
Treating Patients With Cardiovascular Disease and Stroke
The oral health consequences of these common conditions warrant special care strategies.
The oral health consequences of these common conditions warrant special care strategies
PURCHASE COURSE
This course was published in the June 2018 issue and expires June 2021. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
The U.S. Census Bureau estimates that by 2050, 21% of the U.S. population will be age 65 or older. As people live longer, the prevalence of age-related chronic conditions, such as cardiovascular disease and stroke, also increases. Cardiovascular disease is responsible for 38.5% of deaths in the United States each year, and 70% of deaths among those older than 75.1 More than 74 million Americans have hypertension, 17.6 million have coronary artery disease, and 5.8 million experience heart failure.1 The U.S. Centers for Disease Control and Prevention (CDC) reports that, annually, about 795,000 people experience strokes; 140,000 of these are fatal, averaging one every four seconds.2 These cardiovascular problems and the medications used to treat them profoundly affect patients’ oral health and the provision of dental care.3
This course was published in the June 2018 issue and expires June 2021. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Describe the prevalence of cardiovascular disease and stroke in the U.S. population — and the health consequences of these conditions.
- Explain the impact of international normalized ratio testing on treatment planning, as well as the new guidelines for hypertension and their bearing on elective procedures.
- List oral health care strategies for treating patients who have experienced cardiovascular disease or stroke.
The following case study prompted the authors to write this article in the hope that lessons learned would be of value to other practitioners. It will review hypertension, coronary artery disease, heart failure, cardiomyopathy and stroke — along with practical applications for dental treatment.
According to new guidelines issued by the American Heart Association in November 2017, hypertension is an arterial pressure greater than 130/80 mm Hg. Uncontrolled hypertension is a risk factor for cerebrovascular accident (stroke), atherosclerosis, myocardial infarction, congestive heart failure, and chronic renal failure.1,2,4–6 Individuals with blood pressure of 120/80 mm Hg or lower are 50% less likely to have a stroke than those with high blood pressure.1,2 Although the cause of hypertension is not known, contributing factors include smoking, high salt intake, high alcohol consumption, kidney disease, adrenal and thyroid problems, stress, advancing age, genetics, being overweight or obese, sedentary lifestyle, poor exercise tolerance, and a family history of hypertension.6 In addition to antihypertensive medications and cholesterol-control therapy, lifestyle changes are recommended in the treatment of hypertension.6
CORONARY ARTERY DISEASE
Coronary artery disease can lead to angina and myocardial infarction; it can also weaken the heart muscle over time, eventually causing heart failure. It is the No. 1 cause of death among American men and women,7-10 and age, genetics, high cholesterol, smoking, hypertension, high triglyceride levels, kidney disease, history of stroke, alcohol abuse, sedentary lifestyle, and high levels of stress are all risk factors. Inflammation — including elevated levels of C-reactive protein — is being investigated as an additional risk factor. Management includes getting cholesterol and blood pressure levels under control. Single antiplatelet therapy, angioplasty and stent placement, coronary artery bypass surgery, and minimally invasive heart surgery are also used to treat coronary artery disease.7–11
Heart failure is most common in men older than 65 and among African-Americans; incidence is 21 per 1000 after age 65 years.12 It starts with a heart muscle damaged from coronary artery disease, hypertension or complications from diabetes.13 Diagnosis is usually confirmed by swelling of the ankles, feet and legs, and sometimes in the abdomen. Fatigue, shortness of breath or difficulty breathing are additional symptoms. Controlled hypertension, normal weight, not smoking, moderate alcohol intake, and consumption of breakfast cereals, fruit and vegetables have been related to reduced risk.11–14 Although heart failure has no cure, the underlying conditions can be controlled. Affected patients should limit their fluids, watch for daily weight gain, and maintain a diet low in salt. Medications commonly taken include diuretics, angiotensin-converting enzyme inhibitors, beta-blockers, metoprolol and digoxin.3,12–15
STROKE
A cerebrovascular accident is the interruption of the blood supply to the brain due to the blockage or bursting of a blood vessel in the brain. Stroke is most often caused by chronic hypertension, but risk factors include atrial fibrillation, diabetes, family history of stroke, high cholesterol and advanced age. As the fifth leading cause of death in the United States, stroke is a significant contributor to physical and cognitive disability in adults.2,3 While two-thirds of strokes occur in individuals age 65 and older,2,3 the CDC notes that incidence is increasing among young and middle-aged people, which may be related to the rise in obesity.3 Stroke often results in loss of motor control and coordination, which, in turn, cause dysphagia and/or dysarthria. Stroke can also weaken the tongue, soft palate, pharynx and muscles of mastication.3 Stroke survivors may also suffer from paralysis or numbness and pains in their hands that could affect oral self-care.16 Obstructive sleep apnea is common after stroke and can have detrimental oral effects, such as bruxism, hypersensitivity, increased risk of periodontal disease and xerostomia-related caries.17–20 Treatment for stroke may include thrombolytic therapy, use of blood thinners and/or surgery. In addition, the use of tissue plasminogen activator therapy has increased the numbers of stroke patients who do not require post-acute care.21,22
CASE STUDY
A 78-year-old woman who lives with her daughter and has a full-time caregiver visits the authors’ faculty practice. The patient, Mrs. Potts (name has been changed), suffered an ischemic stroke 30 years ago, resulting in hemiplegia on her left side and aphasia. Before initial treatment, both her primary physician and cardiologist were consulted and her medical history reviewed. With older adults, it is imperative to update medical histories at every visit, as medications and medical conditions can change frequently. Dental professionals should inform caregivers that it is important to report any change in health status or medications because it can affect dental treatment plans.
The patient’s medical history includes common risks for stroke: chronic hypertension, osteoporosis, atherosclerosis, smoking (35 years), and heart disease. She also has a history of depression, kidney stones, and deep vein thrombosis, in addition to a seizure disorder caused by her stroke. Her medications, along with indications for use and possible interactions, are listed in Table 1. The initial oral exam revealed that Mrs. Potts had severe root caries and moderate periodontitis. After consultation with her physician, hospitalization was recommended for extraction of teeth #3, #13, #19 and #31. Her international normalized ratio (INR) was 3.0. (If INR is tested 24 hours prior to a dental procedure and is less than 3.5, antiplatelet and warfarin therapy need not be discontinued.)22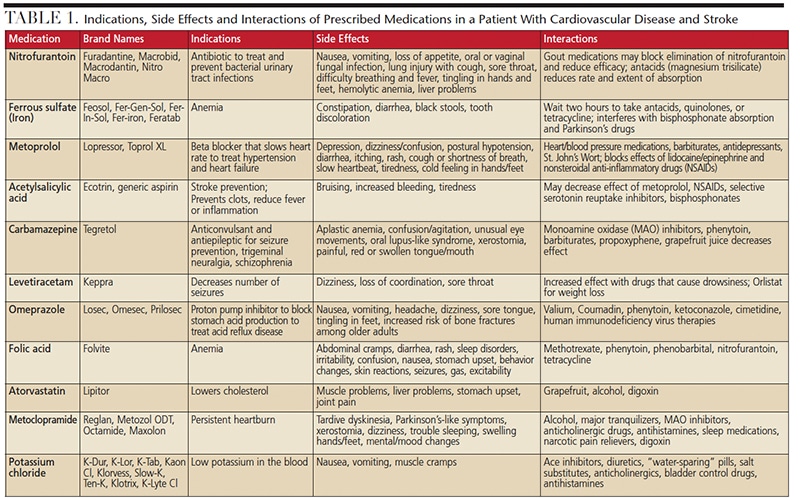
Oral preventive measures included four quadrants of scaling and root planing (with fluoride varnish) and a resin-modified glass ionomer on #18. The patient was placed on a four-week recall for ultrasonic debridement and fluoride varnish treatments; in addition, amorphous calcium phosphate and casein phosphopeptide toothpaste was recommended for home care. No partial denture was ordered to replace the extracted teeth because Ms. Potts, like many stroke patients, has paresthesia and thus could not feel if the prosthesis caused trauma to the oral tissues. As with this patient, motor nerve supply damage to the face by cranial nerve VII may occur in the brain, resulting in loss of oral muscle tone, and reduced chewing efficiency and lip force on the affected side.16 Mrs. Potts often had food debris accumulated on her affected side and was not capable of feeling it.21 Because her caregiver brought her to appointments, we were able to teach the caregiver about these conditions and techniques to address them. Treatment planning should consider the patient’s unique situation and capabilities.21 Support must be offered for daily activities (including help with oral care) and evaluation for depression and visual perceptual difficulties. An interdisciplinary team approach is advised for any stroke patient to ensure comprehensive care.22,23
Because Mrs. Potts has a history of myocardial infarction and hypertension, we limited the administration of any vasoconstrictor during the provision of local anesthesia. Aspiration and the slow injection of the minimal effective dose (not to exceed 0.04 mg of epinephrine within a 15-minute period or more than two cartridges of 1:100,000 epinephrine-containing anesthesia) are recommended in patients with cardiovascular conditions.24 Her appointments were always scheduled for late morning or early afternoon because circadian patterns elevate vascular tone and increase fibrinolytic activity and platelet aggregation between 6:00 am and 9:00 am, which increases the risk of myocardial infarction and stroke.24
Short appointments were scheduled to avoid overstressing the patient and care was taken to sit her up slowly to prevent orthostatic hypotension. When providing dental treatment to this patient population, oxygen should always be readily available because stress from the procedure can increase cardiac oxygen demand. Mrs. Potts’ blood pressure was routinely checked before she left the clinic. Due to this patient’s chronic bilateral carotid artery occlusions, her circulation is dependent on vertebral arteries and external carotid artery collaterals. Thus, care was taken to avoid extreme flexion and extension of her head during procedures. (When treating patients who present with this condition or neck problems, an inflatable travel pillow is helpful for support and can easily be covered and disinfected after use.) At the start of one appointment, Mrs. Potts’ blood pressure was high (185/98 mm Hg). We allowed her to sit quietly for 10 minutes and checked the pressure again. It did not come down, so her debridement procedure was rescheduled. The 2017 American Heart Association/American College of Cardiology guidelines state that it is generally unsafe to perform elective procedures on patients with blood pressure readings greater than 180/110 mm Hg.25
PREVENTIVE INTERVENTIONS
Mrs. Potts has severe xerostomia. Often, when sensory deficits are present and there is difficulty swallowing, a concurrent reduction in fluid intake occurs. This, along with medication use, can result in xerostomia. These facts were relayed to the caregiver. If a patient is on oxygen therapy, the potential for xerostomia is further increased. A consequence of dry mouth is oral malodor, which may lead to social isolation and avoidance by caregivers or others.26 In addition, speech problems and taste alterations may affect quality of life.27 With patients such as Mrs. Potts — who, due to the severity of her stroke, is incapable of self-care — oral hygiene education should be provided to both the patient and caregiver to ensure comprehension and follow-up.
We provided written instructions to Mrs. Potts’ caregiver. The mouth should be kept moist by applying cocoa butter to patient’s lips and oral moisturizers to the inside of the cheeks. Foam swabs or toothettes, which are typically used to clean the mouth in hospitals, may remove food debris or apply moisturizing gels, but they do not remove biofilm adequately to prevent periodontal disease or caries. Caregivers should be instructed on how to brush the patient’s teeth. A power toothbrush is often easier for caregivers to use. Because the risk of caries and periodontal disease is extremely high in this population, the use of 5000 ppm fluoride toothpaste, xylitol products (if tolerated gastrointestinally), and an antimicrobial mouthrinse is indicated.28 If patients cannot rinse their mouths, a small amount of mouthrinse can be applied intraorally with gauze, a cotton swab or toothette. In addition to brushing after each meal, an amorphous calcium phosphate product can be swabbed on the teeth to supersaturate the saliva with calcium to promote remineralization.
SUMMARY
Mrs. Potts is fortunate to have a daughter and a full-time caregiver who are concerned about her oral health. Each appointment with Mrs. Potts affords a new learning experience and requires that we adapt our care to the patient’s changing needs. As the American population ages, oral health professionals will be called upon to treat a greater number of older patients, many of whom will be home-bound or institutionalized. All too often, however, this population is not considered during access-to-care strategizing and educational efforts. In particular, the link between oral and systemic health underscores the importance of implementing care strategies that address the special needs of individuals who, like the patient in this case report, present with cardiovascular disease or stroke.
REFERENCES
- Scully C, Ettinger R. The influence of systemic diseases on oral health care in older adults. J Am Dent Assoc. 2008;139:252–253.
- U.S. Centers for Disease Control and Prevention. Stroke. Available at: www.cdc.gov/stroke. Accessed May 3, 2018.
- Benjamin EJ, Blaha MJ, Chiuve SE, et al. Heart Disease and Stroke Statistics — 2017 Update: A Report From the American Heart Association. Available at: circ.ahajournals.org/content/early/2017/01/25/CIR.0000000000000485. Accessed May 3, 2018.
- American Heart Association. Understanding Blood Pressure Readings. Available at: www.heart.org/HEARTORG/Conditions/HighBloodPressure/KnowYourNumbers/Understanding-Blood-PressureReadings_UCM_301764_Article.jsp#.WntV6-dG2Uk. Accessed May 3, 2018.
- Little JW, Falace D, Miller C, Rhodus NL. Dental Management of the Medically Compromised Patient. 8th ed. St. Louis, Mo: Mosby; 2015.
- Yoon SS, Carroll MD, Fryar CD. Hypertension prevalence and control among adults: United States, 2011–2014. NCHS Data Brief. 2015;220:1–8.
- Mosca L, Benjamin EJ, Berra K, et al. Effectiveness-based guidelines for the prevention of cardiovascular disease in women — 2011 update: a guideline from the American Heart Association. Circulation. 2011;123:1243–1245.
- Morrow DA, Gersh BJ. Chronic Coronary Artery Disease. In: Libby P, Bonow RO, Mann DL, Zipes DP, eds. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. 8th ed. Philadelphia: Saunders Elsevier; 2007.
- Vandvik PO, Lincoff AM, Gore JM, et al. Primary and secondary prevention of cardiovascular disease: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(Suppl 2):e637S–e668S.
- Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronary intervention versus coronary artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360:961–972.
- U.S. Preventive Services Task Force. Aspirin for the Prevention of Cardiovascular Disease: U.S. Preventive Services Task Force Recomendation Statement. Ann Intern Med. 2009;150:396–404.
- Huffman MD, Berry JD, Ning H, et al. Lifetime risk for heart failure among white and black Americans: cardiovascular lifetime risk pooling project. J Am Coll Cardiol. 2013;61:1510–1517.
- Boucher JL, Hurrell DG. Cardiovascular diseases and diabetes. Diabetes Spectrum. 2008;21:154–155.
- Djoussé L, Driver JA, Gaziano JM. Relation between modifiable lifestyle factors and lifetime risk of heart failure. JAMA. 2009;302:394–400.
- Tong X, Kuklina EV, Gillespie C, George MC, CDC. Trends of acute ischemic stroke hospitalizations by age and gender in the United States: 1994–2007. Presented at: International Stroke Conference, February 8–11, 2011; Los Angeles.
- National Institute of Neurological Disorders and Stroke. Stroke Information Page. Available at: www.ninds.nih.gov/Disorders/All-Disorders/Stroke-Information-Page#disorders-r1. Accessed May 3, 2018.
- Redline S, Yenokyan G, Gottlieb DJ, et al. Obstructive sleep apnea-hypopnea and incident stroke: the Sleep Heart Health Study. Am J Respir Crit Care Med. 2010;182:269–277.
- Dong JY, Zhang YH, Qin LQ. Obstructive sleep apnea and cardiovascular risk: meta-analysis of prospective cohort studies. Atherosclerosis. 2013;229:489–495.
- Loke YK, Brown JW, Kwok CS, Niruban A, Myint PK. Association of obstructive sleep apnea with risk of serious cardiovascular events: a systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 2012;5:720–728.
- Li M, Hou WS, Zhang XW, Tang ZY. Obstructive sleep apnea and risk of stroke: a meta-analysis of prospective studies. Int J Cardiol. 2014;172:466–469.
- Weltman NJ, Al-Attar Y, Cheung J, et al. Management of dental extractions in patients taking warfarin as anticoagulant treatment: a systematic review. J Can Dent Assoc. 2015;81:f20.
- Elad S, Marshall J, Meyerowitz C, Connolly G. Novel anticoagulants: general overview and practical considerations for dental practitioners. Oral Dis. 2016;22:23–32.
- Schimmel M, Leemann B, Christou P, et al. Oral health-related quality of life in hospitalized stroke patients. Gerodontology. 2009;10:1741–1750.
- Shaw E, Tofler GH. Circadian rhythm and cardiovascular disease. Curr Atheroscler Rep. 2009;11:289.
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summaryda report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines J Am Coll Cardiol. November 7, 2017. Epub ahead of print.
- Koshimune S, Awano S, Gohara K, Kurihara E, Ansai T, Takehara T. Low salivary flow and volatile sulfur compounds in mouth air. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96:38–41.
- Habbab KM, Moles DR, Porter SR. Oral diseases. Potential oral manifestations of cardiovascular drugs. Oral Dis. 2010;16:769–773.
- Featherstone JD, Doméjean-Orliaguet S, Jenson L, Wolff M, Young DA. Caries risk assessment in practice for age 6 through adult. J Calif Dent Assoc. 2007;35:703–713.
Featured image by STOCKDEVIL/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. June 2018;4(6):26–29.

