

Selection Guidelines for All-Ceramic Restorations
Clinicians must understand the physical and esthetic properties of these materials in order to provide appropriate treatment recommendations.
Clinicians must understand the physical and esthetic properties of these materials in order to provide appropriate treatment recommendations
Due to improvements in materials and the sustained demand for esthetic and metal-free restorations, the use of all-ceramic restorations has become ubiquitous.1 Although there is a plethora of all-ceramic systems, many are becoming obsolete almost as quickly as they were introduced due to the distinct advantages of lithium disilicate and zirconia. The wide range of clinical applications for these materials includes veneers, partial-coverage crowns, crowns and fixed dental prostheses (FDP).2
Successful application of all-ceramic materials depends on the practitioner’s ability to select both the appropriate material and cementation protocol that satisfy the patient’s needs and expectations.3 The selection of a particular ceramic system should be based on physical properties — such as strength, fracture resistance, wear resistance and long-term outcomes — as well as esthetic considerations. Hence, the dentist must understand these materials and systems so he or she can educate patients and present appropriate treatment options. This article will review clinical considerations for choosing all-ceramic materials.
LITHIUM DISILICATE CERAMICS
On the market for almost 15 years, lithium disilicate restorations are typically monolithic, meaning the full contour of the prosthesis is fabricated from a single material and is homogeneous throughout. Lithium disilicate offers lifelike translucency, opalescence and light diffusion, and can be stained, glazed or cut back to layer veneering porcelain to enhance incisal characterization (Figure 1 and Figure 2). These restorations can be fabricated by milling ceramic blocks. After milling, the restoration is classified as being in its “green state.” It then undergoes crystallization at high temperature, and external staining and glazing at lower temperatures. This procedure can be done in office with computer aided design and computer aided milling (CAD/CAM) technology, or at a dental laboratory. Lithium disilicate prostheses can also be fabricated by laboratories by pressing the material into a wax pattern. Due to its high strength — which ranges from 360 megapascals (MPa) to 400 MPa4 — lithium disilicate can be used for inlays, onlays, three-quarters crowns, full-coverage crowns, and short-span bridges in the anterior and premolar areas.5


ZIRCONIA-BASED CERAMICS
Zirconia restorations are popular and widely used due to their high strength.6 These restorations are fabricated using CAD/CAM technology (similar to the milling process outlined for lithium disilicate). They can be fabricated as monolithic restorations used for posterior crowns, as well as a layered, or bilaminate, crown. In the case of the bilaminate crown, the high-strength zirconia coping is veneered with hand-stacked or milled nanofluorapatite glass ceramic. The flexural strength of this material ranges from 900 MPa to 1200 MPa.7
MATERIAL CHOICE GUIDELINES
If a patient expresses interest in highly esthetic, metal-free restorations, the indications and/or limitations of the all-ceramic options must be considered. These include the amount of remaining tooth structure, position in the dental arch (esthetic versus functional zone,) and any parafunctional habits. Additional esthetic considerations include the color of underlying tooth structure and the translucency of adjacent teeth.3

When considering the wide range of options for indirect restorations, it helps the practitioner to categorize oral zones in general terms. The esthetic zone primarily refers to the teeth in the anterior sextant, although the considerations that apply to the esthetic zone can extend as far back as the first molar, depending on the patient’s smile line, facial musculature and cosmetic expectations. The functional zone primarily refers to the premolars and molars, and, at times, the anterior sextant, depending on the patient’s dentition. The premolars typically fall into both categories. The anterior teeth also serve in a functional capacity, of course, but the forces generated by anterior guidance and lateral excursions typically fall short of the occlusal loading forces of the functional zone (Figure 3).
Occlusal forces are a factor when considering indirect restorations in the functional zone. Edentulism, proximity to the gnasthostomatic fulcrum (i.e., temporomandibular joint), parafunctional habits and occlusal plane discrepancies can all increase the demands placed on a prosthesis. Traditionally, metal copings provided the strength for porcelain-fused-to-metal (PFM) crowns. While adhesive failures can occur at the metal/porcelain interface when inadequate space is provided for the lab technician to stack the various layers, provided appropriate reduction is achieved, the fusion of the veneering porcelain to the metal coping is highly predictable. Because PFMs require fairly heavy reduction, the materials and lab technicians’ abilities limit esthetics. Zirconia provides an alternative to the gray metal coping, while also offering high flexural strength. In the early days of veneered zirconia crowns, many instances of these junctional adhesive failures were reported.8 Lab techniques for bonding the layering porcelain have improved, however, which has greatly reduced adhesive material failures. Practitioners have also modified the preparation design such that the functional areas of the restoration (e.g., functional cusps, marginal ridges and occlusal form) are brought to full contour with monolithic zirconia, and the nonfunctional areas (e.g., buccal surfaces or nonfunctional cusps) are layered. This design is similar to a three-quarters occlusal metal design for a PFM (Figure 4).

MONOLITHIC RESTORATIONS
More recently, the demand for good esthetics with excellent strength in the functional zone has been answered with advanced monolithic materials. Both lithium disilicate and monolithic zirconia crowns provide high strength and excellent esthetics in the functional zone and have shown reliable clinical performance in the literature.9 The latest monolithic zirconia products claim lifelike translucency and opalescence, and the ability to be milled with multiple shades (Figure 5). They are also excellent at blocking underlying dark tooth structure (Figure 6 and Figure 7).



Considerations for the esthetic zone include the patient’s expectations, existing restorations that need to be matched, and quality and quantity of the remaining tooth structure. As such, a wide range of options is available. Most restorative solutions — ranging from PFM crowns to lithium disilicate to layered zirconia crowns — are acceptable in terms of function (Table 1). A hybrid lithium disilicate full-coverage crown provides excellent esthetics and strength.9 The term hybrid refers to an incisal third cut back by the lab (either CAD premilling or after milling by hand) and stacked with layering ceramic for depth and translucency. This option provides a strong, stable, full-contour lithium disilicate crown with an added esthetic enhancement. Note this is different, however, than milling a coping and stacking to full contour with layering porcelain (i.e., a true bilaminate). Lithium disilicate crowns milled from a high-opacity ingot offer the ability to block out underlying dark tooth structure.
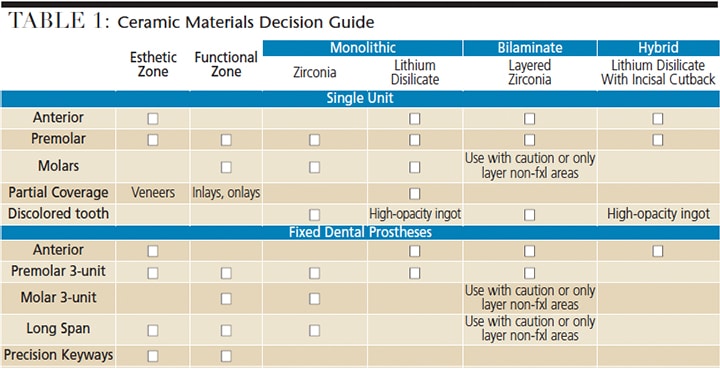
As adhesive bonding technology improves — and bonding capabilities are evermore predictable — the reliance on traditional resistance and retention form for indirect restorations is diminishing. This provides more options for preserving healthy tooth structure by utilizing bondable ceramics in the form of onlays and inlays (which require minimally invasive preparations). If it is possible to retain a portion of healthy tooth structure, a bonded inlay or onlay might be preferable to a large, multisurface posterior composite.10 At present, lithium disilicate is the go-to option for partial coverage in the functional zone, as it is a bondable substrate that provides reliable strength (Figure 8 and Figure 9).11 It should be noted, however, that pure monolithic zirconia is not recommended for nonretentive preparations.


Regarding restoration with a FDP, material manufacturers have very specific guidelines for each type of material based on in-vitro testing (Table 1). Studies have shown promising clinical performance with monolithic zirconia for a wide range of bridge types.11 Similar adhesive failures exist for bilaminate FDPs as for bilaminate single-unit crowns.11
Based on occlusal forces, lithium disilicate FDPs have a restricted range of use, which includes anterior bridges and three-unit premolar bridges; following these parameters, research indicates excellent survival and success rates.12,13 If the practitioner is considering a precision connector or keyway, a traditional metal-ceramic FDP is still recommended, and this is also true for surveyed partial denture abutment crowns.
CEMENTATION OR BONDING
When deciding on a cementation or bonding protocol, clinicians have many options, ranging from resin modified glass ionomers (RMGI), self-adhesive resin cements or a full bonding protocol with adhesive resin cement. The prudent clinician will consider the preparation and restoration in terms of its retentive characteristics, as well as material thickness (Table 2). For nonretentive preps (such as inlays, onlays or short preps), a full bonding protocol with adhesive resin cement is recommended. Note that if using a full bonding protocol, material thickness determines whether a dual-cure or light-cure version of the bonding agent and cement should be utilized.
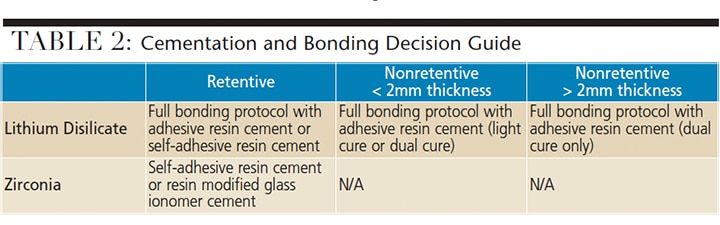
Lithium disilicate crowns have been shown to be more resistant to fracture when an adhesive luting protocol is used (as opposed to a traditional cement, such as RMGI).14 In addition, a dual-cure adhesive resin cement has greater bond strength to lithium disilicate than a self-adhesive resin cement.15 More traditional preparation designs in zirconia can be cemented with an adhesive resin or a glass ionomer cement. What’s more, treating the intaglio surface of zirconia with tribochemical silica sandblasting has been shown to increase bond durability.16
KEY TAKEAWAYS
- Demand for all-ceramic restorations has increased to the point they are becoming the standard of care. The wide range of applications for lithium disilicate and zirconia includes veneers, partial-coverage crowns, crowns and fixed dental prostheses.
- The selection of ceramic materials should be based on physical properties — such as strength, fracture resistance, wear resistance and long-term outcomes — as well as esthetic considerations.
- Predictable outcomes hinge on careful review of the indications and patient considerations for a given case.
- Lithium disilicate and monolithic zirconia crowns provide high strength and excellent esthetics in the functional zone.
- Clinicians have many options when deciding on a cementation or bonding protocol; these range from resin modified glass ionomers and self-adhesive resin cements to a full bonding protocol with adhesive resin cement.
CONCLUSION
In recent years, demand for all-ceramic restorations has increased to the point they are becoming the standard of care. They provide excellent fit, function and esthetics and, if used appropriately, can be reasonable substitutes for metal-ceramic restorations. With improvements in manufacturing and esthetic qualities, demand for all-ceramic materials will continue to grow. Consequently, oral health professionals should remain up to date on developments in materials and cementation protocols. When it comes to choosing the best material and technique, predictable outcomes hinge on careful review of the indications and patient considerations for a specific case.
References
- Santos MJ, Costa MD, Rubo JH, Pegoraro LF, Santos GC Jr. Current all-ceramic systems in dentistry: a review. Compend Contin Educ Dent. 2015;36:31–37.
- Giordano R, McLaren EA. Ceramics overview: classification by microstructure and processing methods. Compend Contin Educ Dent. 2010;31:682–684.
- McLaren EA, Whiteman YY. Ceramics: rationale for material selection. Compend Contin Educ Dent. 2010;31:666–668.
- Culp L, McLaren EA. Lithium disilicate: the restorative material of multiple options. Compend Contin Educ Dent. 2010;31:716–720.
- Etman MK, Woolford MJ. Three-year clinical evaluation of two ceramic crown systems: a preliminary study. J Prosthet Dent. 2010;103:80–90.
- Giordano R, Sabrosa CE. Zirconia: material background and clinical application. Compend Contin Educ Dent. 2010;31:710–715.
- Anusavice K, Shen C, Rawls R. Phillips’ Science of Dental Material.12th ed. St. Louis, MI: Saunders, Elsevier Inc; 2013:418–473.
- Dorri M. All-ceramic tooth-supported single crowns have acceptable 5-year survival rates. Evid Based Dent. 2013;14:47.
- Morimoto S, Rebello de Sampaio FB, Braga MM, Sesma N, Ozcan M. Survival rate of resin and ceramic inlays, onlays and overalys: a systematic review and meta-analysis. J Dent Res. 2016;95:985–994.
- Magne P, Belser UC. Porcelain versus composite inlays/onlays: effects of mechanical loads on stress distribution, adhesion, and crown flexure. Int J Periodontics Restorative Dent. 2003;23:543–555.
- Belli R, Petschelt A, Hofner B, Hajto J, Scherrer SS, Lohbauer U. Fracture rates and lifetime estimations of CAD/CAM all-ceramic restorations. J Dent Res. 2016:95:67–73.
- Gehrt M, Wolfart S, Rafai N, Reich S, Edelhoff D. Clinical results of lithium-disilicate crowns after up to 9 years of service. Clin Oral Investig. 2013;17:275–284.
- Kern M, Sasse M, Wolfart S. Ten-year outcome of three-unit fixed dental prostheses made from monolithic lithium disilicate ceramic. J Am Dent Assoc. 2012;143:234–240.
- Lim MJ, Lee KW. Effect of adhesive luting on the fracture resistance of zirconia compared to that of composite resin and lithium disilicate glass ceramic. Restor Dent Endod. 2017;42:1–8.
- Potiket N, Chiche G, Finger IM. In vitro fracture strength of teeth restored with different all-ceramic crown systems. J Prosthet Dent. 2004;92:491–495.
- Bielen V, Inokoshi M, Munck JD, et al. Bonding effectiveness to differently sandblasted dental zirconia. J Adhes Dent. 2015;17:235–42.
The authors have no commercial conflicts of interest to disclose
From Decisions in Dentistry. March 2017;3(3)24–28.

[…] J, Noble WH, Gupta S, Schulze KA, Hakim F. Selection guidelines for all-ceramic restorations. Decisions in Dentistry. […]