
Preventing Infective Endocarditis
Understanding when to prescribe antibiotic prophylaxis, and why oral hygiene may matter more, can help dental professionals prevent a potentially fatal cardiac infection.
PURCHASE COURSE
This course was published in the May/June 2025 issue and expires June 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the May/June 2025 issue and expires June 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 750
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Explain the pathophysiology, risk factors, and clinical manifestations of infective endocarditis.
- Identify the current American Heart Association and European Society of Cardiology guidelines for antibiotic prophylaxis related to dental procedures.
- Describe the role of oral health maintenance in reducing the risk of infective endocarditis, especially in high-risk patients.
Infective endocarditis (IE) is a rare, often fatal, inflammatory condition of the endocardium, the innermost lining of the heart. It can progress quickly with a mortality rate of around 30% in the first year.1,2 The virulent microbiota that contribute to this process can enter the blood stream during certain dental procedures, among other avenues.3 Antibiotic prophylaxis (AP) prior to any dental treatment involving gingival or tissue manipulation has been thought to mitigate these concerns.3-7
Historically, AP was recommended for any patient at risk for IE; however, due to insufficient evidence, in 2007 the AP protocol was revised by the American Heart Association (AHA) and the European Society of Cardiology (ESC). Since then, AP for the prevention of IE has been limited to high-risk patients.3,8 In 2021, the AHA and, later in 2023, the ESC only recommended AP for patients at high-risk for developing IE. These patients include those with a high likelihood of severe adverse outcomes should they develop IE such as those with prosthetic valves, any foreign material used for cardiac valve repair, previous IE, congenital heart disease or defect, or coronary heart disease. Oral disease is recognized as a major contributor to IE. Proper oral hygiene including regular maintenance provides positive outcomes in the prevention of IE.
Risk Factors and Types
Risk factors associated with IE are divided into cardiac and noncardiac categories. Cardiac risk factors include prosthetic valves, congenital heart defects, rheumatic heart disease, mitral valve prolapse, aortic valve stenosis and the presence of an implantable electronic cardiac device. Noncardiac risk factors include diabetes mellitus, hemodialysis, intravenous (IV) drug use, immunosuppression, and poor oral hygiene.9 Other risk factors include advanced age (> 60), male gender, history of prior IE, poor dentition, and dental procedures that involve soft tissue trauma, surgery, and the root apex.10
IE has two types: acute endocarditis and subacute endocarditis. Acute endocarditis is a febrile illness that rapidly damages the endocardium and lining of the heart, while spreading hematogenously.11 Due to its presence in the bloodstream, IE can involve almost any organ system in the body.2 It can be fatal within weeks. Staphylococcus aureus is commonly associated with this condition and is often passed from IV drug users.12-16
Subacute endocarditis is a slower inflammatory condition that is complicated by a major embolic event or ruptured structure.10 It is caused by the less virulent viridans streptococci. Its progression is more gradual. S. viridans affects the left side of the heart and the aortic and mitral valves; it occurs in damaged, diseased, and abnormal heart valves.17
Impact of Oral Health
Oral pathogens are one of the most significant risk factors for IE.18 The oral cavity harbors more than 700 different species of bacteria, including commensal and opportunistic pathogens.19-21 These oral conditions are a frequent source of bacteremia, such as the viridians group streptococci (VGS), HACEK group, and orange and red complex bacteria.22,23 A notable 30% to 40% of suggesting a connection between invasive dental work and the onset of IE.24
The bacteria present in the oral cavity enter the blood stream through traumatic tissue injury such as chewing food, toothbrushing, or during periodontal diagnostic charting and treatment.3 Poor periodontal health appears to increase the risk of cardiovascular and pulmonary diseases, preterm birth, and low birth weight.25 In periodontal patients, the ulcerated pocket epithelium provides vascular entry for pathogens to the systemic circulation and plausible etiology of IE and cardiovascular disease.25,26
Indirect evidence suggests that the host immune response is also increased due to the systemic inflammatory burden caused by the influx in pro-inflammatory cytokines. A cross-sectional study found that patients with valvular heart disease and IE had a significantly higher percentage of alveolar bone loss compared to those without IE.27 A related study reported a significant correlation between the occurrence of IE and clinical oral findings. They found that decayed teeth and periodontitis were the leading predisposing factors. VGS were isolated in 52% of cases, whereas staphylococci were isolated in 32% of cases.28
Current literature also suggests that maintaining good oral hygiene in patients at risk from VGS-induced IE can prevent bacteremia from routine daily activities such as chewing food or toothbrushing.5,29 Because routine activities result in transient bacteremia at a much higher frequency than a single dental procedure, optimizing good oral health supports the prevention of IE.5 While a pathogenic link appears plausible, difficulties arise due to the diverse microbiota present in IE lesions, which can originate from various conditions, including oral infections, in addition to periodontitis.23
Clinical Recommendations
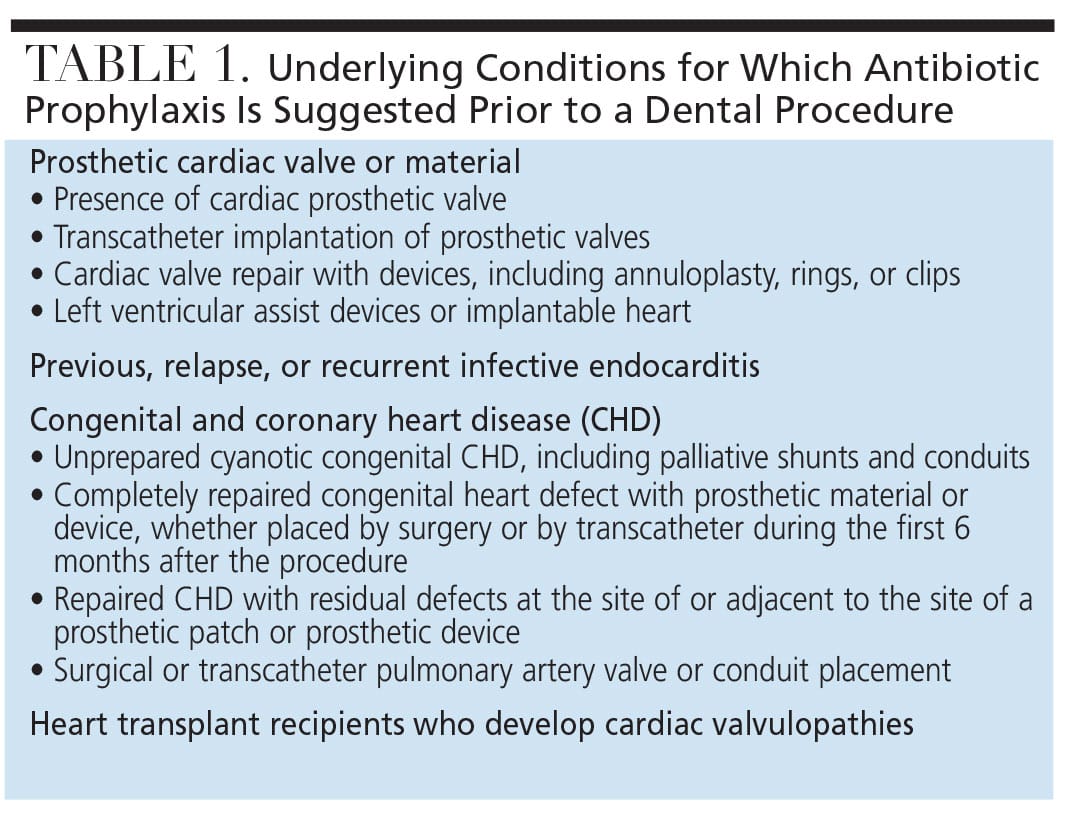
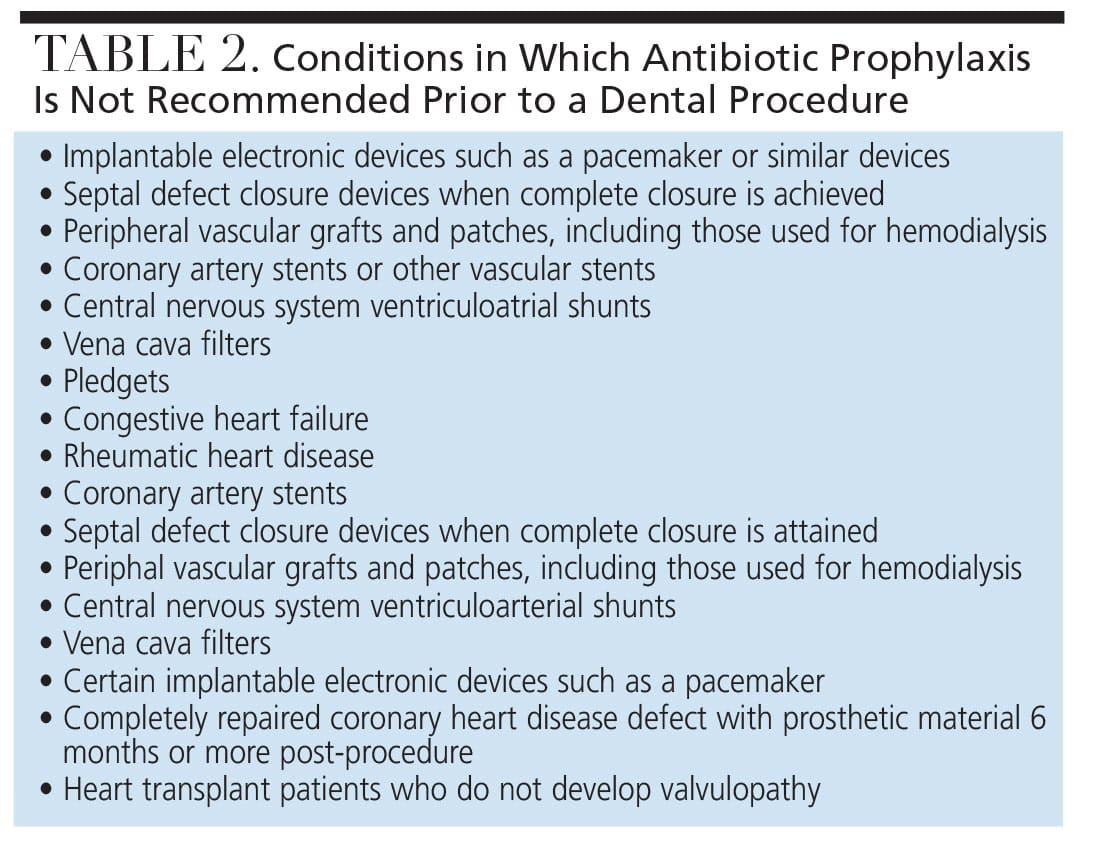
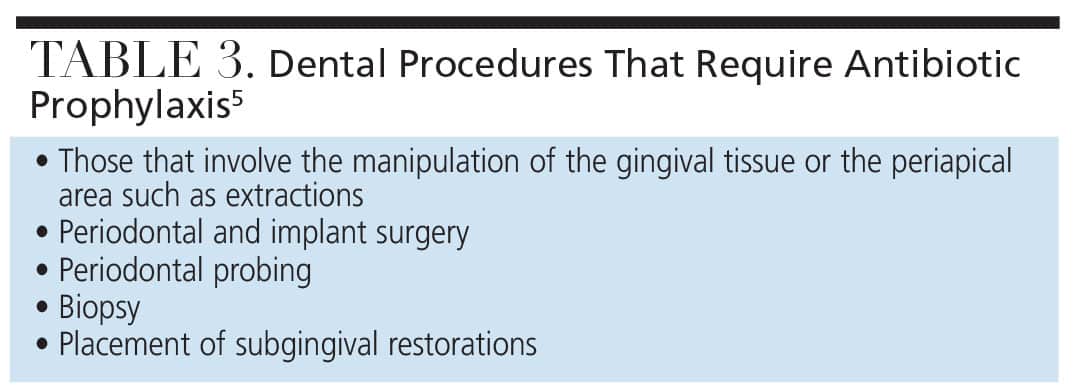
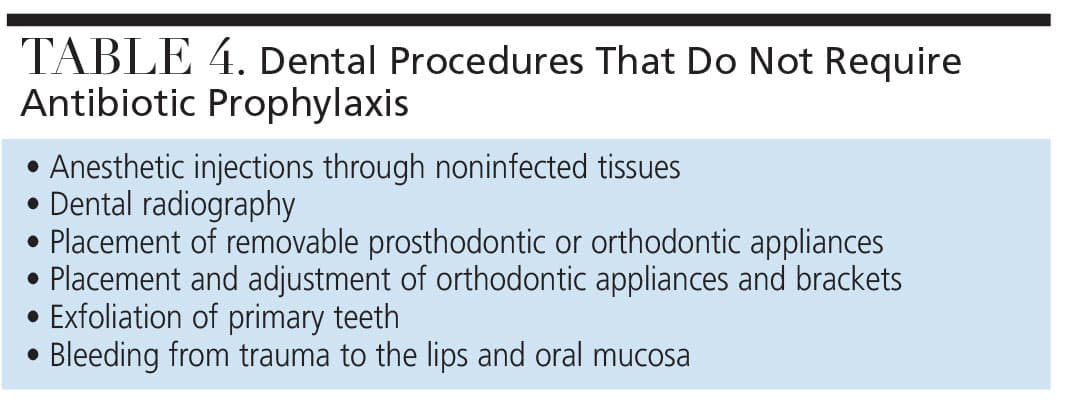
In 2007, the AHA published updated, evidence-based guidelines on the recommend use of AP to prevent VGS-IE in patients undergoing invasive surgical procedures. In 2021, the guidelines were revised to reaffirm the classification of high-risk VGS groups established in the earlier 2007 guidelines. Overall, these updates reflect a continued emphasis on preventive measures for vulnerable patients to reduce the risk of IE associated with dental and surgical procedures (Tables 1 and 2). According to the AHA and the ESC, AP is recommended only in high-risk cases that undergo invasive dental procedures.5,30 Tables 3 and 4 list the dental procedures that do and do not require AP.
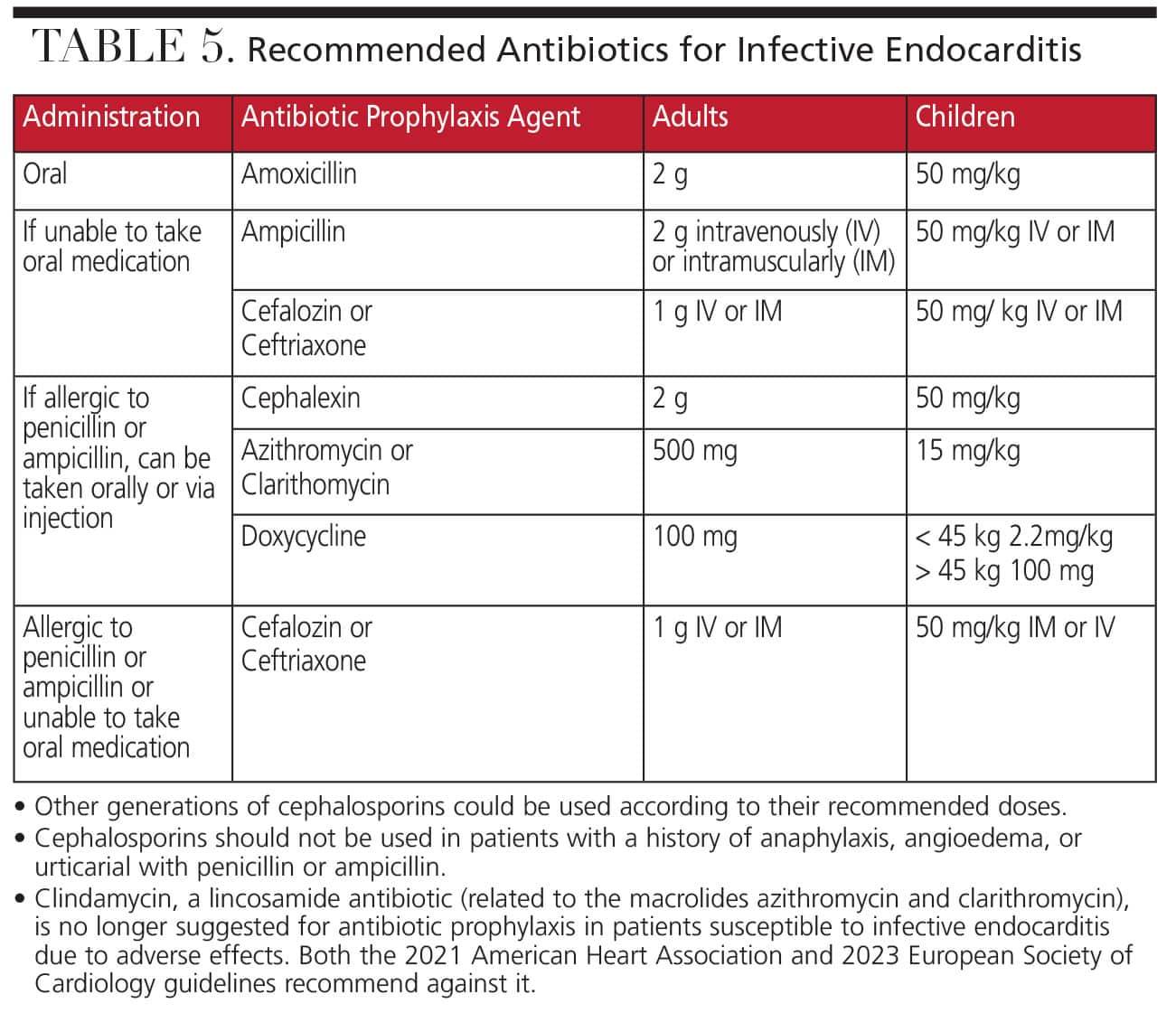
In the dental setting, AP is administered in a single dose for a low magnitude transient exposure to a microorganism 30 to 60 minutes before the dental procedure in order to allow the antibiotic to reach adequate blood levels.5 If the AP is not administered before the dental procedure, then it may be administered up to 2 hours after the procedure (Table 5).5
If the AP is not administered pre- or post-operatively within the recommended time frame, no antibiotic should be given. The patient should be informed and advised to reach out to his or her primary care provider.31 As established in AHA’s 2007 guidelines and retained in the 2021 guidelines, if a patient received 7 to 10 days of pre-operative antibiotics, a different class of antibiotics should be chosen for the procedure to reduce the risk of antibiotic resistance. If possible, the elective dental procedure should be postponed for at least 10 days after the completion of the short course of antibiotics. For patients undergoing multiple sequential dental procedures, the next procedure should be delayed for 10 days after the last dose of antibiotic therapy.5 In this scenario, the same class of antibiotics can be used.
The inappropriate use of antibiotics can lead to antibiotic resistance. The US Centers for Disease Control and Prevention estimates that, in 2019, antibiotic-resistant infections caused over 2 million illnesses, resulting in 23,000 deaths and tens of billions of dollars in healthcare costs. Certain antibiotics, such as the macrolide clarithromycin, are more likely to contribute to the development of resistance than a beta-lactam, such as penicillin. Nonetheless, there was not sufficient evidence for the AHA to change its 2007 AP guidelines.5
In addition to implementing an AP protocol for high-risk patients, oral health professionals should educate patients with cardiovascular disease about the significance of oral hygiene in reducing their risk of IE. This dual approach will improve patient care and minimize the risk of IE in vulnerable populations. Patients should be educated on the importance of proper oral hygiene, such as regular toothbrushing, flossing, and seeking routine dental care to reduce bacterial load. This reduction is essential for preventing IE, reinforcing the need for both personal oral care and professional dental support in at-risk populations.32
The AHA and ESC suggest that maintenance of good oral health and regular access to dental care are considered more important to prevent IE than AP for a dental procedure. With the combination of AP administered to high-risk individuals and consistent good oral hygiene, the risk of developing IE is significantly decreased.5
Dentists are responsible for prescribing AP for patients at high risk of IE, following the AHA guidelines. In a rare situation in which the patient’s physician doesn’t feel that AP is necessary, the dentist should still follow the AHA guidelines.
Conclusion
AP should be used during dental procedures only for patients with specific underlying cardiac conditions that carry a high risk of adverse outcomes from IE. AP is advised for any dental procedures that manipulate gingival tissue or the periapical region of teeth or perforate the oral mucosa. Moreover, promoting consistent and effective oral hygiene practices for all patients, not just those at high risk for IE, is key.
References
- Jensen AD, Ostergaard L, Petersen JK, et al. Temporal trends of mortality in patients with infective endocarditis: a nationwide study. Eur Heart J Qual Care Clin Outcomes. 2022;9:24-33.
- Cahill TJ, Prendergast BD. Infective endocarditis. Lancet. 2016;387:882-893.
- Wilson W, Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. J Am Dent Assoc. 2007;138:739-745-760.
- Habib G, Erba PA, Iung B, et al. Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC-EORP EURO-ENDO (European infective endocarditis) registry: a prospective cohort study. Eur Heart J. 2019;40:3222-3232.
- Wilson WR, Gewitz M, Lockhart PB, et al. Prevention of Viridans Group Streptococcal Infective Endocarditis: A Scientific Statement From the American Heart Association. Circulation. 2021;143:e963-e978.
- Baddour LM, Weimer MB, Wurcel AG, et al. Management of infective endocarditis in people who inject drugs: a scientific statement From the American Heart Association. Circulation. 2022;146:e187-e201.
- Thornhill MH, Gibson TB, Yoon F, et al. Antibiotic prophylaxis against infective endocarditis before invasive dental procedures. J Am Coll Cardiol. 2022;80:1029-1041.
- Habib G, Lancellotti P, Antunes MJ, et al. 2015 ESC guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015;36:3075-3128.
- Cahill TJ, Dayer M, Prendergast B, Thornhill M. Do patients at risk of infective endocarditis need antibiotics before dental procedures? BMJ. 2017;358:j3942.
- Galar A, Weil AA, Dudzinski DM, Munoz P, Siedner MJ. Methicillin-resistant staphylococcus aureus prosthetic valve endocarditis: pathophysiology, epidemiology, clinical presentation, diagnosis, and management. Clin Microbiol Rev. 2019;32:e00041-118.
- Vilcant V, Hai O. Bacterial Endocarditis. Treasure Island, Florida: StatPearls; 2023.
- Kamde SP, Anjankar A. Pathogenesis, diagnosis, antimicrobial therapy, and management of infective endocarditis, and its complications. Cureus. 2022;14:e29182.
- Hays LH. Infective endocarditis: call for education of adults with CHD: review of the evidence. Cardiol Young. 2016;26:426-430.
- Selton-Suty C, Celard M, Le Moing V, et al. Preeminence of Staphylococcus aureus in infective endocarditis: a 1-year population-based survey. Clin Infect Dis. 2012;54:1230-1239.
- Barnett R. Infective endocarditis. Lancet. 2016;388:1148.
- Di Mauro M, Foschi M, Dato GMA, et al. Surgical treatment of isolated tricuspid valve infective endocarditis: 25-year results from a multicenter registry. Int J Cardiol. 2019;292:62-67.
- Sullam PM, Drake TA, Sande MA. Pathogenesis of endocarditis. Am J Med. 1985;78:110-115.
- Gomes SV, Rodrigues V, Nunes-Dos-Santos DL, Pereira ALA, Peres MA. The relationship between periodontal status and hyperglycemia after kidney transplantation. Clin Oral Investig. 2022;26:397-406.
- Palmer RJ, Jr. Composition and development of oral bacterial communities. Periodontol 2000. 2014;64:20-39.
- Kinane DF, Stathopoulou PG, Papapanou PN. Periodontal diseases. Nat Rev Dis Primers. 2017;3:17038.
- Slots J. Periodontitis: facts, fallacies and the future. Periodontol 2000. 2017;75:7-23.
- Barrau K, Boulamery A, Imbert G, et al. Causative organisms of infective endocarditis according to host status. Clin Microbiol Infect. 2004;10:302-308.
- Dhotre S, Jahagirdar V, Suryawanshi N, Davane M, Patil R, Nagoba B. Assessment of periodontitis and its role in viridans streptococcal bacteremia and infective endocarditis. Indian Heart J. 2018;70:225-232.
- Thornhill MH, Dayer M, Lockhart PB, Prendergast B. Antibiotic prophylaxis of infective endocarditis. Curr Infect Dis Rep. 2017;19:9.
- Carinci F, Martinelli M, Contaldo M, et al. Focus on periodontal disease and development of endocarditis. J Biol Regul Homeost Agents. 2018;32:143-147.
- Forner L, Larsen T, Kilian M, Holmstrup P. Incidence of bacteremia after chewing, tooth brushing and scaling in individuals with periodontal inflammation. J Clin Periodontol. 2006;33:401-407.
- Ninomiya M, Hashimoto M, Yamanouchi K, Fukumura Y, Nagata T, Naruishi K. Relationship of oral conditions to the incidence of infective endocarditis in periodontitis patients with valvular heart disease: a cross-sectional study. Clin Oral Investig. 2020;24:833-840.
- Nakatani S, Mitsutake K, Ohara T, et al. Recent picture of infective endocarditis in Japan — lessons from Cardiac Disease Registration (CADRE-IE). Circ J. 2013;77:1558-1564.
- Lockhart PB, Brennan MT, Sasser HC, Fox PC, Paster BJ, Bahrani-Mougeot FK. Bacteremia associated with toothbrushing and dental extraction. Circulation. 2008;117:3118-3125.
- Delgado V, Ajmone Marsan N, de Waha S, et al. 2023 ESC Guidelines for the management of endocarditis. Eur Heart J. 2023;44:3948-4042.
- Martico M., Kapageridis H, Ouanounou A. Infective endocardis: etiology, epidemiology and current recommendations for the dental practitioner. J Can Dent Asoc. 2024;90;4.
- Del Giudice C, Vaia E, Liccardo D, et al. Infective endocarditis: a focus on oral microbiota. Microorganisms. 2021;9:1218.
From Decisions in Dentistry. May/June 2025;11(3):28-31.

