
TMD Demystified: Practical Diagnosis and Conservative Management
Move beyond referral-only thinking with clear screening, diagnostic loading, and conservative strategies to manage temporomandibular joint disorders confidently in general practice.
PURCHASE COURSE
This course was published in the February/March 2026 issue and expires March 2029. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the February/March 2026 issue and expires March 2029. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 200
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Differentiate muscle-related temporomandibular joint disorders (TMDs) from other conditions using structured screening, comprehensive history-taking, and focused clinical examination.
- Identify diagnostic loading techniques to reproduce symptoms and guide evidence-based treatment.
- Discuss a conservative management plan for muscle-related TMDs.
Despite substantial evidence to support early, conservative management, temporomandibular joint disorders (TMDs or TMJDs) remain one of the most common reasons for referral to dental/medical specialists in the United States.1 TMDs comprise a subset of orofacial pain conditions affecting the masticatory muscles and/or temporomandibular joints.
Dental school education often focuses on screening and referral as management for TMDs. This approach relies on geographic and financial access to a provider offering TMD treatment. As their community’s primary dental provider, general dentists are frequently left with few practical options to help patients with TMD. This is exacerbated by the potential for TMDs to worsen if not properly managed during the initial presentation.
Much of the confusion over the diagnosis and management of TMDs comes from the prevalence of comorbidities and difficulty in distinguishing TMJ dysfunction and associated musculature from other complex orofacial pain conditions. Common screening questions focus on pain in/around the TMJ area, type and location of headaches, abnormal or limited jaw function as noted with difficulty eating, limited opening, getting stuck open or closed, popping/clicking/grating sounds, history of injury to face/head or neck, and time of symptom onset.2 Patients are also asked about changes in their bite or face shape. Oral health professionals should include comprehensive screening questionnaires for TMDs and known comorbidities as part of their regular dental intake exams before initiating treatment (Table 1).
Any affirmative response on the patient questionnaire warrants further discussion, followed by clinical examination. The initial assessment should include panoramic radiographic examination; evaluation of TMJ function through measurement of maximum comfortable opening; palpation of TMJs during opening; listening to TMJs using a stethoscope (especially for grating sounds characteristic of bony degradation); and evaluation of face shape, interarch relationships, and symmetry both at rest and during mandibular function.
Acute Patient
Muscle-related disorders, including myalgias and myofascial pain, are commonly seen in general practice settings.5,6 Patients often present with recently developed symptoms, as longer-standing TMD tends to progress to joint-related problems due to structural changes. The primary symptoms of muscle-related disorders are pain in masseteric and temporalis muscles and perceived limitation of function.
Referred pain in other muscles of the masticatory system and the area of the TMJs may also be noted. The location of pain can be confirmed by palpation, especially for the masseter and temporalis.6 Patients commonly report the onset of these symptoms following some triggering event, such as a long dental appointment or psychological stress associated with parafunctional habits.
Daytime and/or nighttime clenching and bruxism are also correlated. Limited opening may be noted by the patient or measured clinically to be less than 40 mm from incisal edge to incisal edge. Variation in the degree of pain experienced throughout the day frequently depends on activities and level of psychological stress. Patients often express a sensation of fullness in the ears and occasionally report tinnitus. Deviation upon opening can occur with asymmetric muscle spasm, necessitating re-evaluation of the medical history for a systemic etiology. Patients who clench and brux may report a change in the shape of their face due to hypertrophy of masticatory muscles. Clinicians may observe signs of wear and damage to the dentition.
Importance of Diagnostic Loading
The value of mechanically loading the TMJs is immeasurable. We believe that true TMDs involving the masticatory muscles and/or TMJs cannot be clearly differentiated from other orofacial pain conditions without this diagnostic tool. Various methods have been described using some means to position the mandibular condyles in centric relation (bimanual manipulation, chin point guidance, anterior jig, etc) and modestly load the TMJs with force to reproduce the patient’s symptoms.7-9
If performed effectively and with care, both muscle- and TMJ-related pain can be easily identified, providing the clinician with a specific direction for treatment. James Metz, DDS, of Columbus, Ohio, and the late Bill McHorris, DDS of Memphis, Tennessee, developed a protocol using a leaf gauge to load the TMJs.10-12 This method has proven reliable in identifying whether conservative occlusal splint therapy may be helpful.
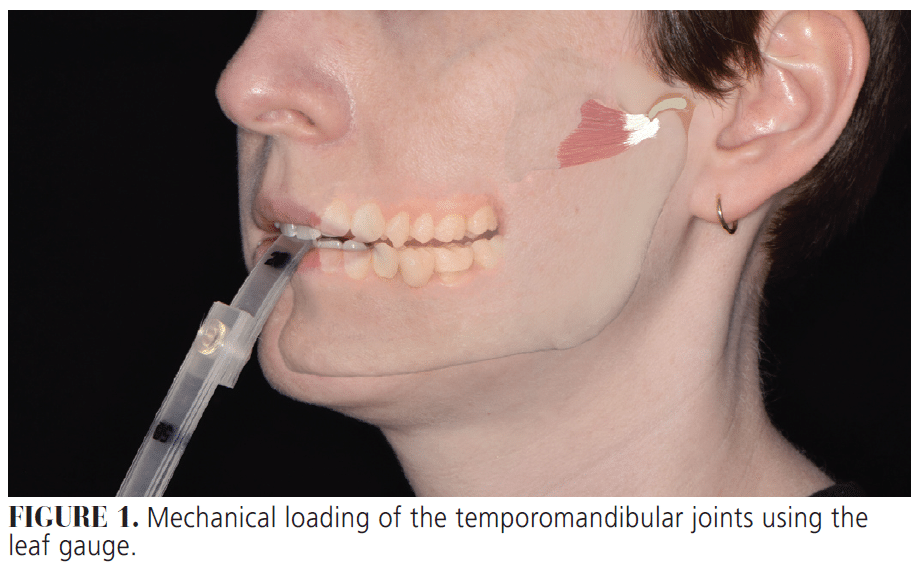
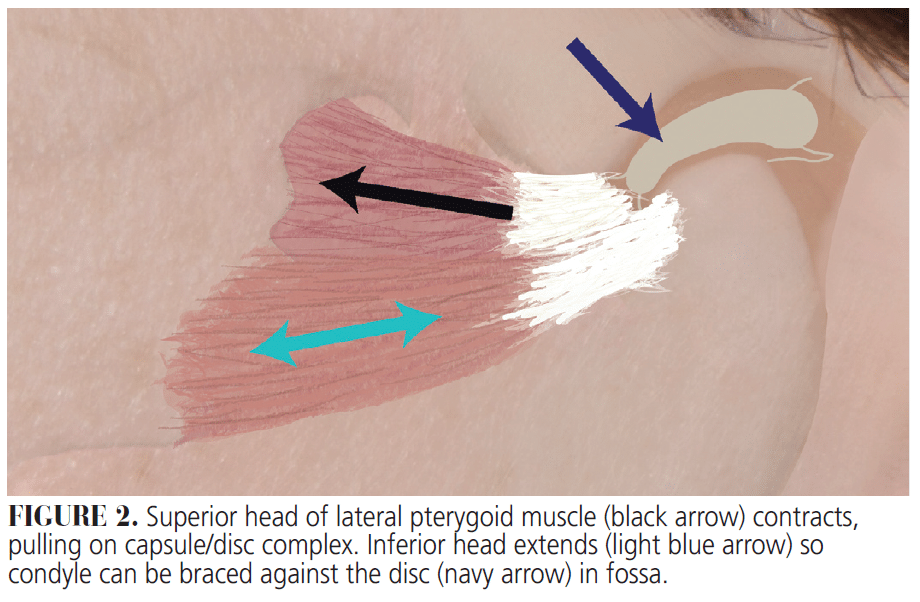
To use the leaf gauge, the patient is instructed to bite on a select number of leaves (20 to 25 leaves is often a good starting point) with anterior teeth, then protrude the mandible, followed by retrusion (Figure 1). The leaf gauge must be positioned at the maxillary midline. The mandible is then held in centric relation position with a mild-to-moderate squeezing force on the leaf gauge. This causes bilateral contraction of lateral pterygoid and temporalis muscles (Figure 2). The lateral pterygoids are involved with normal and abnormal movement of the condylar-disc complex. The patient must not squeeze with full force but should be squeezing tightly enough so that the leaf gauge does not slide out if gently tugged on. The patient then holds this position for 7 to 10 minutes, unless acute pain develops. During this time, the clinician must periodically check that posterior teeth do not begin to contact as the condyle seats further into the fossa. If tooth contact does develop, additional leaves are added, and the process is repeated. If a patient develops pain, the clinician should palpate muscles and joints to locate the pain and establish severity. If/when the patient develops acute pain, the leaf gauge may be removed, and the patient is asked to report when the pain dissipates.
Patients with a TMJ problem will develop acute pain almost instantly when loaded on the leaf gauge. For these individuals, the TMJ loading test will reveal pain that tends to linger after removing the leaf gauge. This pain may be quite severe, so patients should be warned at the outset of the need to diagnostically reproduce their symptoms.
Patients with muscle problems typically feel pain come on slowly over several minutes. For these patients, the pain will usually dissipate over a few minutes upon removal of the leaf gauge. It is not uncommon for these patients to also have reported some mild TMJ clicking/popping caused by extended partial contraction of the superior head of the lateral pterygoid muscle and slight dislocation of the disc, resulting in the condyle clicking past the edge of the discal tissue.11 If managed early, these patients may return to normal function and experience resolution of the clicking/popping. However, if left untreated, long-term damage to connective tissues results in more severe issues.
Related Symptoms
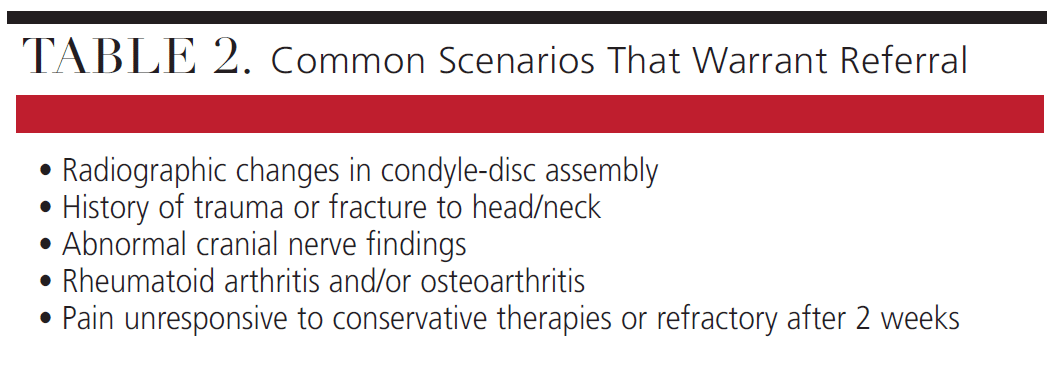
Patients presenting with TMD symptoms following physical trauma (such as a car accident), with clinical evidence of a joint problem, or with systemic medical conditions known to involve the TMJ (eg, rheumatoid arthritis or osteoarthritis) may warrant referral to an orofacial pain specialist or oral surgeon (Table 2). Other medical specialties may also need to be engaged. Clinical evidence of a chronic joint problem can include grating sounds, or crepitus, upon evaluation of TMJ with a stethoscope and evidence of condyle degradation on panoramic radiograph (eg, “beaking” and radiographically visible disruption of corticated bone on condyle). Patients with long-term degeneration of some component of the TMJ do not always present with pain or clinically evident limitation of function. For symptomatic individuals, load testing will quickly produce severe and lingering pain.
Role of the Airway
The airway potentially plays a significant role in the development and progression of TMDs. Research indicates a frequent co-occurrence of sleep-disordered breathing (including sleep apnea and bruxism) and TMDs.13,14 Therefore, screening for obstructive sleep apnea (OSA) risk factors, such as those identified with the STOP-BANG questionnaire, should be included in every TMD evaluation.
Patients with positive risk factors should be referred to a sleep physician for further evaluation. Importantly, upper airway resistance syndrome (UARS), a condition often undetected by traditional sleep studies, might manifest as TMD symptoms.15 Oral health professionals should consider the impact of OSA and UARS on TMD treatment, including splint design and treatment duration. For example, increasing the vertical dimension of occlusion or excessive bulk of an occlusal splint could negatively affect airway patency due to alterations in tongue and mandible position.16
Conversely, appropriately designed and titrated oral appliances can effectively manage both TMD and sleep-disordered breathing, improving overall health and quality of life.17 Ongoing research will likely yield further insights and recommendations regarding the interplay between TMD and airway health.
Clinical Management
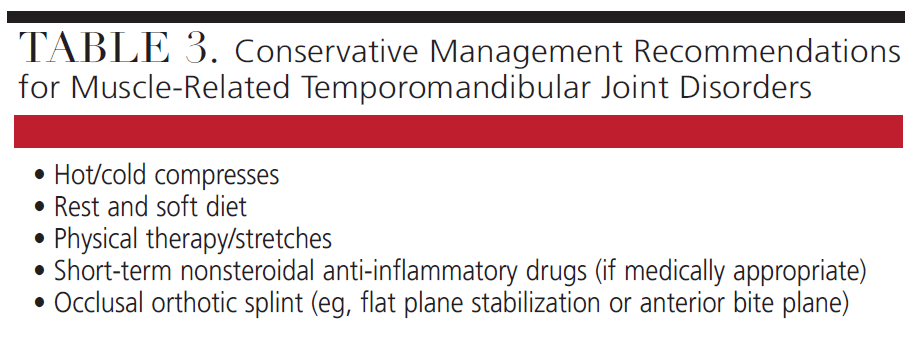
For most patients with muscle-related TMD, a combination of palliative self-care, anti-inflammatory medications, and conservative occlusal splint therapy will be sufficient (Table 3).3 Palliative measures include rest, soft diet, and hot or cold compresses. Exercises involve opening and moving the lower jaw laterally while applying light resistance by hand. Caution is recommended with at-home exercises, as some patients will attempt to strain or open the jaw forcefully or beyond normal physiological limits, which can damage the TMJ over time. Opening excessively when yawning is discouraged; instructing patients to use their fist to limit the opening until they can train themselves not to open so wide is an option.
Some providers may prescribe a short-term regimen of a low-dose skeletal muscle relaxer, such as cyclobenzaprine, though most of the time it is not necessary. Oral steroid use can be beneficial for some patients. However, providers should ensure familiarity with potential side effects and drug interactions and be prepared to manage any complications. For patients without medical contraindications, a regimen of nonsteroidal anti-inflammatory drugs is most helpful for managing both pain and inflammation.
A flat plane stabilization splint is the most frequently prescribed occlusal device for muscle-related TMD. This type of splint has a long track record for effectively managing symptoms when used correctly.18,19 Adjusting and managing stabilization splints may be somewhat tedious, as repeated visits are necessary.
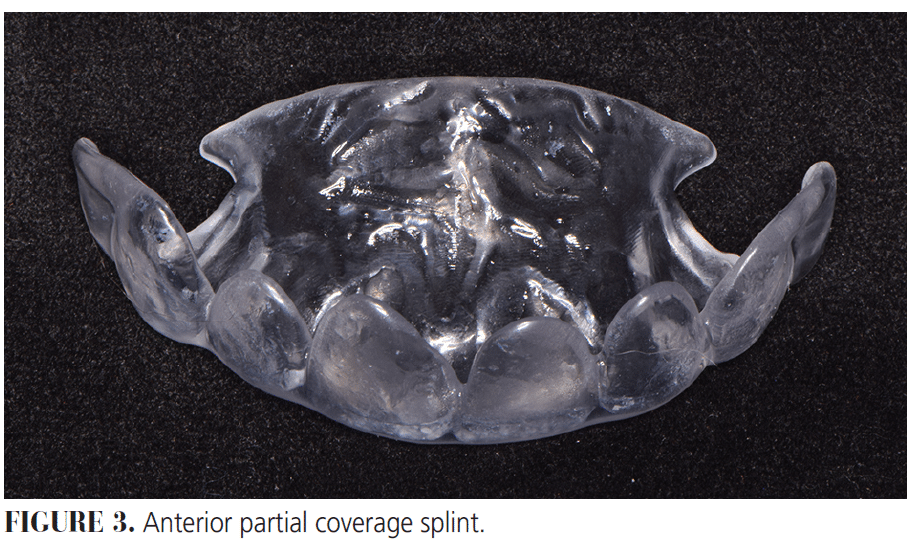
Alternatives for muscle-related TMDs include full or partial coverage anterior bite planes/plates.20,21 These splints do not engage posterior tooth contacts, which may help minimize activation of masticatory muscles. Additionally, partial coverage anterior bite plates achieve deprogramming before restorative treatment (Figure 3).22 Some providers have raised concerns about unmonitored long-term use of occlusal splints, including stabilization splints and anterior bite plates.23-25 Any occlusal appliance used to manage TMD will require follow-up after no more than 2 weeks and careful evaluation of risks/benefits before continuing long-term use. Occasionally, muscle-related TMD issues are associated with collapse or loss of posterior occlusal support, which may require complex oral rehabilitation. Additionally, younger patients with mixed dentition may present with muscle-related TMDs that are often self-limiting and successfully managed with palliative home measures. Occlusal splint therapy is usually not advised in growing and developing patients.
A variety of alternative treatment options have been promoted for muscle-related TMD, such as Botox or steroid injections, trigger point injections, dry needling, and laser therapy. Each has mixed results and its own set of risks and benefits.3 The provider should be appropriately trained and capable of managing undesirable outcomes for any adjunctive therapy prescribed.
If palliative measures, appropriate pharmaceutical use, and occlusal splint therapy do not result in some improvement after 2 weeks, or symptoms begin to worsen, use of the occlusal splint should cease and a specialist should be consulted.
Conclusion
While TMDs are a complex group of orofacial pain conditions, the primary dental provider must identify them early. Proper identification and prompt management of TMDs have significant repercussions on progression of the condition, any restorative dental treatment, and potential comorbid conditions. Through proper screening, including using the leaf gauge to mechanically load the TMJs, the general dentist should feel empowered to conservatively manage common muscle-related TMDs and confidently refer to a specialist when indicated.
References
- Klasser GD, Abt E, Weyant RJ, Greene CS. Temporomandibular disorders: Current status of research, education, policies, and its impact on clinicians in the United States of America. Quintessence Int. 2023;54:328-334.
- Schiffman E, Ohrbach R, Truelove E, et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J Oral Facial Pain Headache. 2014;28:6-27.
- Hoffmann RG, Kotchen JM, Kotchen TA, Cowley TA, Dasgupta M, Cowley AW Jr. Temporomandibular disorders and associated clinical comorbidities. Clin J Pain. 2011;27:268-274.
- Thomas DC, Khan J, Manfredini D, Ailani J. Temporomandibular joint disorder comorbidities. Dent Clin North Am. 2023;67:379-392.
- Ferrillo M, Ammendolia A, Paduano S, et al. Efficacy of rehabilitation on reducing pain in muscle-related temporomandibular disorders: A systematic review and meta-analysis of randomized controlled trials. J Back Musculoskelet Rehabil. 2022;35:921-936.
- Dawson PE. Functional Occlusion from TMJ to Smile Design. St. Louis:Mosby Elsevier; 2007:86-89.
- Lövgren A, Visscher CM, Alstergren P, Lobbezoo F, Häggman-Henrikson B, Wänman A. The outcome of a temporomandibular joint compression test for the diagnosis of arthralgia is confounded by concurrent myalgia. Clin Oral Invest. 2020;24(1):97-102.
- de Wijer A, Lobbezoo-Scholte AM, Steenks MH, Bosman F. Reliability of clinical findings in temporomandibular disorders. J Orofac Pain. 1995;9:181-191.
- Huffman Dental Products. How to Guide for Huffman Leaf Gauge. Available at: prestige-dental.co.uk/app/uploads/2023/04/Huffman-Leaf-Gauge-How-to-Guide.pdf. Accessed February 20, 2026.
- McHorris WH. Non-surgical management of noisy joints. J Tenn Dent Assoc. 1986;66:31-35.
- McHorris WH. Treatment of TMJ dysfunction. J Tenn Dent Assoc. 1980;60:21-23.
- Kato T, Thie NMR, Huynh N, Miyawaki s, Lavigne GJ. Topical review: Sleep bruxism and the role of peripheral sensory influences. J Orofacial Pain. 2003;17:191-213.
- Carra MC, Huynh N, Lavigne G. Sleep bruxism: A comprehensive overview for the dental clinician interested in sleep medicine. Dent Clin N Am. 2012;56:387-413.
- Dubrovsky B, Raphael KG, Lavigne GJ, et al. Polysomnographic investigation of sleep and respiratory parameters in women with temporomandibular pain disorders. J Clin Sleep Med. 2014;10:195-201.
- Gagnon Y, Mayer P, Morisson F, Rompré PH, Lavigne GJ. Aggravation of respiratory disturbances by the use of an occlusal splint in apneic patients: A pilot study. Int J Prosthodont. 2004;17:447-453.
- Metz JE, Attarian HP, Harrison MC, et al. High-resolution pulse oximetry and titration of a mandibular advancement device for obstructive sleep apnea. Front Neurol. 2019;10:757.
- Kuzmanovic Pficer J, Dodic S, Lazic V, Trajkovic G, Milic N, Milicic B. Occlusal stabilization splint for patients with temporomandibular disorders: Meta-analysis of short and long term effects. PLoS One. 2017;12:e0171296.
- Capp N, Eder A. Occlusion and splint therapy. In: Tooth Wear. London: Springer International Publishing; 2022:135-152.
- Fu AS, Mehta NR, Forgione AG, Al-Badawi EA, Zawawi KH. Maxillomandibular relationship in TMD patients before and after short-term flat plane bite plate therapy. Cranio. 2003;21:172-179.
- Seiler A, Lukic N, Özcan M, et al. Temporomandibular joint space variation and masticatory muscle activation during clenching with full versus partial covering occlusal splints. Clin Oral Investig. 2024;28:584.
- The Metz Center Lab Services. Available at: http://themetzcenter.com/lab_services.html. Accessed February 20, 2026.
- Bereznicki T, Barry E, Wilson NHF. Unintended changes to the occlusion following the provision of night guards. Br Dent J. 2018;225:715-722.
- Bereznicki T, Barry E, Wilson NHF. Unintended changes to the occlusion following the provision of night guards. Part two: management. Br Dent J. 2019;226:649-656.
- Magdaleno F, Ginestal E. Side effects of stabilization occlusal splints: a report of three cases and literature review. Cranio. 2010;28:128-135.
From Decisions in Dentistry. February/March 2026;12(1):36-39.

