanent incisors begin to erupt.2 When there is concern for skeletal discrepancies, additional imaging (such as lateral cephalometrics and cone beam computed tomography) can be used to establish a diagnosis.
Orthodontic treatment planning relies upon proper diagnosis, development of a problem list and treatment objectives, and a sequenced treatment plan. Some interventions can be treated in a single phase of care, while others should be treated with multiple phases — such as early (phase I) and later (phase II) treatment regimens. The following 10 orthodontic challenges in the primary and mixed dentition represent treatment options ranging from simple interventions that can be addressed by a general practitioner to complex challenges that should be managed by providers with advanced training in orthodontics and dentofacial orthopedics.
1 Mild to Moderate Crowding: The most common malocclusion among U.S. patients is a Class I malocclusion with crowding.1 This can be limited to one or both arches, and classified as mild, moderate or severe. As children transition from primary to the mixed dentition, it is normal to see spacing in the maxillary anterior region and crowding in the mandible.3 Both are considered normal and do not necessarily require early intervention.
The size difference between primary incisors widths and permanent incisor widths is called incisor liability. Mechanisms to accommodate incisor liability include the presence of spacing in primary teeth, primate space, leeway space, and the flaring of incisors as they reach their final position.4 To determine if crowding can be categorized as mild/moderate or more severe, clinicians can perform an arch analysis to identify possible arch length discrepancies and estimate the space that will be needed for unerupted teeth.5 When crowding surpasses the arch length space available, the provider can consider preserving the leeway space with fixed bilateral space maintainers.6
Generally, mild to moderate crowding does not require phase I treatment. Understanding space maintenance principles can facilitate preservation of leeway space to simplify comprehensive care.
 2 Severe Crowding: In cases of severe crowding, there are two general approaches to treatment: extraction or nonextraction. General guidelines for serial extraction are: 5 mm or more of crowding in each quadrant, Class I molar relationship in the absence of other skeletal issues, and adequate soft tissue support.7 Serial extraction involves the sequential removal of the primary canines, primary first molars, and the first premolars. Due to the irreversible nature of extraction, any decision to use this approach should be coordinated with an orthodontist who will provide long-term care,8 as patients treated with serial extractions will often require orthodontic care to level, align and consolidate spaces following extractions.
2 Severe Crowding: In cases of severe crowding, there are two general approaches to treatment: extraction or nonextraction. General guidelines for serial extraction are: 5 mm or more of crowding in each quadrant, Class I molar relationship in the absence of other skeletal issues, and adequate soft tissue support.7 Serial extraction involves the sequential removal of the primary canines, primary first molars, and the first premolars. Due to the irreversible nature of extraction, any decision to use this approach should be coordinated with an orthodontist who will provide long-term care,8 as patients treated with serial extractions will often require orthodontic care to level, align and consolidate spaces following extractions.
3 Anterior Dental Crossbite: The presence of one or two incisors in crossbite is usually a dental crossbite, rather than a skeletal crossbite. An accurate diagnosis of skeletal versus dental crossbite is imperative.9 If left untreated, an anterior dental crossbite can lead to traumatic wear on teeth, traumatic occlusion leading to mobility, loss of bone support and gingival dehiscence.
Treatment approaches for a single tooth can include a fixed or removable appliance with a finger spring, limited brackets, or a bonded appliance (e.g., Catlan appliance or composite), each of which serve as a ramp to “jump” the crossbite.10 Although numerous sources cite the use of tongue blade, there are no specific guidelines about the frequency, duration or force needed to correct an anterior crossbite.
Crossbite of one or both permanent lateral incisors is generally indicative of crowding and insufficient arch perimeter. Because lateral incisors erupt lingually/palatally, they may be “crowded out” following the eruption of central incisors. To gain adequate space for lateral incisors to erupt, expansion and fixed appliances may be necessary.
4 Anterior Skeletal Crossbite/Class III: An anterior crossbite involving all incisors can be attributed to an anterior functional shift or a true skeletal crossbite. To differentiate between the two, the dentist should evaluate the occlusal relationship when the patient closes in centric relation.9 If there is a premature point of contact accompanied by an anterior shift, the crossbite may be corrected with limited orthodontics.
If the patient bites into a crossbite position when closing in centric relation, the crossbite is likely due to a true Class III relationship. This can be attributed to maxillary deficiency, mandibular prognathism, or a combination of both. A proper diagnosis of the underlying cause must be determined, as this dictates the course of treatment. Maxillary retrusion is treated with protraction headgear.11 There is limited evidence to suggest that chin-cup therapy is effective in reducing mandibular growth.12 When the Class III growth pattern is severe, patients require surgical intervention to achieve an ideal orthodontic and skeletal relationship after growth is complete at the end of adolescence.
5 Ectopic Eruption of Molars: Ectopic eruption of molars occurs in up to 3% of the population, and is seen more frequently in the maxilla.13 More than two-thirds of ectopic molars self-correct. Dentists should routinely examine bitewing radiographs to evaluate the path of eruption on permanent molars. If ectopic eruption tendency is noted, the molars should be monitored radiographically for six to 12 months. If there is no improvement, intervention is needed.
In mild cases, an elastic separator or brass wire can deimpact the permanent molar and should be checked weekly until correction is noted.14 If the first permanent molar has resorbed the distal aspect of the second primary molar, an orthodontic appliance should be used to distalize and correct the impaction of the permanent molar. An asymptomatic second primary molar (with sufficient stability) is necessary to anchor these appliances. When resorption of the second primary molar is severe or the tooth is mobile/symptomatic, extraction of the primary second molar is the only option. Space will need to be regained and maintained to allow eruption of the second premolar.
6 Premature Loss of Molars and Space Loss: One common reason for early loss of a primary molar is extensive caries treated by extraction. The early loss of a primary molar can lead to space loss and reduced arch length.15 Space loss is more severe following the premature loss of a second primary molar compared to a first primary molar.16 Total space loss is greater when the primary tooth loss occurs before or during the eruption of the first permanent molar.17 The eruption path and force of the first permanent molars cause the teeth to erupt with a mesial inclination, with a slight rotation around the palatal root in the maxilla. In most cases, space maintainers are recommended to reduce the severity of space loss.
It is beyond the scope of this article to provide space maintainer recommendations for each clinical scenario, but attention must be paid as to whether the premature loss occurred in the maxilla or mandible, involved a first or second primary molar, which permanent teeth have erupted, and whether the patient requires preservation of arch length.
If space is not maintained, the patient may develop a pseudo Class II or pseudo Class III molar relationship due to space loss. Space-regaining methods in the maxilla include headgear, limited brackets with open coil mechanics, a pendulum appliance, or removable appliance with a distalizing spring. Many of these same mechanics — including the lip bumper or lower lingual holding arch with distalizing loops — can be used to regain space in the mandible.18
7 Selective Extractions for Eruption Guidance: Primary teeth can be extracted to promote or correct the path of eruption of permanent teeth. When permanent maxillary canines erupt with a mesioangular path or the permanent canine overlaps the midline of the lateral incisor, selective extraction of primary canines can promote permanent canine correction.19 In cases with crowding, when a primary canine is lost unilaterally due to eruption of a permanent incisor, the contralateral canine should be extracted and space maintenance should be considered to preserve the midline and arch perimeter.
Other clinical situations in which extraction of primary teeth can promote/guide the eruption of permanent teeth is in the premolar region. If premolars are found to have an angular eruption path or are located ectopically to the buccal or lingual, early extraction of primary molars with space maintenance (if necessary) can promote a more favorable premolar eruption.
8 Class II Malocclusion: A Class II molar relationship can occur from either a dental or skeletal etiology. Skeletal Class II malocclusion can be attributed to a prognathic maxilla, retrognathic mandible, or a combination of both.20 A Class II Division I occlusion is characterized by increased overjet with flared incisors, while a Class II Division II occlusion is characterized by flared lateral incisors and/or retroclined central incisors, with increased overbite. A Class II dental relationship with a skeletal Class I relationship is treated with orthodontic therapy and may include selective extractions, while a skeletal Class II can be treated with orthopedic intervention.
Maxillary prognathism is treated with headgear, while mandibular retrusion can be treated with functional appliance to promote forward posturing of the mandible.21 Treatment using functional appliance should coincide with the early part of the growth curve. In cases in which the skeletal pattern is severe, surgical correction with mandibular advancement or a maxillary setback may be necessary following the growth period.
9 Posterior Crossbite: A posterior crossbite is defined as the abnormal transverse relationship between one or more teeth in a quadrant. This can be limited to a single tooth, or it can involve a full segment unilateral or bilateral crossbite either in the permanent, primary or mixed dentition.
Single-tooth posterior crossbites in the primary dentition do not always require orthodontic intervention because they may not persist in the permanent dentition. Single-tooth crossbites in permanent molars can be fixed with cross-elastics. Unilateral crossbites in the primary dentition are of greater concern when they involve the entire molar segment and are accompanied by a functional shift, leading to a deflection to one side and a midline deviation on closing.22 A posterior crossbite with a lateral shift can lead to asymmetric growth of the mandible.23 The most common cause of a lateral functional shift is a premature contact on the primary canine.9 In some cases, this premature contact can be equilibrated to remove the crossbite, while other cases require future correction with orthopedic expansion.
When a patient has a posterior segment crossbite in the primary dentition that is not accompanied by deflection, early treatment may not be necessary if the permanent molar erupts in the correct transverse relationship. In some cases, expansion can be initiated in the primary dentition. Once erupted, the permanent molar relationship should be examined. If the crossbite persists in the permanent molar, expansion will be necessary to achieve ideal occlusion and increase arch perimeter. Expansion when children are younger, before suture closure, is more efficient and stable in terms of treatment outcomes.
Passive expansion can be achieved via slow expansion with a W-arch or quad helix.24 While passive/slow expansion appliances can be used more predictably in younger children, patient cooperation may preclude such treatment. Alternatively, rapid palatal expansion can be achieved with an appliance utilizing a jackscrew, such as a Hyrax appliance, Haas-type appliance or Hawley-type appliance with a jackscrew.25 In the mandible, true bony expansion is not possible without surgical intervention because the mandibular symphysis fuses early in life.
Maxillary expanders often accompany Class II treatment to promote forward posturing of the mandible, as well as in treating Class III cases to activate bony sutures when maxillary protraction is needed. Cases involving bilateral posterior crossbites are more complex and require a careful determination of etiology and treatment planning.
10 Anterior Open Bite: The most common cause of an anterior dental open bite is nonnutritive sucking (NNS).26 Habits that persist beyond the age of 3 are more likely to cause dental and orthopedic effects.27 An anterior open bite can be caused by NNS, anterior maxillary growth deficiency, or a tongue-thrusting habit. There is controversy as to whether the open bite is secondary to a tongue-thrusting habit, or if tongue thrusting is compensatory for an anterior open bite. Dental findings for NNS primarily include flared upper incisors, retroclined lower incisors, increased overjet, a negative overbite, and maxillary constriction (due to recruitment of buccinator muscles).28 Tongue thrusting is usually accompanied by flaring of the maxillary and mandibular teeth, with a negative overbite.
A NNS habit can be curbed using behavioral or reminder therapy. In cases in which behavioral therapy or reminder therapy proves ineffective, and the child is motivated to stop, orthodontic appliance can serve as adjuncts to habit therapy.29
IN SUMMARY
Orthodontic challenges are relatively common in the primary and mixed dentition. Awareness of these conditions and approaches to treatment will allow clinicians to effectively screen for problems and make timely referrals to orthodontists when necessary. In addition, dentists should screen for other pathologies that may occur; although space limitations preclude a more detailed discussion, these include ankylosis, congenitally missing teeth and supernumerary teeth.
The decision for a nonorthodontist to treat orthodontic challenges is at the discretion of the provider and depends on the clinician’s knowledge and comfort level in providing interceptive treatment. While many patients undergo a single phase of comprehensive orthodontics, some will benefit from multiple phases of care. Early intervention is intended to reduce malocclusion, reduce the time needed for phase II treatment (if needed), or eliminate the need for comprehensive care altogether. Clinicians must develop a systematic approach to evaluating occlusion and make orthodontic evaluation part of every pediatric comprehensive and recall examination.
REFERENCES
- Proffit WR, Fields HW, Moray LJ Prevalence of malocclusion and orthodontic treatment need in the United States: estimates from the NHANES III survey. Int J Adult Orthod Orthognath Surg. 1998;13:97–106.
- American Dental Association Council on Scientific Affairs. The use of dental radiographs: update and recommendations. J Am Dent Assoc. 2006;137:1304–1312.
- Sayin M, Türkkahraman H. Factors contributing to mandibular anterior crowding in the early mixed dentition. Angle Orthod. 2004;74:754–758.
- Proffit W, Fields H. Contemporary Orthodontics. 5th ed. St. Louis, Mo: Elsevier Health Sciences; 2012.
- Gardner RB. A comparison of four methods of predicting arch length. Am J Orthod. 1979;75:387–398.
- Gianelly AA. Leeway space and the resolution of crowding in the mixed dentition. Semi Orthod. 1995;1:188–194.
- Dewel BF. Serial extraction in orthodontics: indications, objectives, and treatment procedures. Am J Orthod. 1954;41:906–926.
- Graber TM. Serial extraction: a continuous diagnostic and decisional process. Am J Orthod. 1971;60:541–575.
- Ngan P, Hu AM, Fields HW Jr. Treatment of class III problems begins with differential diagnosis of anterior crossbites. Pediatr Dent. 1997;19:386–395.
- Ulusoy AT, Bodrumlu EH. Management of anterior dental crossbite with removable appliances. Contemp Clin Dent. 2013;4:223–226.
- Kim JH, Viana M, Graber TM, Omerza FF, BeGole EA. The effectiveness of protraction face mask therapy: a meta-analysis. Am J Orthod Dentofacial Orthop. 1999;115:675–685.
- Liu ZP, Li CJ, Hu HK, Chen JW, Li F, Zou SJ. Efficacy of short-term chincup therapy for mandibular growth retardation in Class III malocclusion. Angle Orthod. 2011;81:162–168.
- Barberia-Leache E, Suarez-Clúa MC, Saavedra-Ontiveros D. Ectopic eruption of the maxillary first permanent molar: characteristics and occurrence in growing children. Angle Orthod. 2005;75:610–615.
- Kennedy DB, Turley PK. The clinical management of ectopically erupting first permanent molars. Am J Dentofacial Orthop. 1987;92:336–345.
- Miyamoto W, Chung CS, Yee PK. Effect of premature loss of deciduous canines and molars on malocclusion of the permanent dentition. J Dent Res. 1976;55:584–590.
- Rönnerman A. The effect of early loss of primary molars on tooth eruption and space conditions a longitudinal study. Acta Odontol Scand. 1977;35:229–239.
- Pedersen J, Stensgaard K, Melsen B. Prevalence of malocclusion in relation to premature loss of primary teeth. Community Dent Oral Epidemiol. 1978;6:204–209.
- Ngan P, Alkire RG, Fields H Jr. Management of space problems in the primary and mixed dentitions. J Am Dent Assoc. 1999;130:1330–1339.
- Ericson S, Kurol J. Early treatment of palatally erupting maxillary canines by extraction of the primary canines. Eur J Orthod. 1988;10:283–295.
- Baccetti T, Franchi L, McNamara JA Jr, Tollaro I. Early dentofacial features of Class II malocclusion: a longitudinal study from the deciduous through the mixed dentition. Am J Orthod Dentofacial Orthop. 1997;111:502–509.
- Keeling SD, Wheeler TT, King GJ, et al. Anteroposterior skeletal and dental changes after early Class II treatment with bionators and headgear. Am J Orthod Dentofacial Orthop. 1998;113:40–50.
- Petrén S, Bondemark L, Söderfeldt B. A systematic review concerning early orthodontic treatment of unilateral posterior crossbite. Angle Orthod. 2003;73:588–596.
- Myers DR, Barenie JT, Bell RA, Williamson EH. Condylar position in children with functional posterior crossbites: before and after crossbite correction. Pediatr Dent. 1980;2:190–194.
- Lagravère MO, Major PW, Flores-Mir C. Skeletal and dental changes with fixed slow maxillary expansion treatment: a systematic review. J Am Dent Assoc. 2005;136:194–199.
- Agarwal A, Mathur R. Maxillary expansion. Int J Clin Pediatr Dent. 2010;3:139–146.
- Ngan P, Fields HW. Open bite: a review of etiology and management. Pediatric Dent. 1997;19:91–98.
- Warren JJ, Bishara SE. Duration of nutritive and nonnutritive sucking behaviors and their effects on the dental arches in the primary dentition. Am J Orthod Dentofacial Orthop. 2002;121:347–356.
- Heimer MV, Tornisiello Katz CR, Rosenblatt A. Non-nutritive sucking habits, dental malocclusions, and facial morphology in Brazilian children: a longitudinal study. Eur J Orthod. 2008;30:580–585.
- Turgeon-O’Brien H, Lachapelle D, Gagnon PF, Larocque I, Maheu-Robert LF. Nutritive and nonnutritive sucking habits: a review. ASDC J Dent Child. 1996;63:321–327.
Featured Image by J2R/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. September 2018;4(9):30–32,35.

