
Recognize the Early Warning Signs of Autoimmune Disease
Understanding the oral manifestations of the five most common autoimmune diseases equips oral health professionals to identify systemic disease earlier and intervene more effectively.
PURCHASE COURSE
This course was published in the February/March 2026 issue and expires March 2029. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the February/March 2026 issue and expires March 2029. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 010
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe the immunopathology of autoimmune diseases.
- Identify the common oral manifestations associated with rheumatoid arthritis, psoriasis, type 1 diabetes, Graves disease, and Hashimoto thyroiditis.
- Discuss evidence-based management considerations and the role of oral health professionals in early detection, interdisciplinary collaboration, and comprehensive patient care.
Autoimmune (AI) diseases are chronic inflammatory disorders marked by the presence of autoantibodies and dysfunction in both innate and adaptive immunity. This dysfunction results in end-organ damage and clinical disease manifestations.1,2 The innate immune response triggers adaptive immune responses and proliferation of innate immune cells such as macrophages, granulocytes, and dendritic cells. These release inflammatory factors stimulating the infiltration of T and B cells.
The hallmark of AI disease is the presence of autoantibodies that target organ tissue, leading to cytotoxic reactions resulting in tissue damage, and cell death.3 Approximately 15 million people in the United States, or 4.6%, have an AI disease. Of those individuals, 34% have more than one AI disease.2,3 Women are twice as likely as men to be diagnosed with an autoimmune disease, accounting for 63% of cases compared to 37% in men.2,3
Immune system dysfunction is due to proinflammatory environmental agents such as diet, smoking, xenobiotic contacts, infections, obesity, sleep deprivation, stress, and air pollution, as well as family history of AI diseases.2,3 Screening for an AI disease involves an antinuclear antibody (ANA) test. The higher the ANA titers, the greater the probability of developing an AI disease. Due to potential false positives, further antibody testing and clinical evaluation are required.3
The five most common AI diseases in the US are rheumatoid arthritis (RA), psoriasis, type I diabetes, Graves disease (GD), and autoimmune thyroiditis.4 Each AI disease is associated with distinct oral manifestations that may be early indicators of disease onset and progression.
Rheumatoid Arthritis
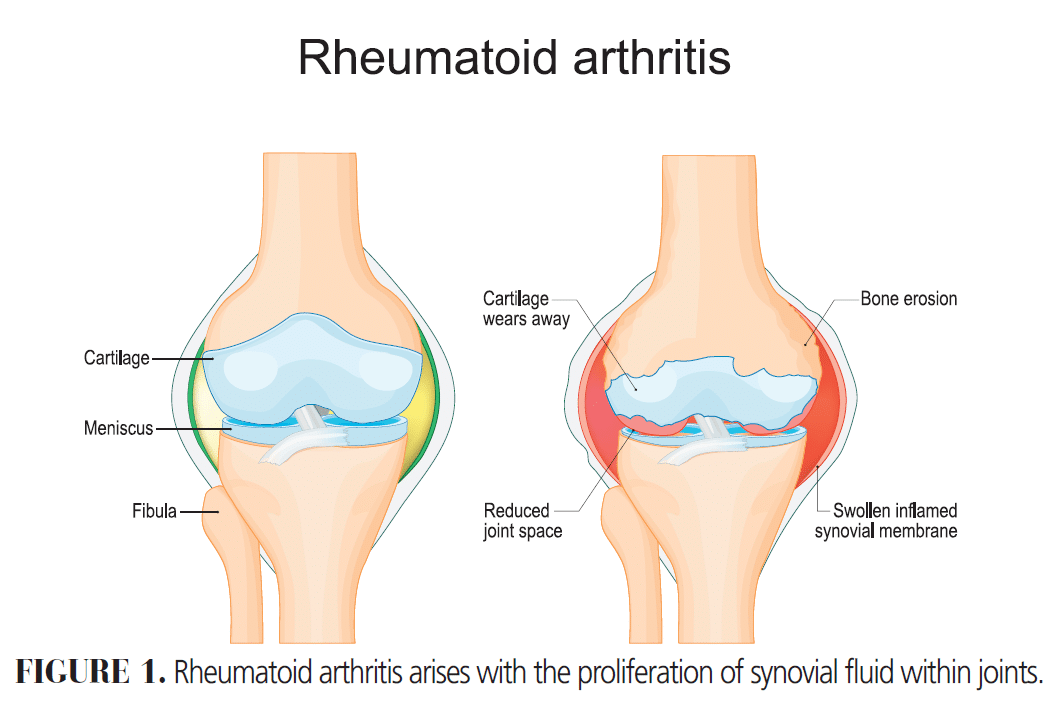
RA is the most common inflammatory arthritis characterized by the proliferation of synovial fluid within joints (Figure 1). The wrists, proximal interphalangeal joints, and meta-carpophalangeal joints are the most frequently affected. Symptoms may last for 6 weeks or more. Risk factors associated with RA are older age with a peak onset between ages 30 and 50, family history of RA, female sex, and smoking. The autoantibodies present in patients with RA include rheumatoid factor and anticitrullinated protein antibody.5
Oral manifestations of RA include periodontitis, xerostomia, secondary Sjögren syndrome, oral candidiasis, and temporomandibular joint disorder. The most common is periodontitis characterized by attachment and bone loss due to a microbial shift from Gram-positive to Gram-negative species such as Porphyromonas gingivalis, P. aggregatibacter, and P. actinomycetemcomitans. This shift causes the release of inflammatory cytokines and metalloproteinases resulting in tissue and bone loss.6 Both RA and periodontitis show an overexpression of pro-inflammatory cytokines such as interleukin (IL) 1-beta, tumor necrosis factor-alpha (TNF)-α, IL-6 and IL-8.7
Xerostomia is the second most common oral manifestation, affecting up to 50% of patients with RA and is often associated with decreased parotid gland function. The symptoms include dryness, burning sensation, difficulty swallowing, and decreased or loss of taste sensation. Xerostomia increases the risk of other oral conditions such as caries, periodontitis, candidiasis, and oral malodor.6 When xerostomia is accompanied with dry eyes it may indicate secondary Sjögren syndrome, which affects 21% of individuals with RA.8 Management strategies for xerostomia and Sjögren syndrome include frequent sipping of water, chewing gum, and using saliva substitutes or salivary stimulants such as pilocarpine or cevimeline.9
Oral candidiasis, an opportunistic fungal infection, is a common sequela in patients with xerostomia. Oral candidiasis is caused by Candida albicans, a fungus present in 30% to 60% of immunocompetent adults. Oral candidiasis is typically asymptomatic and appears as white or erythematous lesions. White lesions are easily removed with gauze, leaving an erythematous mucosal surface. These lesions present most often on the tongue, labial and buccal mucosa, gingival tissues, hard and soft palate, and the oropharynx. The different types of white lesions include pseudomembranous candidiasis, acute atrophic candidiasis, and chronic atrophic candidiasis.
Pseudomembranous candidiasis presents in a third of total cases and is seen mostly in immunocompromised patients using topical steroids. Most commonly seen on the palate, acute atrophic candidiasis is more common among those with uncontrolled diabetes. Chronic atrophic candidiasis, also known as denture stomatitis, occurs under dentures in 65% of cases due to a poor fit, prolonged denture use, and poor oral hygiene.
Oral candidiasis can also present as erythematous lesions including angular cheilitis, median rhomboid glossitis, and linear gingival erythema. Angular cheilitis arises due to a moist environment at the commissures of the mouth. Median rhomboid glossitis is very rare, affecting less than 1% of individuals and presents as an erythematous patch in the center of the tongue due to atrophy of filiform papillae. Atrophy can occur due to smoking or use of inhaled steroids. Linear gingival erythema is seen in patients with human immunodeficiency virus as an erythematous line over the gingival margin of single or multiple teeth. Symptoms include burning sensation, oral bleeding, and changes in taste.
The first line treatment for mild presentations of oral candidiasis is a topical antifungal, with nystatin being the most prescribed. For patients with diabetes, nystatin oral rinse or clotrimazole troches should be avoided due to their high sucrose content. An alternative is triazoles (fluconazole or itraconazole).10
Psoriasis
Psoriasis is a chronic inflammatory skin disease that presents as scaly plaques (Figure 2).11 Up to 3% of the population or 4.5. million people are affected by this disease with symptoms beginning before the age of 40.12,13 There are several types of psoriasis including plaque, inverse, guttate, pustular, erythrodermic, and nail psoriasis. Of these types, plaque psoriasis is the most common and affects up to 80% to 90% of individuals. The most frequently areas affected are the elbows, knees, face, scalp, fingernails and toenails, genitals, lower back, palms, and feet.10

Oral manifestations associated with psoriasis include benign migratory glossitis, fissured tongue, periodontitis, intraoral psoriasis, and chronic atrophic candidiasis. Benign migratory glossitis, also known as geographic tongue, is the most common, affecting approximately 10% of individuals with fissured tongue often accompanying it. If symptomatic, geographic tongue can be treated with oral rinses containing anesthetics, topical corticosteroids, antihistamines, vitamin A, and zinc supplements.14
Both psoriasis and periodontitis share pathophysiologic features including neutrophil and cytokine presence, along with IL-17 and TNF-α.15 Intraoral psoriasis appears as either small, white papules that bleed when scraped or as red and white plaques. The most common locations are the lips, tongue, palate, buccal mucosa and gingiva.13
Type 1 Diabetes
Type 1 diabetes is characterized by an immune-mediated destruction of pancreatic beta cells that leads to insulin deficiency. The disease pathophysiology is composed of three stages: destruction of beta cells, beta cell dysfunction, and symptomatic hyperglycemia.
In the first stage, the beta cells are destroyed but fasting glucose levels are normal and there are no symptoms. In the second stage, more beta cell dysfunction occurs, leading to dysglycemia or an impaired fasting glucose (100 to 125 mg/dL), impaired glucose tolerance, and glycated hemoglobin (HbA1C) of 5.7% to 6.4%. The last stage presents with symptomatic hyperglycemia (≥ 200 mg/dL), fasting glucose (126 mg/dL) and HbA1C ≥ 6.5%. If left untreated, ketoacidosis, a life-threatening condition, occurs causing hyperglycemia, ketonuria, and electrolyte imbalance. The symptoms of ketoacidosis include fruity smelling breath, lethargy, and coma.16
Type 1 diabetes affects about 304,000 children and adolescents and 1.7 million adults or 5% to 10% of the population.16,17 More common among men (0.64%) than women (0.46%), type 1 diabetes causes polyuria or frequent urination, polydipsia or frequent need to drink water, and unintentional weight loss.18 Treatment requires replacement of insulin through daily injections or continuous subcutaneous insulin through an insulin pump.16
The oral manifestations associated with type 1 diabetes include periodontitis, oral mucosal diseases, xerostomia, burning mouth, and taste disturbances.19,20 The function of normal immune cells, including neutrophils, monocytes, and macrophages, are impaired. Neutrophil impairment adherence, chemotaxis, and phagocytosis are dysfunctional, which lead to diminished bacterial killing and an increase in periodontal destruction. Monocytes normally produce TNF-α; however, in those with type 1 diabetes, they produce more TNF-α than normal, resulting in further periodontal destruction.19
The oral mucosal diseases associated with type 1 diabetes include oral lichen planus (OLP), recurrent aphthous stomatitis (RAS), and oral candidiasis.20 The six clinical subtypes of OLP are reticular, papular, plaque, atrophic, erosive, and bullous. Of these subtypes, the most common are reticular, erosive, and plaque.
The reticular type presents as a white lacy network on the buccal mucosa also referred to as Wickham striae. The erosive type presents as erythematous ulcerations while the plaque type appears as white keratotic papules. OLP presents bilaterally and appears most commonly on the buccal mucosa, tongue, and gingiva. The first line treatment is topical corticosteroids in either a gel form, such as triamcinolone acetonide, or a rinse (eg, dexamethasone).21
The three subgroups of RAS are minor aphthous ulcers, major aphthous ulcers, and herpetiform aphthous ulcers. Minor aphthous ulcers are the most common type, accounting for 80% of patients with RAS.22 They present as small round lesions with an erythematous halo covered by a grey-white pseudomembrane. The ulcers are 5 mm or less in diameter and present on nonkeratinized tissue including buccal and labial mucosa and the floor of the mouth.
Major aphthous ulcer type impact about 10% of those with RAS.22 The ulcers are larger in size measuring greater than 10 mm in diameter and last 5 to 10 weeks. These ulcers can present anywhere in the oral cavity and the oropharynx.
Herpetiform aphthous ulcers are the least common, appearing in 1% to 10% of patients with RAS.22 The ulcers are numerous and small, measuring 2 to 3 mm in diameter. They can appear on keratinized and nonkeratinized tissues.22
Xerostomia and burning mouth syndrome are other common oral manifestation of type 1 diabetes. Xerostomia not only contributes to an increased caries risk. but also raises the risk for oral candidiasis. Patients experiencing xerostomia may have a burning sensation or a change in taste.23 In a third of adults with type 1 diabetes, taste dysfunction occurs, inhibiting the ability to maintain a healthy diet, leading to poor glycemic control.20
Thyroid Autoimmune Diseases
The thyroid gland is the largest endocrine gland in the body and is located directly inferior to the larynx. The thyroid is essential for the synthesis and secretion of thyroid hormones and iodine homeostasis.24 The thyroid produces hormones that are 90% inactive thyroxine (T4) and 10% active triiodothyronine (T3). T4 is a prohormone of T3 and is converted peripherally in the liver, kidneys, and brain.25
The thyroid also houses the parathyroid gland, which releases calcitonin, an essential hormone for bone health. When functioning normally, the hypothalamus releases thyrotropin, releasing hormone (TRH), which stimulates the pituitary gland to release thyroid stimulating hormone (TSH). TSH stimulates the thyroid to release T3 and T4.24 When T3 and T4 levels increase, the release of TRH and TSH decreases through a negative feedback loop. This, in turn, decreases T3 and T4 secretion and iodine uptake.25 These thyroid hormones play an important role in body temperature regulation, heart rate, digestive rate, muscle contraction, and metabolism.24 When the thyroid is functioning incorrectly, diseases such as Graves disease (GD) and Hashimoto thyroiditis (HT) can arise.
Graves Disease
GD is defined as an overactivity of the thyroid gland also known as hyperthyroidism.26 The disease is caused by thyroid-stimulating immunoglobulin (TSI) also known as thyroid stimulating antibody (TSAb). TSI binds to the TSH receptor on the thyroid cell membrane, leading to thyroid hormone synthesis T3 and T4 and thyroid gland growth. As a result, TSH is low and T3 and T4 levels are elevated.27
GD affects one in 100 Americans and is more commonly seen in women over the age of 30. A family history of GD, HT, or other autoimmune disorders such as vitiligo, autoimmune gastritis, TID, and RA, increase the likelihood of a GD diagnosis. Symptoms include weight loss, rapid and irregular heartbeat, nervousness, irritability, insomnia, muscle weakness, sweating, goiter, and ophthalmopathy.26
The most common oral manifestations associated with hyperthyroidism are increased caries risk, periodontitis, enlargement of extraglandular thyroid tissue seen on the lateral posterior tongue, maxillary or mandibular osteoporosis, accelerated tooth eruption, and burning mouth syndrome.28
Autoimmune Thyroiditis
Autoimmune thyroiditis, or HT, is an underactivity of the thyroid gland or hypothyroidism (Figure 3).29 The disease is caused by the formation of antithyroid antibodies, thyroid peroxidase, thyroglobulin, and T-cell activation that attack the thyroid tissue, causing progressive fibrosis.30,31 As a result, TSH is elevated and T3 and T4 are low.31
HT is four to 10 times more common in women than in men. While the disease can manifest in teens and young women, it is mostly seen between the ages of 30 and 50. Individuals are more likely to develop the disease if other autoimmune diseases are present such as celiac disease, lupus, Sjögren syndrome, RA, and type 1 diabetes. Symptoms include fatigue, weight gain, cold intolerance, joint and muscle pain, constipation, dry skin, irregular menstrual periods, and slow heart rate. Individuals with HT are treated with levothyroxine sodium.29
The most common oral manifestations associated with hypothyroidism are macroglossia or enlarged tongue, dysgeusia or altered taste sensation, periodontitis, delayed tooth eruption, altered tooth morphology, and delayed wound healing.28 Patients with HT are likely to develop cardiovascular and metabolic disorders, which are associated with poor periodontal health.
The commonality between HT and periodontal diseases is the presence of inflammation and T helper cells, Th1 and Th17. HT also presents with vascular endothelial dysfunction, which impairs blood flow and nutrient delivery to the periodontal tissues. Patients with HT may have decreased bone density, exacerbating bone loss seen with periodontitis.31
Conclusion
With the rise in prevalence of autoimmune diseases in the US, oral health professionals must be able to accurately identify, understand, and treat the most common oral pathologies associated with the top five AI diseases. By recognizing the oral manifestations early, oral health professionals play a vital role in ensuring accurate diagnosis, timely intervention, and improved patient outcomes through comprehensive care.
References
- Abajina M, Abend, AH, Avasarala J, et al. Estimation of prevalence of autoimmune diseases in the United States using electronic health record data. J Clin Invest. 2025;135:e178722.
- Miller FW. The increasing prevalence of autoimmunity and autoimmune diseases: an urgent call to action for improved understanding, diagnosis, treatment, and prevention. Curr Opin Immunol. 2022;80:102266.
- Jiang D, Shi J, Su Q, Xiang Y, Zhang M. The role of inflammation in autoimmune disease: a therapeutic target. Front Immunol. 2023;14:1267091.
- De Widt L. New study calculates autoimmune disease prevalence in U.S. Available at /newsnetwork.mayoclinic.org/discussion/new-study-calculates-autoimmune-disease-prevalence-in-u-s/. Accessed February 13, 2026.
- Wasserman AM. Diagnosis and management of rheumatoid arthritis. Am Fam Physician. 2011;84:1246-1252.
- Abubakr OA, Hamdy MA, Mohamed MA, Youssef AM. Dental and oral manifestations of rheumatoid arthritis: is it related to general disease activity? J Med Sci Res. 2023;6:15-24.
- Cugno M, Gualtierotti R, Marzano AV, Spadari F. Main oral manifestations in immune-mediated and inflammatory rheumatic diseases. J Clin Med. 2019:8;21.
- Sjögren’s Foundation. Overlapping diseases. Available at sjogrens.org/living-with-sjogrens/overlapping-diseases#:~:text=Graves%20disease%20and%20Hashimoto%20thyroiditis,Autoimmune%20Thyroid%20Disease%20and%20Sjögren’s. Accessed February 13, 2026.
- Blum MA, Carsons SE. Sjögren syndrome. Available at ncbi.nlm.nih.gov/books/NBK431049/. Accessed February 14, 2026.
- Brizuela M, Raja A, Taylor M. Oral Candidiasis.Treasure Island, Florida: StatPearls. 2025.
- Cleveland Clinic. Psoriasis. Available at my.clevelandclinic.org/health/diseases/6866-psoriasis. Accessed Febuary 13, 2026.
- Adamska K, Adamski Z, Dorocka-Bobkowska B, Olejnik M. Oral health status of psoriatic patients managed with modern biological therapy. Postepy Dermatol Alergol. 2021;39:1151-1156.
- Brown GC, Dreyer LN. Oral manifestations of psoriasis clinical presentation and management. N Y State Dent J. 2012;78:14-18.
- Carla V, Carlos A, Carneiro S. Geographic tongue and psoriasis: clinical, histopathological, immunohistochemical and genetic correlation – a literature review. An Bras Dermatol. 2016;91:410-421.
- Farag YMK, Hussein M, Sonis S. Psoriasis and oral health in adult United States population: a cross-sectional study. BMC Oral Health. 2023;23:66.
- Lucier J, Mathias PM. Type 1 diabetes. Available at ncbi.nlm.nih.gov/books/NBK507713. Accessed February 13, 2026.
- American Diabetes Association. Statistics About Diabetes. Available at diabetes.org/about-diabetes/statistics/about-diabetes. Accessed February 13, 2026.
- United States Centers for Disease Control and Prevention. Prevalence of diagnosed diabetes in adults by diabetes type – United States, 2016. Available at cdc.gov/mmwr/volumes/67/wr/mm6712a2.htm#:~:text=The%20prevalence%20of%20type%201%20diabetes%20was%20higher%20among%20men,%25)%20(p%3C0.01). Accessed February 13, 2026.
- Indurkar MS, Indurkar S, Maurya AS. Oral manifestations of diabetes. Clin Diabetes. 2016;34:54-57.
- Vernillo AT. Dental considerations for the treatment of patients with diabetes mellitus. J Am Dent Assoc. 2003;134:24-33.
- Raj G, Raj M. Oral lichen planus. Available at ncbi.nlm.nih.gov/books/NBK578201. Accessed February 13, 2026.
- Chatterjee K, Plewa MC. Recurrent apthous stomatitis. Available at ncbi.nlm.nih.gov/books/NBK431059/. Accessed February 13, 2026.
- Rohani B. Oral manifestations in patients with diabetes mellitus. World J Diabetes. 2019;10:485-489.
- Achanta A, Kasbage SD. Oral manifestations of thyroid disorders. J Res Med Dent Sci. 2022;10:12-16.
- Armstrong M, Asuka E, Fingeret A. Physiology, thyroid function. Available at ncbi.nlm.nih.gov/books/NBK537039/. Accessed February 13, 2026.
- National Institute of Diabetes and Digestive and Kidney Diseases. Graves’ Disease. Available at niddk.nih.gov/health-information/endocrine-diseases/graves-disease. Accessed February 13, 2026.
- Bhusal K, Pockhrel B. Graves’ Disease. Available at ncbi.nlm.nih.gov/books/NBK448195/. Accessed February 13, 2026.
- Bathla M, Chandna S. Oral manifestations of thyroid disorders and its management. Indian J Endocrinol Metab. 2011;15:S113-S116.
- National Institute of Diabetes and Digestive and Kidney Diseases. Hashimoto’s Disease. Available at niddk.nih.gov/health-information/endocrine-diseases/hashimotos-disease. Accessed February 13, 2026.
- Kaura J, Jialal I. Hashimoto thyroiditis. Available at ncbi.nlm.nih.gov/books/NBK459262/. Accessed February 13, 2026.
- Morais A, Resende M, Pereira J. Association between hashimoto’s thyroiditis and periodontal disease: a narrative review. Acta Med Port. 2016;29:651-657.
From Decisions in Dentistry. February/March 2026;12(1):28-31.

