
 PEAKSTOCK/ISTOCK/GETTY IMAGES PLUS
PEAKSTOCK/ISTOCK/GETTY IMAGES PLUS
Applications for Acupuncture in Dentistry
An overview of this ancient technique and the most common oral conditions that can be treated with acupuncture therapy.
PURCHASE COURSE
This course was published in the August 2020 issue and expires August 2023. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the August 2020 issue and expires August 2023. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe the basic concepts of acupuncture therapy, and indications for its use in oral healthcare.
- Discuss the evidence for acupuncture’s efficacy in dental treatment.
- Explain the effects of acupuncture in managing dental pain and related conditions.
General dentists can help their patients and practices by being knowledgeable about acupuncture techniques for oral healthcare. This paper reviews the most common oral conditions that can be treated with acupuncture. Part of traditional Chinese medicine, this is a technique in which practitioners stimulate specific points on the body by inserting thin, flexible, sterile needles through the skin (Figure 1). Acupuncture points can also be stimulated with acupressure, transcutaneous nerve stimulation, and lasers.1
Dentists can use acupuncture for treating patients within the scope of their dental license, which is regulated by each state; the requirements vary from state to state. Physicians and acupuncturists can use acupuncture for treating the whole body and all medical conditions.
The rationale behind all traditional Chinese medicine therapies is to restore qi (pronounced chee), which is vital energy that flows through the meridians. The meridians are branches connected to body organs and function through complicated nonanatomical pathways. By stimulating the acupuncture points, the flow of energy is harmonized and optimal health can be restored. Research on acupuncture has shown evidence of efficacy, according to evidence-based medicine principles in both the medical and dental fields.2
Acupuncture is a safe treatment modality because it is nontoxic and has minimal adverse reactions. Furthermore, in contrast to the use of certain drugs, there is no risk of dependency. The disadvantages are that acupuncture is time consuming, and, in some individuals, may fail to bring about complete relief of symptoms. It is not suitable for children because few children will tolerate needles, and it cannot be used effectively in needle-phobic patients. While rare, improper needle insertion can cause serious adverse events and tissue injury.3 In a large-scale survey of 2.2 million consecutive acupuncture treatments, adverse events were detected in two patients: pneumothorax and lower limb nerve injury.4
According to a 2003 World Health Organization report, pain in dentistry — including dental pain, facial pain and postoperative pain — ranks among the conditions that acupuncture has successfully treated in controlled trials.5 Numerous randomized controlled trials have reported on the analgesic efficacy of acupuncture for postoperative pain caused by various dental procedures.6,7

MECHANISMS OF ACTION
Does acupuncture work as a placebo? Our understanding of the biological and psychological mechanisms underlying placebo effects has expanded significantly due to recent developments in brain imaging technology. Based on findings from brain-imaging analyses, it is known that placebo analgesia is a real (i.e., biologically measurable) phenomenon. It can be blocked by drugs such as naloxone, and behaviorally enhanced, and these responses have been demonstrated to be similar to those elicited by the administration of “real” analgesic substances.8
Psychological mechanisms involved in placebo analgesia include expectancy (i.e., response) and classical conditioning.9–11 Modern science now understands a placebo response is inherent in all types of treatments. Built into the procedure, acupuncture involves powerful actions that contribute to a placebo effect, such as hands-on touching, and a new exotic treatment. The acupuncturist is confident and caring. The placing of needles into the body with minimal pain enhances the patient’s experience and expectation, as does the sensation of the chi response and the acupuncturist’s positive reaction. Last, but not least, acupuncture is somewhat foreign to the Western culture, and it may be perceived as magical or spiritual.12
The fundamental theories of acupuncture-induced analgesia can be summarized in three mechanisms:
- Acupuncture stimulates the peripheral afferent A-delta fibers, which then project to the higher centers in the central nervous system, where midbrain structures, such as the periaqueductal gray matter and raphe nucleus magnus, are involved. The net result is a release of endorphins that, with enkephalin and dynorphin, are mostly involved in pain blocking.13
- Additional mechanisms include segmental inhibition and the activation of the adrenergic and 5-hydroxytryptamine (serotonin) systems; in response to acupuncture stimulation, norepinephrine and serotonin in the spinal cord are released, which inhibit pain, both presynaptically and postsynaptically. This diminishes pain signal transmission all through the spinothalamic tract. Acupuncture, therefore, also enhances the descending inhibitory pathways and modulates pain.14
- The stimulation of the pituitary-hypothalamic complex — which evokes the systemic release of beta-endorphin — also releases adrenocorticotropic hormone, and subsequently accounts for an increased level of cortisol, with beneficial effects on inflammation and stress.15
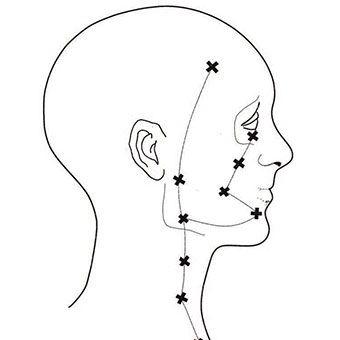
WHAT ARE ACUPUNCTURE POINTS?
Acupuncture points are essential components of acupuncture therapy for both diagnosis and treatment (Figure 2), and have been shown to correspond to myofascial trigger points in Western medicine.16 Trigger points are called ashi points in traditional Chinese medicine and are usually needled (Figure 3).17 Yet despite their historic use, numerous anatomical and histological studies have failed to yield clear evidence of the existence of trigger points.18
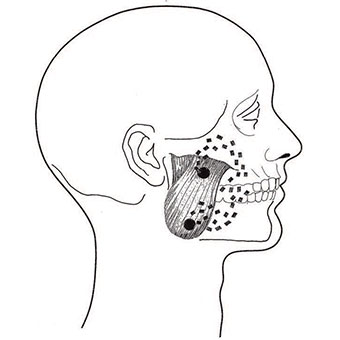
muscle with referral pattern.
Some of the oral conditions for which acupuncture can be used safely and effectively include:
- Dental pain (acute and postoperative)
- Dental anxiety
- Nausea and gag reflex
- Burning mouth syndrome (BMS)
- Orofacial pain
1. Acute and postoperative dental pain: Acupuncture analgesia is an adjunctive measure for pain control in patients with acute dental pain. Studies have shown that acupuncture is at least as effective as nonsteroidal anti-inflammatory drugs in controlling pain after oral surgery (a wisdom tooth extraction, for example).19
2. Dental anxiety: Use of acupuncture can help eliminate or minimize fear of pain from the dental injection.20 In 2010, Rosted et al21 examined the effect of acupuncture administered before dental treatment on patients’ level of anxiety. All patients received acupuncture treatment for five minutes before the planned dental treatment. There was a significant reduction in the anxiety scores after treatment with acupuncture (Figure 4).
3. Nausea and gag reflex: Nausea and gagging make it a challenge when trying to acquire an impression or place a dental restoration. The efficacy of acupuncture in controlling the gag reflex is unclear. Nevertheless, the stimulation of the acupuncture points, especially pericardium-6 (P-6), seems to provide a remarkable reduction of the gag reflex (Figure 5).22–26

4. Burning mouth syndrome: According to the International Headache Society, BMS is an idiopathic condition consisting of an intraoral burning or dysesthesia recurring daily for more than two hours per day over more than three months, without clinically evident causative lesions.27 This condition mainly affects females in the fifth to seventh decade and can involve multiple sites, with the tip of the tongue being the most common location (71%), followed by the lips (50%), lateral border of the tongue (46%), and palate (46%).28 A systematic review of acupuncture or injection of local anesthetic into an acupoint for the management of BMS showed positive results.29

Another randomized controlled trial found that acupuncture and clonazepam are similarly effective for BMS.30 Research shows combined acupuncture and auriculotherapy is effective in reducing the intensity of BMS and improving quality of life.31 A published case series of 11 patients who had been diagnosed and treated with clonazepam and were still having significant pain showed positive results after three acupuncture treatments. The ratings for pain and rest were significantly improved.32
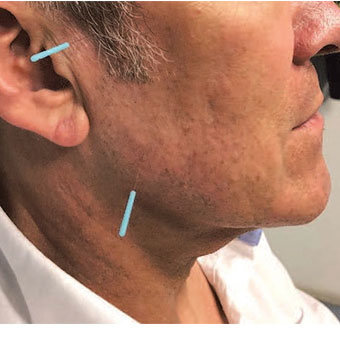
5. Orofacial pain: Dental pain aside, the most common causes of orofacial pain are temporomandibular disorders (TMD),33 which comprise several conditions with signs and symptoms involving the temporomandibular joints, masticatory muscles or associated structures.34 A systematic review suggests there is moderate evidence that acupuncture is an effective intervention in reducing the symptoms associated with TMD.35 Increasing evidence also supports the use of acupuncture in myofascial pain disorders.36 These triggers are the equivalent of ashi points (Figure 6). Symptoms of myofascial pain include tenderness, headaches, restricted movement, and muscle stiffness and weakness.16

A systematic review of 33 trials with 1692 patients that used acupuncture for myofascial pain found that most acupuncture therapies, including acupuncture combined with other treatments, were effective in decreasing pain and improving physical function (Figure 7).37
ACUPUNCTURE TREATMENT PLAN
A good history, including past medical history, and an extensive clinical examination with attention to painful joints, nerve abnormalities and muscle tender points (especially distant pain referral) is essential for an accurate diagnosis. A suitable acupuncture treatment plan can be developed based on the diagnosis. The treatment plan will include the use of one or more distal points to draw the pain away. Distal points have a greater central nervous system effect. Examples include the P-6 on the wrist for gagging (Figure 5), and Li-4 on the hand for pain (Figure 8). Local trigger points in the area of the chief complaint are also chosen (ashi points; Figure 7). Finally, auxiliary points based on the patient’s condition are chosen to reduce stress, anxiety, or impart a general feeling of well-being.

CONCLUSION
Acupuncture can be a useful adjunct in dentistry. There is a large body of scientific evidence supporting the safe use of acupuncture for pain, anxiety and gagging. Dentists can help their patients and expand their practice offerings by learning to perform acupuncture or referring patients to an acupuncturist.38
References
- Veith I. Acupuncture in traditional Chinese medicine. An historical review. Calif Med. 1973;118:70–79.
- Lewin AJ. Acupuncture and its role in modern medicine. West J Med. 1974;120:27–32.
- Chan MW, Wu XY, Wu JC, Wong SY, Chung VC. Safety of acupuncture: overview of systematic reviews. Sci Rep. 2017;7:3369.
- Witt CM, Pach D, Brinkhaus B, et al. Safety of acupuncture: results of a prospective observational study with 229,230 patients and introduction of a medical information and consent form. Forsch Komplementmed. 2009;16:91–97.
- Acupuncture: review and analysis of reports on controlled clinical trials. Available at: http://digicollection.org/hss/en/d/Js4926e/. Accessed June 19, 2020.
- Rosted P. Introduction to acupuncture in dentistry. Br Dent J. 2000;189:136–140.
- Naik PN, Kiran RA, Yalamanchal S, Kumar VA, Goli S, Vashist N. Acupuncture: an alternative therapy in dentistry and its possible applications. Med Acupunct. 2014;26:308–314
- Tétreault P, Mansour A, Vachon-Presseau E, Schnitzer TJ, Apkarian AV, Baliki MN. Brain connectivity predicts placebo response across chronic pain clinical trials. PLoS Biol. 2016;14:e1002570.
- Kaptchuk TJ, Eisenberg DM. The persuasive appeal of alternative medicine. Ann Intern Med. 1998;129:1061–1065.
- Kaptchuk TJ. Powerful placebo: the dark side of the randomised controlled trial. Lancet. 1998;351:1722–1725.
- Beecher HK. The powerful placebo. JAMA. 1955;159:1602–1606.
- Lao L, Bergman S, Hamilton GR, Langenberg P, Berman B. Evaluation of acupuncture for pain control after oral surgery: a placebo-controlled trial. Arch Otolaryngol Head Neck Surg. 1999;125:567–572.
- Lee A, Chan S. Acupuncture and anaesthesia. Best Pract Res Clin Anaesthesiol. 2006;20:303–314.
- Kawakita K, Okada K. Acupuncture therapy: mechanism of action, efficacy, and safety: a potential intervention for psychogenic disorders? Biopsychosoc Med. 2014;8:4.Lai HC,
- Lin YW, Hsieh CL. Acupuncture-analgesia-mediated alleviation of central sensitization. Evid Based Complement Alternat Med. 2019:6173412.
- Travell J, Rinzler SH. The myofascial genesis of pain. Postgrad Med. 1952;11:425–441.
- Melzack R, Stillwell D, Fox E. Trigger points and acupuncture points for pain: correlations and implications. Pain. 1977;3:3–23.
- Chernyak GV, Sessler DI. Perioperative acupuncture and related techniques. Anesthesiology. 2005;102:1031–1049.
- Gupta D, Dalai DR, Swapnadeep, et al. Acupuncture (zhēn jiǔ) – an emerging adjunct in routine oral care. J Tradit Complement Med. 2014;4:218–223.
- Appukuttan DP. Strategies to manage patients with dental anxiety and dental phobia: literature review. Clin Cosmet Investig Dent. 2016;8:35–50.
- Rosted P, Bundgaard M, Gordon S, Pedersen AM. Acupuncture in the management of anxiety related to dental treatment: a case series. Acupunct Med. 2010;28:3–5.
- Bassi GS, Humphris GM, Longman LP. The etiology and management of gagging: a review of the literature. J Prosthet Dent. 2004;91:459–467.
- Dickinson CM, Fiske J. A review of gagging problems in dentistry: 2. Clinical assessment and management. Dent Update. 2005;32:74.
- Morrish RB. Suppression and Prevention of the Gag Reflex With a TENS Device During Dental Procedures. Available at: https://pubmed.ncbi.nlm.nih.gov/9515420/. Accessed June 19, 2020.
- Hotta H. Case report of difficult dental prosthesis insertion due to severe gag reflex. Bull Tokyo Dent Coll. 2012;53:133–139.
- Daneshkazemi A, Daneshkazemi P, Davoudi A, Badrian H, Firouzabadi VP. Is acupuncturing effective in controlling the gag reflex during dental procedures? A review of literature. Anesth Essays Res. 2016;10:173–177.
- Headache Classification Committee of the International Headache Society. The International Classification of Headache Disorders. 3rd edition. Cephalalgia. 2013;33:629–808.
- Jääskeläinen S, Woda A. Burning mouth syndrome. Cephalalgia. 2017;37:627–647.
- Yan Z, Ding N, Hua H. A systematic review of acupuncture or acupoint injection for management of burning mouth syndrome. Quintessence Int. 2012;43:695–701.
- Kvesic A, Zavoreo I, Basic Kes V, et al. The effectiveness of acupuncture versus clonazepam in patients with burning mouth syndrome. Acupunct Med. 2015;33:289–292.
- Franco FR, Castro LA, Borsatto MC, Silveira EA, Ribeiro-Rotta RF. Combined acupuncture and auriculotherapy in burning mouth syndrome treatment: a preliminary single-arm clinical trial. J Altern Complement Med. 2017;23:126–134.
- Diepp C, Goddard G, Mauro G. Acupuncture improves pain and rest in burning mouth syndrome patients: clinical cases. Dental Cadmos. 2019;87:160.
- Renton T, Durham J, Aggarwal VR. The classification and differential diagnosis of orofacial pain. Expert Rev Neurother. 2012;12:569–576.
- Prasad S, Kumar N, Shruthi H, Kalavathi SD. Temporomandibular pain. J Oral Maxillofac Pathol. 2016;20:272–275.
- Shen Y, Goddard G. Short term effects of acupuncture on myofascial pain patients after clenching. Pain Pract. 2007;7:256–264.
- National Institutes of Health Consensus Panel. Acupuncture: National Institutes of Health Consensus Development Conference Statement. Available at: https://consensus.nih.gov/1997/1997acupuncture107html.htm. Accessed June 19, 2020.
- Li X, Wang R, Xing X, et al. Acupuncture for myofascial pain syndrome: a network meta-analysis of 33 randomized controlled trials. Pain Physician. 2017;20:E883–E902.
- Goddard G, Mauro G. Acupuncture for Dentistry and Orofacial Pain. Bloomington, Ind: Balboa Press; 2020:21–22.
From Decisions in Dentistry. July/August 2020;6(7):32-35.

