

Digital Precision Transforms Full-Arch Implant Surgery and Immediate Loading Success
Advanced digital workflows paired now allow clinicians to plan bone reduction, implant placement, and prosthetic design with unprecedented accuracy. By integrating immediate loading protocols and durable interim prostheses, these technologies streamline treatment, reduce complications, and greatly enhance patient outcomes.
Based on the restorative volume, prosthetic type, and implant positions, the necessity for bone reduction can be determined during the virtual implant planning phase. The required amount of bone reduction can be precisely evaluated during virtual implant planning, ensuring optimal implant positioning and prosthetic outcomes.1,2
There are three primary approaches for guided surgery: static computer-aided implant surgery (s-CAIS), dynamic computer-aided implant surgery (d-CAIS), and robot-assisted implant placement.3,4 Choosing among these techniques depends on clinical preferences, workflow integration, and case-specific requirements; though s-CAIS is predominantly used in a clinic. Regardless of the selected method, guided and robotic-assisted implant surgeries contribute to improved implant placement accuracy, reduced surgical invasiveness, and enhanced long-term treatment outcomes.5
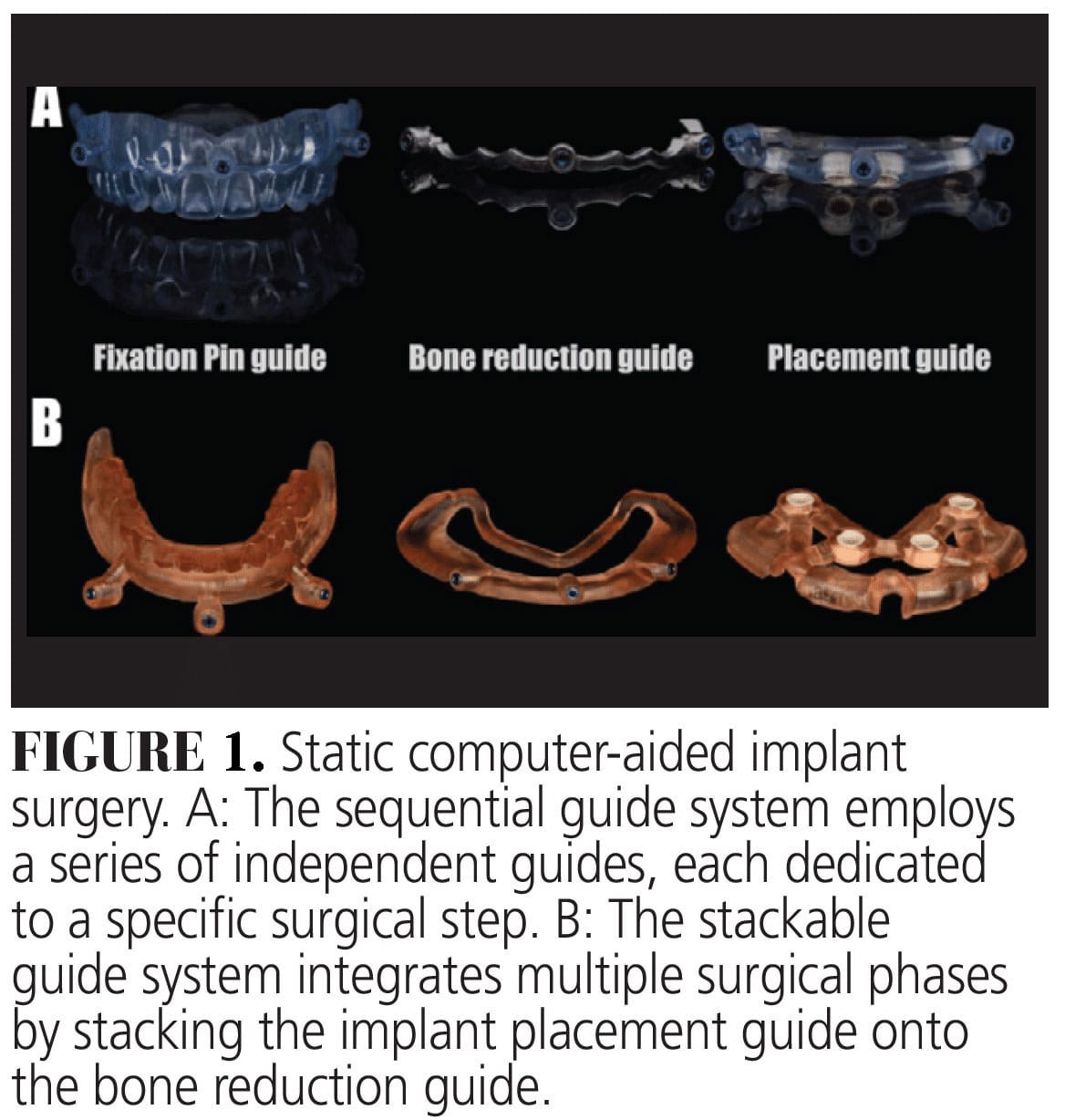
In s-CAIS, two primary guided systems are utilized: the sequential guide system and the stackable guide system (Figure 1). The sequential guide system employs a series of independent guides, each dedicated to a specific surgical step, including fixation pin placement, bone reduction, and implant placement. In contrast, the stackable guide system integrates multiple surgical phases by stacking the implant placement guide onto the bone reduction guide, creating a streamlined workflow that eliminates the need for repeated guide replacements. Both guided systems effectively translate digital preoperative planning into clinical execution, with the choice between them being dependent on case-specific requirements, surgical complexity, and clinician preference.
Material selection for each guide in s-CAIS plays a crucial role in ensuring surgical precision, durability, and procedural efficiency. The two predominant materials used for guide fabrication are printing resin and cobalt-chromium, each offering distinct advantages and considerations. Printing resin is the most used material due to its cost-effectiveness and ease of fabrication. However, to ensure sufficient strength and durability during the surgical procedure, a specific minimum material thickness is required to prevent fractures or deformations that could compromise guide stability. In contrast, cobalt-chromium guides, although more expensive, allow for a thinner design, which improves surgical accessibility and facilitates a less obstructive intraoperative workflow. Material selection also directly influences critical parameters, such as offset values in guide design and fabrication. Failure to account for these material-specific considerations may lead to technical complications.
Lastly, since various loading protocols for ISCFDPs have consistently demonstrated high implant survival rates,6,7 immediate loading with interim ISCFDPs has become an increasingly preferred approach for edentulous patients receiving at least four implants.8-11 The success of immediate loading is contingent on optimal primary implant stability, proper implant distribution, and strategic prosthetic planning, all of which must be carefully considered during the surgical planning phase. By incorporating immediate loading strategies into the surgical plan, clinicians can enhance efficiency, reduce treatment time, and improve patient satisfaction while maintaining long-term prosthetic and implant success.
The quality of the immediate loading prosthesis is a critical factor in fully utilizing the digital workflow during the prosthetic phase of treatment.12 A well-designed interim ISCFDP not only facilitates a smooth transition to the definitive prosthesis but also ensures optimal function, stability, and patient comfort throughout the healing phase. Durability is a key consideration for immediate loading devices, as they must withstand functional loads during osseointegration while maintaining structural integrity. To enhance both ease of fabrication and durability, various prosthetic conversion techniques have been developed, allowing for a more efficient and predictable workflow.
The integration of digital workflows in full-arch implant rehabilitation has significantly enhanced precision, efficiency, and predictability throughout the treatment process. A prosthetically driven approach, beginning with comprehensive diagnostic data collection and meticulous planning, ensures that implant positioning is optimized to meet both functional and esthetic demands. Advanced digital tools, including IOS, CBCT, digital wax-ups, and guided implant surgery, facilitate seamless communication between the surgical and prosthetic teams, minimizing errors and improving overall treatment outcomes. Furthermore, the use of s-CAIS, d-CAIS, and robot-assisted guided surgery has enabled clinicians to accurately transfer digital planning to the clinical setting, reducing intraoperative complications and enhancing surgical precision.
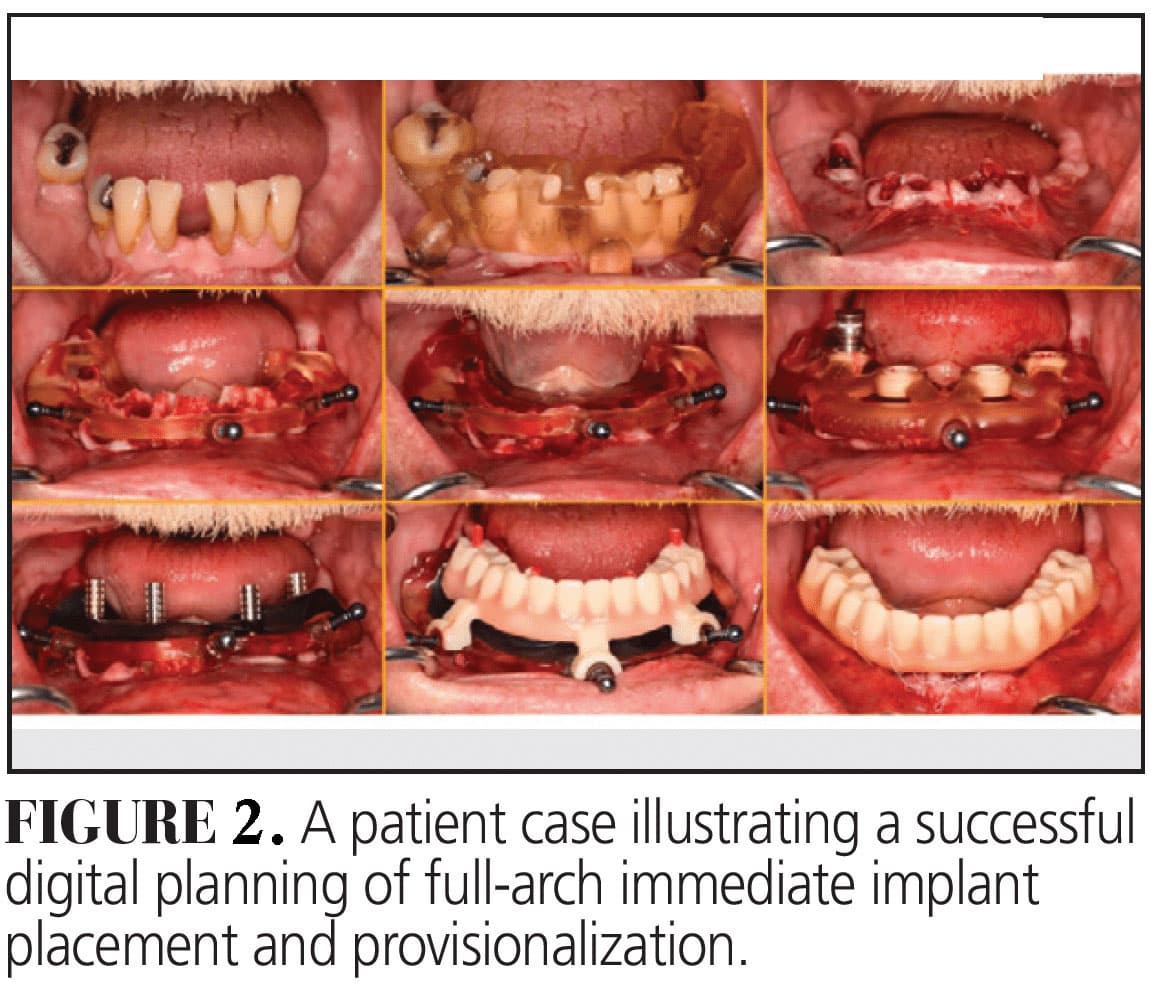
The selection of prosthetic materials, abutments, and restorative space parameters plays a critical role in ensuring long-term prosthetic stability and patient satisfaction. Additionally, the immediate loading protocol has emerged as a preferred treatment modality, offering shorter treatment times and improved patient experience while maintaining high implant survival rates. Ultimately, the successful rehabilitation of implant-supported and implant-assisted complete-arch prostheses relies on a comprehensive digital workflow, integrating diagnostic assessment, surgical precision, and prosthetic planning to achieve optimal long-term outcomes (Figure 2).
References
- Bidra AS. Technique for systematic bone reduction for fixed implant-supported prosthesis in the edentulous maxilla. J Prosthet Dent. 2015;113:520-523.
- Zhao W, Teng W, Su Y, Zhou L. Accuracy of dental implant surgery with freehand, static computer-aided, dynamic computer-aided, and robotic computer-aided implant systems: An in vitro study. J Prosthet Dent. 2024:S0022-3913:00702-9.
- Takács A, Hardi E, Cavalcante BGN, Szabó B, Kispélyi B, Joób-Fancsaly Á, Mikulás K, Varga G, Hegyi P, Kivovics M. Advancing accuracy in guided implant placement: A comprehensive meta-analysis: Meta-Analysis evaluation of the accuracy of available implant placement Methods. J Dent. 2023;139:104748.
- J Yang J, Li H. Accuracy assessment of robot-assisted implant surgery in dentistry: A systematic review and meta-analysis. J Prosthet Dent. 2024;132:747.
- Aghaloo T, Hadaya D, Schoenbaum TR, Pratt L, Favagehi M. Guided and navigation implant surgery: a systematic review. Int J Oral Maxillofac Implants. 2023;38(suppl):7-15.
- Papaspyridakos P, Chen CJ, Chuang SK, Weber HP. Implant loading protocols for edentulous patients with fixed prostheses: a systematic review and meta-analysis. Int J Oral Maxillofac Implants. 2014;29(Suppl):256-270.
- Gallardo YNR, da Silva-Olivio IR, Gonzaga L, Sesma N, Martin W. A systematic review of clinical outcomes on patients rehabilitated with complete-arch fixed implant-supported prostheses according to the time of loading. J Prosthodont. 2019;28:958-968.
- Schimmel M, Araujo M, Abou-Ayash S, et al. Group 4 ITI Consensus Report: Patient benefits following implant treatment in partially and fully edentulous patients. Clin Oral Implants Res. 2023;34(Suppl 26):257-265.
- Horiuchi K, Uchida H, Yamamoto K, Sugimura M. Immediate loading of Brånemark system implants following placement in edentulous patients: a clinical report. Int J Oral Maxillofac Implants. 2000;15:824-830.
- Grunder U. Immediate functional loading of immediate implants in edentulous arches: two-year results. Int J Periodontics Restorative Dent. 2001;21:545-551.
- Misch CM. Immediate loading of definitive implants in the edentulous mandible using a fixed provisional prosthesis: The denture conversion technique. J Oral Maxillofac Surg. 2004;62(9 Suppl 2):106-115.
- Nagai T, Liu W, Yang CC, Polido WD, Morton D, Lin WS. Intraoral scanning for implant-supported complete-arch fixed dental prostheses (ISCFDPs): Four clinical reports. J Prosthodont. 2024 Nov 3.
This originally appeared in Nagai T, AlQallaf H. Precision planning in full-arch implant rehabilitation. Decisions in Dentistry. 2025;11(4):32-35.
