
My Go-To for Tough Extractions
Extraction cases that once filled me with dread are now met with confidence thanks to ArtCraft Dental’s Xpanders.
 Extractions are procedures that simultaneously fill me with excitement and dread. To ensure success of my technique, I have upgraded my armamentarium to include the Xpanders from Artcraft Dental. Appearing similar to a 301, Xpanders have a bulbous handle that extends into a round shank that develops a concave and convex semicircle shape at the tip. However, Xpanders have a two-pronged tip instead of a standard shovel shape that makes them more specialized for extreme elevations. Curved to engage the root surface, they’re treated with a proprietary ceramic material that enhances grip during vertical elevation, allowing quicker, more focused penetration of the periodontal ligament (PDL) space.
Extractions are procedures that simultaneously fill me with excitement and dread. To ensure success of my technique, I have upgraded my armamentarium to include the Xpanders from Artcraft Dental. Appearing similar to a 301, Xpanders have a bulbous handle that extends into a round shank that develops a concave and convex semicircle shape at the tip. However, Xpanders have a two-pronged tip instead of a standard shovel shape that makes them more specialized for extreme elevations. Curved to engage the root surface, they’re treated with a proprietary ceramic material that enhances grip during vertical elevation, allowing quicker, more focused penetration of the periodontal ligament (PDL) space.
Although crafted from surgical-grade French stainless steel, Xpanders are still lightweight and ergonomic. The handles are easy to grip, and the hollow interior ensures airtight sterilization. I’ve yet to bend or break the tips, even when applying considerable force. The Xpanders excel in creating a two-point contact: one tip establishes a purchase point, while the other provides the force necessary for root movement and expulsion.
Tooth elevation works by generating a lever action to lift the tooth against the bone. The Xpanders’ double-pronged design nearly doubles the lever action, making them ideal for tight spaces. Thanks to their ceramic coating, which enables a strong grip, Xpanders are my first choice for elevation when there’s at least 2 mm of ferrule above the bone. If the tooth is level with or below the bone, I opt for a PDL knife, luxator, or spade elevator.
Standard Protocol for Extractions
- Effective anesthesia
- Periosteal elevation
- Radicular stability test
- Evaluation of ferrule to assess purchase point for elevation
- Use of spade, PDL knife, or Xpanders for luxation
- Vertical apically directed force with a ¼ turn reciprocal twist on four interproximal corners
- Reintroduce a standard elevator if the PDL space is wide enough
- If the root is mobile, secure with 151 or 150 forceps
- Remove the tooth or root
- Curette the socket
- Place collagen or graft and close with membrane and sutures
If a tooth shows significant instability with an instrument, I proceed with removal. While the most atraumatic extraction uses only a periosteal, Xpanders provide a rugged option for tougher cases that may require troughing, sectioning, or bone removal.

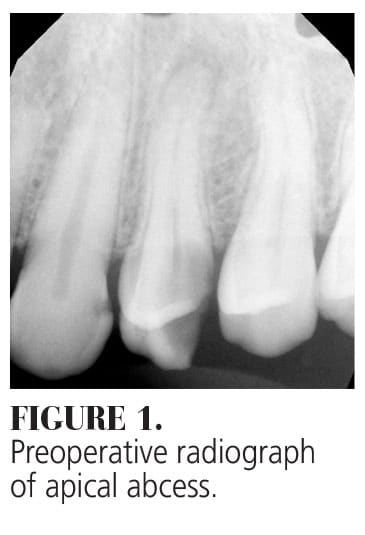
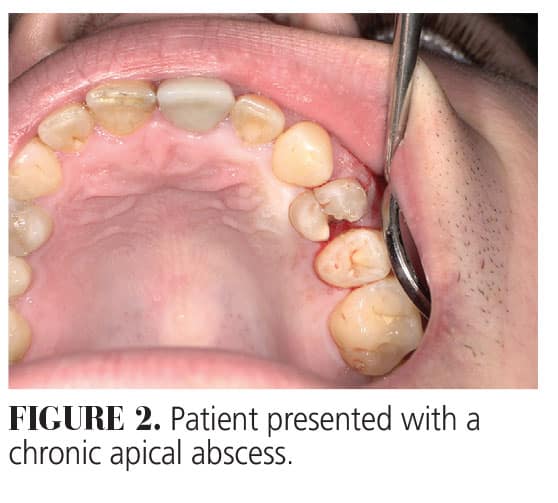
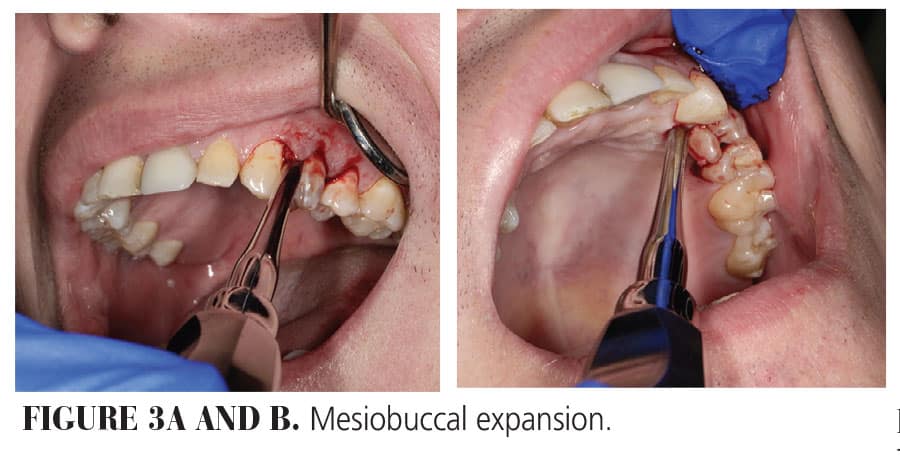
Case Study #1. A 34-year-old man presented with a chronic apical abscess that required extraction of #12, which had led to significant swelling (Figures 1 and 2). I prescribed antibiotics and steroids, and a week later, proceeded with the extraction and grafting. After anesthetizing the site, I lifted the gingiva and periosteum. I inserted a 301 to create horizontal mobility, then used the straight Xpanders at the mesiobuccal corner (Figure 3A and B), applying vertical pressure with ¼-turn twists. After increasing mobility, I moved to the mesiolingual corner and completed the same motion. The distobuccal corner had decay, so I used a spade elevator to gain access, followed by the Xpanders. After some fractures in the coronal portion, I re-engaged the Xpanders, driving them apically until the root rose coronally. The root was removed, and the site was cured and grafted (Figure 4). The extraction was minimally traumatic, completed in 15 minutes. In this case, I was able to perform a minimally traumatic extraction and complete the procedure efficiently.
Case Study #2. The second case involved a 39-year-old man with no significant medical history or medication use. Tooth #15 had a history of root canal treatment and crown. The patient was seen at a previous appointment by my associate with the crown off and significant recurrent decay diagnosed on the mesial aspect from a food pack. The failure of the crown rendered the tooth nonrestorable but it was recemented and the patient was scheduled with me for the extraction (Figure 5A and B).
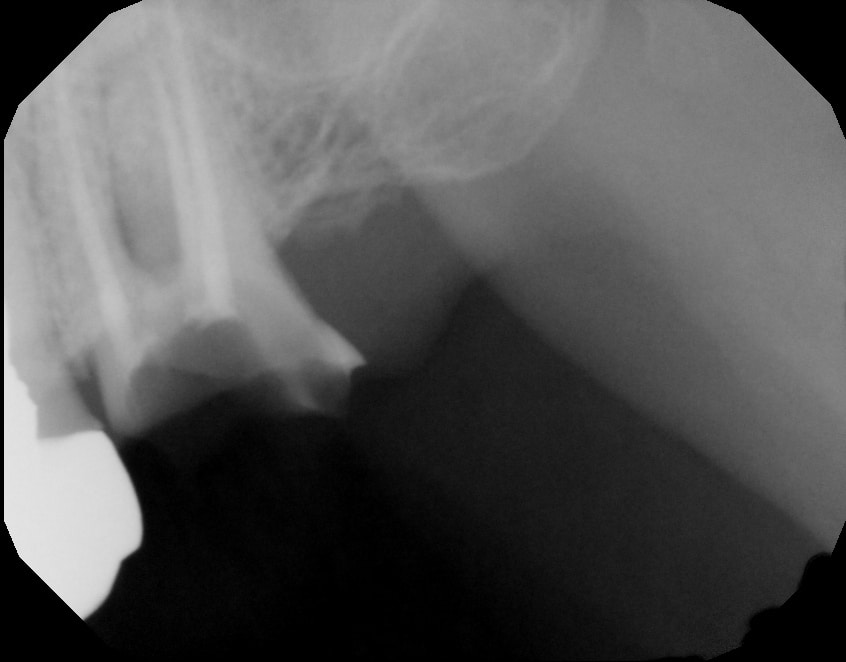

Figure 5 A and B. Pre-op from previous appointment.
There was no swelling or purulence so effective anesthesia only required two carpules of infiltration with articaine, hydrochloride, and epinephrine. I began with circumferential periosteal elevation and then progressed to my Xpanders set (Figure 6). I was able to use the “Posterior In” Xpander to get a good purchase point on the mesiobuccal corner of the mesiobuccal root and worked that angle until the crown popped off (Figure 7 A and B).

Figure 6. Periosteal elevation.
I typically plan to section the roots of molars prior to elevation. However, since there was extensive decay and it was root canal treated, I correctly predicted the cemented crown would not hold up to pressure and provide me with greater visibility for sectioning. I prefer sectioning prior to periosteal elevation because even though I utilize a reverse vent air-driven surgical handpiece, I still like to maintain a periosteal seal as much as possible to prevent pneumonias from debris, air, or water into the fascial planes.


Figure 7 A and B. Mesiobuccal Xpansion prior to crown removal.
I completed a y-shaped sectioning of the roots with my handpiece and was then able to engage the distobuccal root on its mesiobuccal corner. This quickly created instability and I removed the distal root with the Xpanders only. The decay on the mesial root caused repeated fracturing upon elevation force and necessitated further troughing and osseous reduction.
Final removal of the apical portion required root picks. The palatal root was easier to access with the “Posterior Out” Xpander on the distolingual aspect and the “Posterior In” Xpander on the mesiolingual and moved buccally enough to allow for removal with a set of 150 forceps. The patient elected not to graft at this location so hemostasis was confirmed and the patient released (Figure 8A and B).
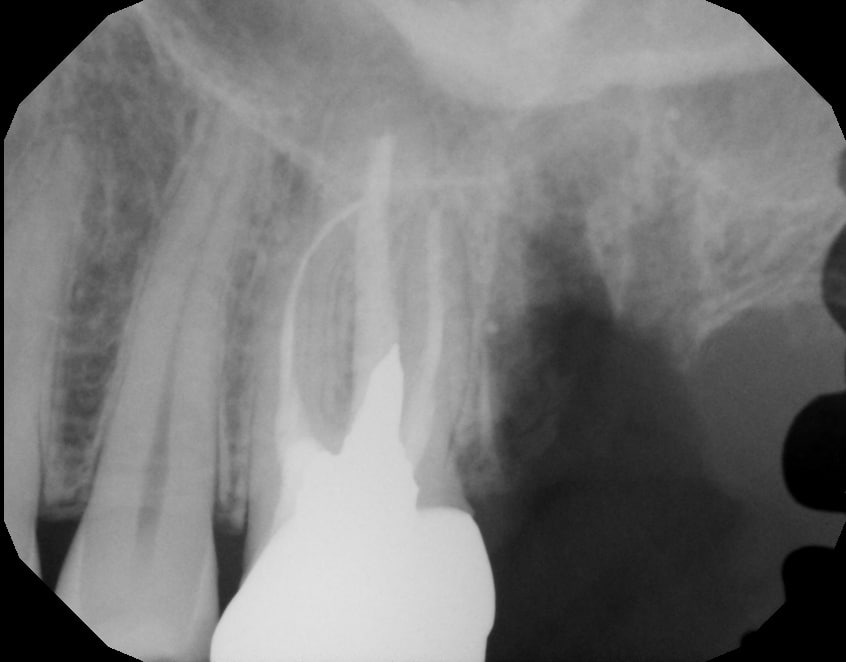

Figure 8 A and B. Post-op.
In the first case, I was successful at completing a minimally traumatic extraction that did little damage to the surrounding bone and was able to complete the procedure in only about 15 minutes. I then treated the site with ridge regeneration techniques for future restoration. The second case was significantly more challenging but I achieved success through implementation of a good plan with great instruments.
By describing my personal style and use of the Xpanders system from Artcraft Dental, I hope you can understand why I consider them a critical part of my surgical set up. I think you will find that incorporating them into your kit will elevate your experience as well.
ArtCraft Dental Inc
artcraftdental.com
877-340-1776
From Decisions in Dentistry. May/June 2025;11(3):23.
