

Precision Pathways to Predictable Occlusal Guard Therap
A step-by-step clinical framework for capturing accurate centric relation, deprogramming musculature, and designing canine-guided occlusal guards.
PURCHASE COURSE
This course was published in the February/March 2026 issue and expires March 2029. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the February/March 2026 issue and expires March 2029. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 180
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Explain the biomechanical and electromyographic rationale for incorporating canine guidance into occlusal guard design.
- Identify a systematic protocol for using a leaf gauge to deprogram musculature, obtain a repeatable centric relation bite registration, and digitally capture an accurate interocclusal record.
- Discuss evidence-based equilibration principles to fabricate and adjust a hard occlusal guard.
Occlusal guards play a crucial role in treating myofascial pain, nocturnal bruxism, clenching, and occlusal-incisal attrition in both adults and children.1,2 Capturing an accurate centric relation (CR) bite registration is critical for making and equilibrating an occlusal guard. A properly designed CR occlusal guard manages bite forces by loading the temporomandibular joints (TMJs) with all teeth contacting simultaneously.
A study of bite forces by Manns et al3 compared electromyographic (EMG) activity in patients exhibiting canine guidance with that in patients displaying group function. During working and nonworking excursions of the mandible, both the masseter and temporalis muscles work half as much in canine guidance as in group function. The decrease in muscle contractions among the elevator muscles resulted from the lack of posterior tooth contacts. A later EMG study by Manns et al4 concluded that elevator muscle contractions and joint health depend on posterior tooth contacts and canine guidance functioning to prevent posterior tooth contacts during excursive movements of the mandible.
These findings make a compelling case for designing canine guidance in occlusal guards for patients with myofascial pain. Canine guidance results in the temporalis and masseter muscles releasing their contractions (ie, becoming more relaxed) and the inability to exert the magnitude of harmful forces on teeth and restorations as when posterior interferences are present. The efficacy of therapy with an occlusal guard (ie, how effectively it relaxes the elevator muscles [masseter, temporalis, medial pterygoid, and superior belly of the lateral pterygoid]) depends on how accurately it is equilibrated and on the level of patient compliance.
Introduction of Leaf Gauges
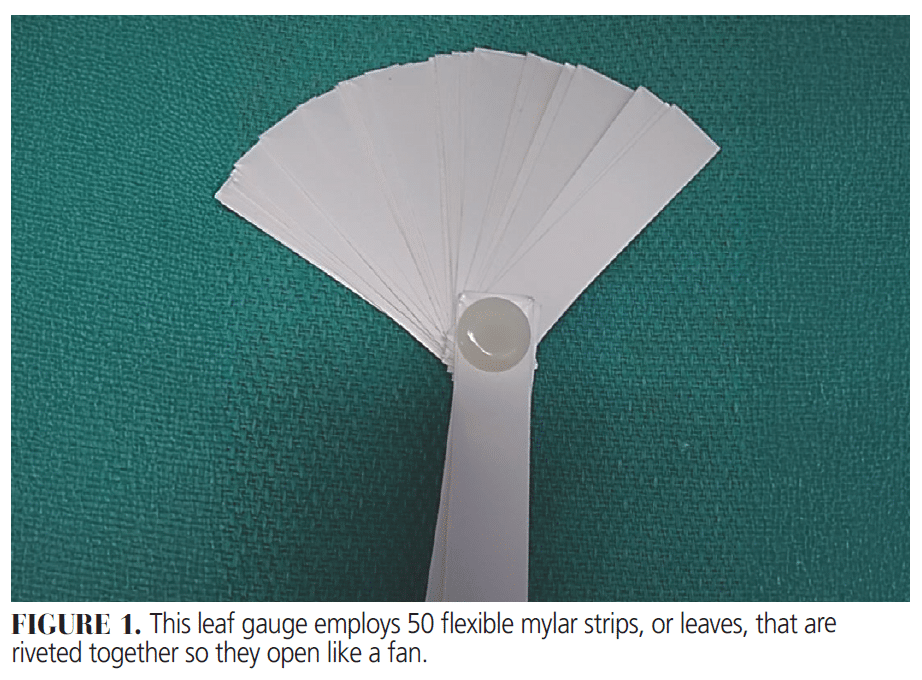
In 1973, Long5 introduced leaf gauges to facilitate the separation of posterior teeth to locate CR. A popular brand of leaf gauges employs 50 flexible mylar strips, or leaves, that are riveted together so they can open like a fan (Figure 1). The leaves are approximately 0.1 mm thick, 13 mm wide, 60 mm long, and autoclavable.
A leaf gauge is an occlusal stop; it is placed in the anterior section of the mouth, between the maxillary central incisors, to eliminate posterior deflective occlusal interferences to CR. The patient is then directed to attempt to occlude on the posterior teeth. With the leaf gauge properly placed at the midline, between the central incisors,the posterior teeth are separated while maintaining the tripodization of the mandible (ie, the narrow anterior stop forms a tripod effect between the anterior teeth and the two condyles in their respective positions in the glenoid fossae). When this condition exists, the mandible is said to be “tripodized.” Maintaining this separation for 5 to 15 minutes will allow patients’ elevator and lateral pterygoid muscles to deprogram from their existing deflective occlusal contacts.6 Subsequently, these muscles adapt to their new environment by changing their contraction activity and changing the position of the mandible.
Technique for Using the Leaf Gauge
Following are the appropriate steps to using the leaf gauge to digitally record CR and equilibrate a maxillary occlusal guard.
- After both dental arches have been digitally scanned, use a leaf gauge to create an interocclusal CR record at a vertical dimension (VD) that provides sufficient space between posterior teeth for the thickness of an occlusal guard. Enough leaf gauges should be used to allow 2 to 3 mm of clearance between the first molars. Incisal openings of 3 and 4 mm are approximately equivalent to first molar openings of 2 and 3 mm, respectively.)
- Position the patient in the dental chair with the head tipped back approximately 30° to 45°. Place the leaf gauges in the mouth and ask the patient if any posterior teeth are contacting. Use shim stock to check this. To ensure that the condyles are not deflected away from the condylar braced position in the fossae, ask the patient to first protrude and then retrude the mandible, and then bite on the leaves with a “half-hard” bite (ie, a bite force that is the same as that exerted when he/she is swallowing). Again, use shim stock to check for unwanted posterior tooth contacts.
If tooth contacts are detected, then add additional leaves until the patient no longer feels any posterior contacts. As the elevator muscles deprogram (relax), the mandible changes position, and new posterior tooth contacts could become evident when checking with shim stock. This occurs as the relaxed muscles seat the condyles in their CR positions in the fossae, bringing the teeth closer together.
Simultaneously, new posterior contacts could become evident when checking with shim stock. After 30 seconds, if the patient feels a posterior tooth contact because of the relaxation of the elevator muscles, add leaves, one at a time, until the patient can bite for 2 to 5 minutes without sensing any posterior contact. During that time, instruct the patient to hold the leaf gauge in the retruded position with a half-hard bite.
Repeated checks with shim shock are required to make sure no posterior tooth contact occurs. The patient must not exert excessive biting force on the leaf gauge, as this can cause the condyles to move inferiorly and posteriorly. This could also occur if the mandible is not maintained in its midmost position as the patient occludes on the leaf gauge. The time needed to accomplish this procedure will vary depending on the degree of muscle tension and the psychological state and cooperativeness of the patient.
The position of the condyles while the posterior teeth no longer touch is considered a braced or seated CR position that is made possible when the muscles are no longer influenced by their deflective malocclusion. Protrusion of the mandible, along with the simultaneous distraction of the condyles from the fossae, may be avoided with this technique because contraction of the lateral pterygoid muscles is diminished as the patient bites firmly on the leaf gauge.7,8
- The leaf gauge should be left in the mouth for at least 5 minutes to allow the muscles to deprogram. As new posterior contacts could become evident when checking with shim stock, the required vertical distance between the first molars decreases. At that point, add enough leaves to reestablish the 2- to 3-mm clearance requirement for an occlusal guard. Then check again with shim stock.
If mild tenderness or tension is noted in the TMJ area while the patient is biting on the leaf gauge — secondary to muscle strain — then ask the patient to protrude and retrude the jaw and then bite. When no tenderness or tension is recognized, the condyles are likely in the correct CR position for therapy with an occlusal guard, and an interocclusal bite registration could be recorded.
- Scan both dental arches. Then, with the leaf gauge in place and providing an interocclusal distance of approximately 3 mm between the first molars, scan the right and left buccal sides (ie, the buccal bite) of the posterior teeth (Figure 2).
At this point, the scans are ready to go to the dental laboratory for the fabrication of an occlusal guard. The prescription should instruct the laboratory to incorporate the following design features in the guard:
- All functional cusp tips should contact the guard evenly and simultaneously in CR.
- The acrylic prominences built into the guard in the canine areas should be angulated approximately 30° to 45° to the occlusal plane to allow the mandibular canines to disclude posterior teeth during laterotrusive movements.
- The canines and as many incisors as possible should contact during protrusive movement for incisal guidance.
- Only the mandibular canines should contact during canine-guided movements.
- The occlusal guard should not move during CR closure or any eccentric jaw movement.9
![]() When the guard is delivered and fits properly without rocking, the leaf gauge is inserted between the maxillary incisors. Add enough leaves to eliminate any posterior contact between the guard and the mandibular teeth. Follow the instructions described in step 2 to allow the muscles to deprogram. If the posterior teeth contact the guard, then increase the number of leaves to separate the teeth. Verify this with shim stock. To relax the muscles, permit the patient to bite on the gauge for 5 minutes.
When the guard is delivered and fits properly without rocking, the leaf gauge is inserted between the maxillary incisors. Add enough leaves to eliminate any posterior contact between the guard and the mandibular teeth. Follow the instructions described in step 2 to allow the muscles to deprogram. If the posterior teeth contact the guard, then increase the number of leaves to separate the teeth. Verify this with shim stock. To relax the muscles, permit the patient to bite on the gauge for 5 minutes.- To bring the guard into equilibrium, gradually decrease the number of leaves until the first point of contact on the guard can be detected with shim stock. Mark the contact with the blue side of thin articulating ribbon. Remove the guard and lightly adjust the contact with a football-shaped stainless steel laboratory bur until additional blue CR contacts appear on the guard. Do not create deep concavities in the guard when adjusting the contacts. To ensure continued muscle deprogramming while adjusting the guard outside the patient’s mouth, place the leaf gauge in the mouth to prevent the teeth from contacting.
- Reinsert the appliance and assess additional contacts on the guard by subtracting one leaf at a time. Use the same procedure outlined in step 6. The muscles should be reprogrammed, also known as “intervening deprogramming,”throughout the process of adjusting the guard by providing additional 1-minute periods of deprogramming after every subtraction of two to three leaves. This enables the patient to be maintained more accurately in the CR position.6
- At an opening of approximately two leaves, continue subtracting leaves and assess with shim stock until all opposing mandibular functional (buccal) cusp tips contact simultaneously and evenly on the guard in CR. Adjust the anterior ramp of the guard to ensure there is immediate comfortable anterior disocclusion of the posterior teeth during protrusive, working, and nonworking excursions of the mandible.10
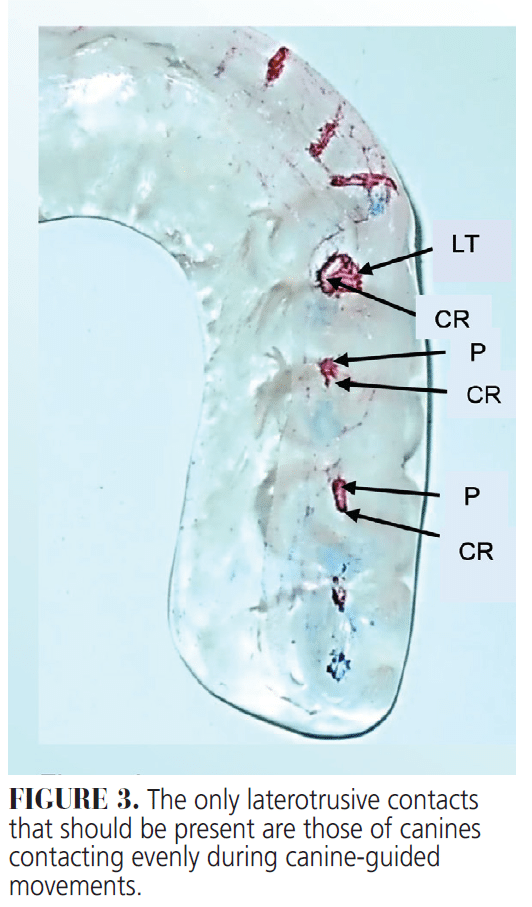
The only laterotrusive contacts that should be present are those of canines contacting evenly during canine-guided movements (Figure 3). No additional adjustments of the guard are needed when one or two leaves will separate the mandibular posterior teeth from the guard when the mandible is in CR.
- Areas on the guard where contacts were adjusted should not be polished as this could result in the loss of CR contacts. The minor roughness produced by the fluted laboratory carbide bur will not harm opposing enamel; we have never encountered a patient who became uncomfortable because of the slight roughness generated by adjustments with a bur.
- Follow-up care is recommended in 1 to 3 weeks when the patient fails to demonstrate any of the occlusal contacts on the guard mentioned in step 8. If a minor adjustment is needed, it may be completed using the method outlined above.
Discussion
Soft occlusal guards have been prescribed for various reasons; however, they are not recommended for patients with myofascial pain because they tend to increase masseter muscle activity during maximum clenching.11 A properly equilibrated hard occlusal guard decreases EMG activity in both masseter and temporalis muscles.12
The interocclusal bite registration record is the most important record obtained in restorative dentistry, and neuromuscular relaxation is a vital part of a physiologically sound interocclusal bite registration recording protocol. The CR system described here is free from all posterior tooth contacts or interferences. A leaf gauge between the anterior teeth helps the patient retrude the mandible while recommended biting forces of closure relax the elevator and lateral pterygoid muscles to permit the condyle-disk assembly to remain against the posterior slope of the articular eminence, and to maintain the desired minimal vertical opening.
Thin, flexible leaf gauges result in minimal incisal opening, and they readily conform to the concave palatal surfaces of maxillary incisors. When the mandibular incisors exert force against the steep guidance created by the gauge above the occlusal plane, the mandible rotates the condyles into the anterior-superior part of the articular fossae.
Use of a leaf gauge allows the patient to position the mandible without help from the dentist; it helps to overcome operator error that occurs when the dentist must manipulate the patient’s mandible to guide it to CR, which is the greatest difficulty encountered when attempting to equilibrate a patient’s occlusion. When coupled with bilateral mandibular manipulation, as advocated by Dawson,13 leaf gauges are especially helpful in obtaining a CR bite registration and transferring it when mounting a patient’s cast or scan on an actual or virtual articulator, respectively.
At our university, under the supervision of prosthodontic faculty members, preclinical (D2) students practice bilateral mandibular manipulation on each other and learn how to use leaf gauges to obtain accurate CR interocclusal bite registrations to mount casts in their articulators.
If conventional bite registration materials (eg, polyvinyl siloxane, polyether, acrylic resin, or wax) are used to capture a CR bite registration to mount casts, polyvinyl siloxane is the most accurate, as it produces the least vertical error (24 µm), followed by polyether (30 µm), acrylic resin (57 µm), and wax (74 µm).14 No occlusal adjustment procedures should be attempted before the dentist has properly mounted casts on an articulator.
Leaf gauges could be used in occlusal therapy to periodically relieve painful spasms of the lateral pterygoid muscles, thereby eliminating the need for occlusal guards or the use of drugs to reduce muscle contractions.7 All occlusal discrepancies must be eliminated before any extensive restorative dental treatment. Any muscle strain caused by the leaf gauge may not result in a repeatable CR braced position of the condyles because of damage existing in the muscles, ligaments, or osseous structures.15
The leaf gauge system is pleasant for the patient, accurate, inexpensive, and adaptable to most occlusal schemes. Leaf gauges, however, may be contraindicated for patients with Class II, Division II malocclusion, as the condyles might be displaced downward and posteriorly when an inclined plane, such as a leaf gauge, is inserted between the maxillary incisors.13 A leaf gauge might also be ineffective in severe Class III malocclusions, where it might be necessary to use a very thick gauge.8 When a large discrepancy in the CR-to-maximum intercuspal position (ie, a large CR-maximum intercuspal position shift of more than 2.5 mm of incisal separation) is discovered by using the leaf gauge, it might not be possible to eliminate the discrepancy without orthodontic or surgical intervention.
References
- Solberg WK, Clark GT, Rugh JD. Nocturnal electromyographic evaluation of bruxism patients undergoing short term splint therapy. J Oral Rehabil. 1975;2:215-223.
- Hachmann A, Martins EA, Araujo FB, et al. Efficacy of the nocturnal bite plate in the control of bruxism for 3 to 5 year old children. J Clin Pediatr Dent. 1999;24:9-15.
- Manns A, Chan C, Miralles R. Influence of group function and canine guidance on electromyographic activity of elevator muscles. J Prosthet Dent. 1987;57:494-501.
- Manns A, Miralles R, Valdivia J, et al. Influence of variation in anteroposterior occlusal contacts on electromyographic activity. J Prosthet Dent. 1989;61:617-623.
- Long JH Jr. Locating centric relation with a leaf gauge. J Prosthet Dent. 1973;29:608-610.
- Fleigel, III JD, Sutton AJ. Reliable and repeatable centric relation adjustment of the maxillary occlusal device. J Prosthodont. 2013;22:233-236.
- Carroll WJ, Woelfel JB, Huffman RW. Simple application of anterior jig or leaf gauge in routine clinical practice. J Prosthet Dent. 1988;59:611-617.
- Woelfel JB. New device for accurately recording centric relation. J Prosthet Dent. 1986;56:716-727.
- Antonelli J, Hottel TL, Siegel SC, et al. The occlusal guard: a simplified technique for fabrication and equilibration. Gen Dent. 2013;61:49-54.
- Antonelli JR. Selectively equilibrating the hard occlusal guard. Today’s FDA. 2019;31:92-95.
- Cruz-Reyes RA, Martínez-Aragón I, Guerrero-Arias RE, García-Zura DA, González-Sánchez LE. Influence of occlusal stabilization splints and soft occlusal splints on the electromyographic pattern, in basal state and at the end of six weeks treatment in patients with bruxism. Acta Odontol Latinoam. 2011;24:66-74
- Al-Quran FAM, Lyons MF. The immediate effect of hard and soft splints on the EMG activity of the masseter and temporalis muscles. J Oral Rehabil. 1999;26:559-563.
- Dawson PE. Functional occlusion from tmj to smile design. In: Recording Centric Relation. 3rd ed. St. Louis: Elsevier Inc; 2007:92-101.
- Kattadiyil MT, Alzaid AA, Campbell SD. What materials and reproducible techniques may be used in recording centric relation? best evidence consensus statement. J Prosthodont. 2021;30:34-42.
- Olsen LF, Shaw AF. Use of leaf gauge in occlusal diagnosis and therapy. Quintess Int. 1984;7:611-621.
From Decisions in Dentistry. February/March 2026;12(1):40-45.

