
Rescuing a Smile With a Ridge Augmentation and Implant Rehabilitation
Severe trauma left a patient missing central incisors and facing a complex horizontal and vertical ridge defect. Through precision-guided bone regeneration and staged implant placement, both form and function were restored with results still holding strong 4 years later.
Dental implant placement in the esthetic zone presents unique challenges, especially when compounded by trauma-induced hard and soft tissue loss. This case highlights the strategic use of guided bone regeneration (GBR) and growth factors to overcome a severe combined ridge defect and achieve long-term stability and esthetic success.
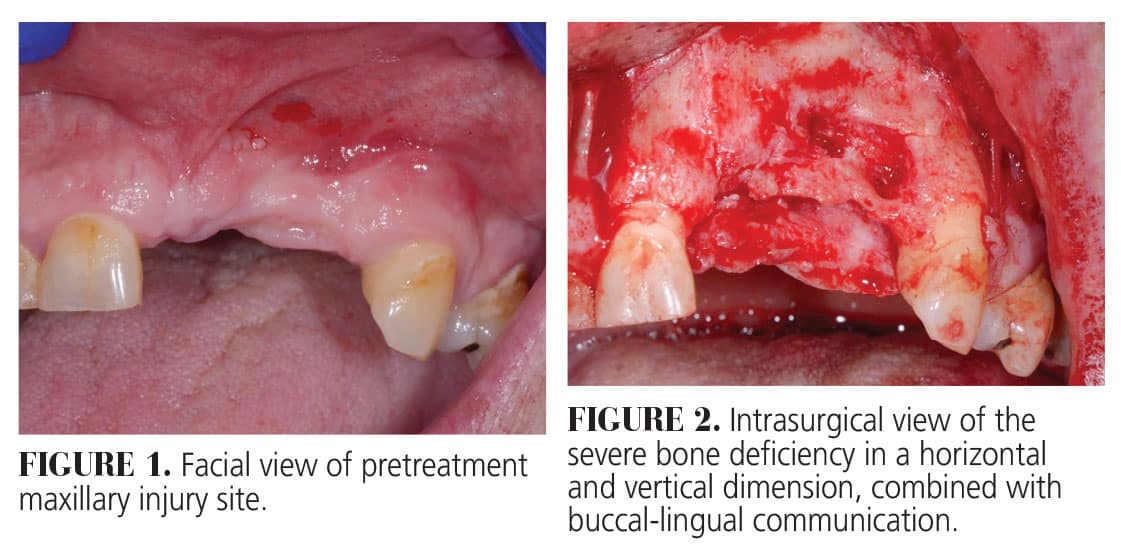
The residual defect was classified as a severe combined horizontal and vertical ridge defect. A through-and-through defect was detected in the left area of the premaxilla (Figure 2). Favorably, the alveolar bone observed on the adjacent natural teeth #8 and11 was intact. Following degranulation, cortical perforations were made to stimulate angiogenesis. A resorbable collagen membrane was trimmed and stabilized on the facial with titanium microscrews, allowing the composite bone graft to be condensed until an ideal geometric form was achieved (Figure 3).
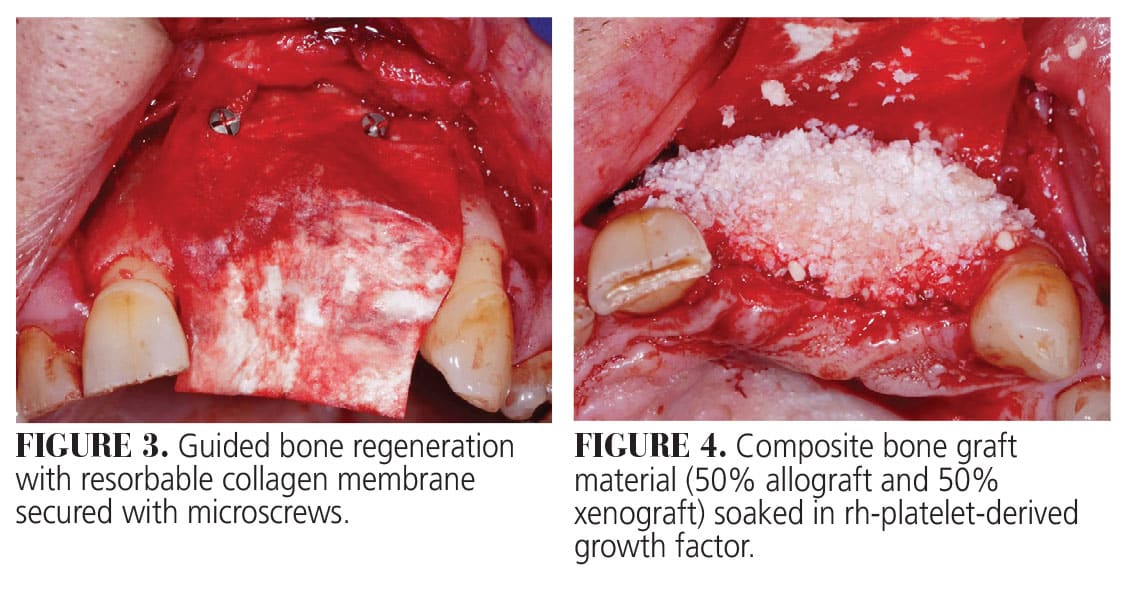
The construct was a composite bone graft consisting of 50% mineralized freeze-dried bone allograft and 50% inorganic bovine bone hydrated for 15 minutes with rhPDGF-BB. Another layer of construct was placed over the composite graft to provide further volume stability (Figure 4). The collagen membrane was then rotated to the palate, extending apically beyond the extent of the defect, and stabilized on the lingual using an additional screw (Figure 5). The flap was released through full/split dissection to ensure tension free primary wound closure using multiple single interrupted and horizontal mattress 5-0 polypropylene sutures (Figure 6).
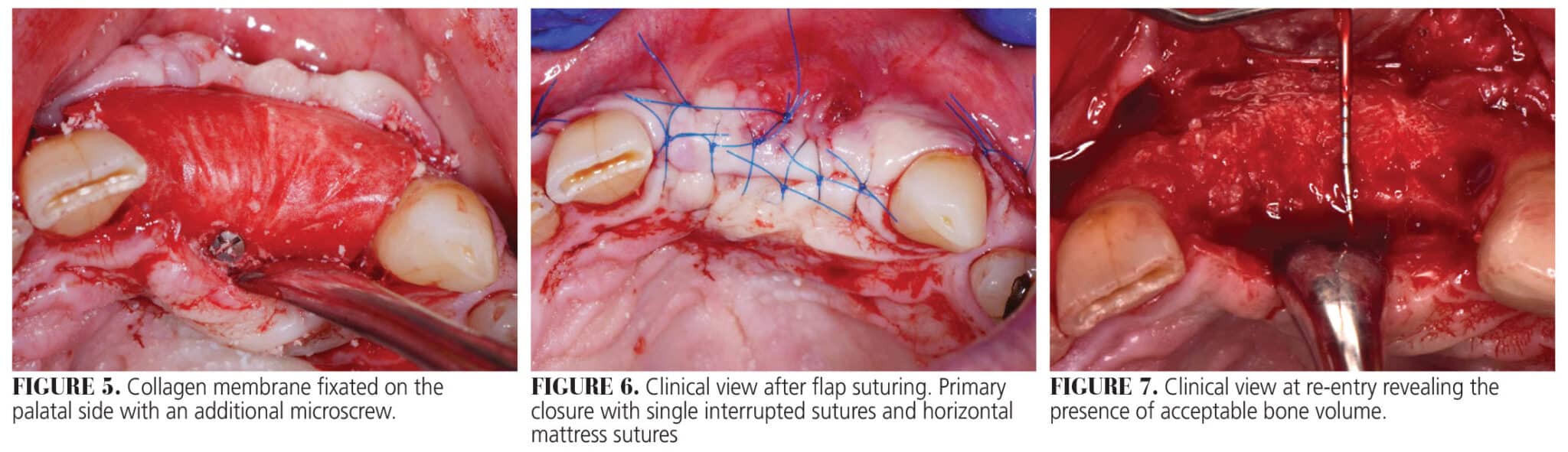
The flap was sutured in two layers. First, a horizonal mattress suture was placed 4 mm from the incision line; second, single interrupted sutures were placed to close the edges of the flap leaving at least 4 mm of the connective tissue layer between the membrane and the oral epithelium. This double layer suture technique approximates the connective tissue of the lingual and buccal flaps, providing a barrier preventing flap exposure. The vertical releasing incisions were closed with single interrupted sutures.
The instructions given prior to the procedure were reviewed again, both verbally and in writing. Post-operative antibiotics consisted of amoxicillin 500 mg q8h × 10 days, bimodal dosing of ibuprofen 600 mg + acetaminophen 650 mg q6h prn and bid rinsing with 0.12% chlorhexidine digluconate. Post-operative follow-up occurred at 3, 8, and 16 weeks and at 6 months. Throughout the duration of healing, the patient reported minimal discomfort and no complications were reported or observed.
Implant surgery was performed at 6 months after the ridge augmentation procedure. Flap reflection revealed outstanding three-dimensional bone gain in a vertical and horizontal direction (Figure 7). The bone was revascularized with excellent bleeding. Implant placement was performed according to the manufacturer instructions. Two tapered 3.8 × 10 mm implants were placed in a two-stage fashion in the position of teeth #9 and 10 (Figure 8). A further horizontal and vertical bone augmentation was performed around the dental implants using the same composite graft soaked in rh-PDGF. The construct was applied to a vertical peri-implant bone defect and covered with a collagen membrane (Figure 9). Primary closure was obtained with single interrupted 5-0 polypropylene sutures.
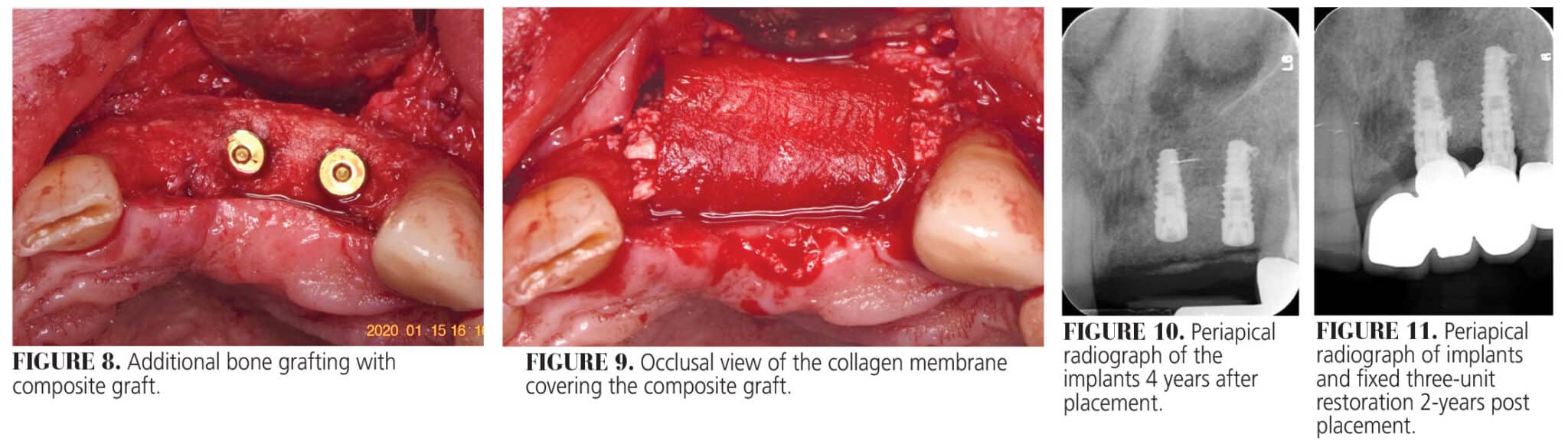
A post-operative radiograph was taken to confirm implant positioning two dimensionally (Figure 10). Two of the fixation tacks placed at the GBR surgery were left submerged as they were covered with osseous tissue, and their maintenance did not influence implant placement.
Exposure of the implants was performed after 3 months to place healing abutments. Bone augmentation procedures often result in coronal shift of the mucogingival junction (MGJ). Therefore, the exposure procedure started with a horizontal incision between the adjacent teeth (#8 and 11), 1 to 2 mm lingual from the previous horizontal midcrestal incision.
The location of the palatal incision depends on the amount of keratinized tissue present on the buccal side. The flap was elevated in a full split thickness to reposition the MGJ apically to its original position prior to the bone augmentation procedure. Furthermore, this buccally repositioned flap allows for the 3 to 4 mm of keratinized tissue to be buccally displaced avoiding the need for a second surgery to increase the amount of keratinized tissue. The cover screws were replaced with tall healing abutments.
Final restoration was completed 5 months later. Figure 11 depicts the patient 4 years after placement of the final restoration indicating minimal remodeling of the augmented site. The patient reported no adverse events since the procedure was completed. This case demonstrates that even the most severe anterior ridge defects can be predictably managed with advanced regenerative techniques, meticulous surgical planning, and careful soft tissue handling. Four years post-restoration, the patient continues to enjoy stable function and a confident smile.
This originally appeared in Boeriu S, Hottel TL, Chirla C, Chirla P. Achieving predictable bone regeneration without autogenous grafts. Decisions in Dentistry. 2025;11(2):36-39.
