
Oral Effects of Hematopoietic Stem Cell Transplant Therapy
As part of a multidisciplinary team, dental professionals play a pivotal role in managing oral complications from hematopoietic stem cell transplants.
As part of a multidisciplinary team, dental professionals play a pivotal role in managing oral complications from hematopoietic stem cell transplants
PURCHASE COURSE
This course was published in the March 2019 issue and expires March 2022. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the March 2019 issue and expires March 2022. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss hematopoietic stem cells, their role in transplant therapy, and the oral manifestations of these treatments.
- Explain the prevalence of hematopoietic stem cell transplant therapy and resulting oral complications.
- List management strategies and the need for interdisciplinary teamwork when caring for this patient population.
The immune system is made of many cells and proteins that keep our body functions in check and protect against infection. Many of the cells that help create and maintain the immune system are hematopoietic stem cells, or blood-forming stems cells.1 Hematopoietic stems cells can mature into three types of blood cells: white blood cells, which are used to help fight infection; red blood cells, which help carry oxygen throughout the body; and platelets that help the blood clot.1 While most hemopoietic stem cells are found in bone marrow, some are found in the bloodstream and umbilical cord.1 When genetic mutations occur in cases involving primary immunodeficiencies, cancer and other hematopoietic life-threatening diseases, hematopoietic stem cell transplantation (HSCT) is a primary therapy.1
The number of HSCT cases in the United States continues to rise. Approximately 20,000 Americans receive HSCT each year due to the efficacy of this procedure.2 Improvements in prophylaxis, immunosuppressive treatments and supportive care will have contributed to an estimated 242,000 survivors in the U.S. by 2020.2 Many patients who have been diagnosed with lymphomas and leukemias undergo HSCT. According to the Surgeon General’s Report on Oral Health in America 2000,3 it is estimated that more than 4 million patients in the U.S. will develop oral complications associated with HSCT annually.
In preparation for HSCT treatment, patients and providers should be knowledgeable of the processes for pretransplant and posttransplant care. Oral complications, such as oral mucositis (OM), can occur during the conditioning phase prior to HSCT. These are largely due to the toxic inflammatory reaction of exposure to chemotherapeutic agents and/or radiation therapies that are common prior to HSCT.4 Even when HSCT is successful, numerous posttransplant complications can occur, such as graft versus host disease (GVHD). Patients and their families should have a good understanding of adverse events that can occur and treatment options to assist them throughout the pre- and posttransplant processes.
This paper will provide guidance to oral health professionals about HSCT, with a focus on OM and GVHD. A painful and debilitating condition that can have a significant impact on the ability to eat, swallow or have daily interactions, OM severely affects quality of life.4,5 It has been reported to affect 75% to 99% of patients who undergo HSCT.4 The acute form of GVHD is observed in approximately 50% to 70% of all allogeneic transplant recipients.4 Within the first three years posttransplant, the chronic form of GVHD (cGVHD), which targets the skin, eyes and mouth, affects approximately 20% to 50% of the pediatric population, and 60% to 70% of adult patients who have received HSCT.6 As part of a multidisciplinary care team, oral health professionals can play a significant role in managing these conditions.
PRETRANSPLANT CONDITIONING
Careful and consistent medical care helps guide hematopoietic stem cell transplantation. There are many considerations in pretransplant preparation and posttransplant care. The first obstacle for the recipient in preparation for transplantation is “conditioning.” The patient often undergoes chemotherapy and/or radiation treatment to rid the body of its own defense mechanisms and make room for the new immune cells in the bone marrow.1 Conditioning reduces the chance of graft rejection, but leaves the patient susceptible to infection due to a depleted immune defense system.1 Inflammation of the oral mucosa often leads to mucositis, characterized by mucosal ulcerative damage that penetrates the submucosa of the oral cavity and orodigestive tract.7 Factors associated with OM, such as the patient’s age, underlying condition and oral health, have been evaluated in the characterization of OM.8–13 Further considerations associated with the extent and severity of OM include conditioning regimens, transplant type, prophylactic drug therapy and pain management regimens.5,14–16
Severe mucositis is associated with pain, increased bacterial and fungal infections, poor nutrition, salivary dysfunction, caries and other opportunistic infections.8–10 Studies have evaluated the effects of myeloablative and chemotherapeutic conditioning in relation to the severity of OM.5,9,11 Lalla et al16 report practice guidelines for managing OM in their review and update of the Multinational Association of Supportive Care in Cancer and International Society of Oral Oncology using The World Health Organization (WHO) Oral Toxicity Scale for mucositis. This scale focuses on objective signs of OM, such as erythema and ulcer development, and subjective signs, such as the ability to swallow and sensitivity of the mucosa.16 Treister17 recommends use of a companion questionnaire, the Oral Mucositis Daily Questionnaire, which measures mouth and throat soreness and the impact on daily activities. The questionnaire has been validated and correlates with the severity of OM found on the WHO score.18 Thus, it is helpful to use both scales when evaluating patients for OM.
Several preventive protocols have been proposed to minimize the effects of OM.8,10,12,13 Good oral health prior to HSCT and continued oral care protocols (including brushing, interproximal biofilm cleansing, and regular professional oral prophylaxis throughout the transplant process) have shown positive results in multiple studies.8,10,12,13 At least two studies have shown bacterial and fungal shifts in the oral microbiome posttransplant. The increased prevalence of Candida species and anaerobic bacteria may play a role in the severity of OM.12,13
Despite OM’s impact, no gold standard of care exists for preventing this condition. Further research is needed to better understand the trauma associated with mechanistic microbial effects of conditioning regimens and trauma to connective and mucosal tissues. However, current approaches to managing OM include oral debridement, oral decontamination (including antibacterial and antifungal rinses), topical and systemic pain management, cryotherapy, palifermin or keratinocyte growth factor, and low-level laser therapy (i.e., photo biomodulation).17–19
Prior to conditioning, it is advised that patients have a thorough medical history review and screening for possible acute infections. This may include CT scans, MRI and a comprehensive dental exam. Dental imaging, such as panoramic, bitewing and periapical radiographs or cone beam computed tomography, may be completed prior to conditioning and transplantation. Treatment may consist of caries management, extractions and/or prophylaxis. Ideally, dental and transplant teams should work closely in developing a comprehensive course of treatment. The interdisciplinary care team should be mindful of the recipient’s underlying condition and extent of dental treatment that may be required prior to HSCT.20
Yet, controversy exists regarding the extent and type of dental treatment needed in close proximity to conditioning and transplantation. In some cases, the need for transplantation is urgent and there is no time to complete dental treatment prior to conditioning. Clinicians are advised to concentrate primarily on acute needs, including periodontal/periapical pathologies and elimination of bleeding or pain, such as active tooth infection.20
ADDITIONAL COMPLICATIONS
Even when HSCT is successful, numerous posttransplant complications are possible. For example, GVHD can occur post-HSCT if donor-derived immunocompetent cells react against human tissues, inciting an inflammatory response.1,21,22 The oral cavity is one of the most frequently targeted sites of GVHD; therefore, it is important for dental professionals to establish clear communication with the transplant team to coordinate oral care throughout HSCT therapy to minimize discomfort and complications. The most common oral lesions associated with GVHD are lichenoid-hyperkeratotic mucosal changes and mucoceles. Salivary gland dysfunction is also common in HSCT recipients.22 The dental evaluation and treatment plan should be discussed with patients, their families and the interdisciplinary care team.
In some cases, patients are persistently neutropenic, or are required to remain in immunosuppressive therapy for extended periods, and infections are a major concern.20 In addition to these obstacles, GVHD can pose serious complications. A result of the immunocompetent T lymphocytes recognizing the new immune system cells as foreign,21 GVHD remains the leading cause of morbidity and mortality associated with allogeneic HSCT.22 Fatalities related to GHVD are often due to immune dysfunction and immunosuppression, leading to recurring opportunistic infections.22 The acute form of GVHD is observed in approximately 50% to 70% of allogeneic transplant patients,21 and occurs within 100 days of transplantation. It is characterized by damage to the skin and liver, as well as mucositis of the oral cavity and gastrointestinal tract.22 By comparison, cGVHD is characterized by the clinical and histological similarities to autoimmune disorders, such as Sjögren’s syndrome, scleroderma immune cytopenias and chronic immunodeficiencies.23 Among allogeneic transplant recipients, 30% to 50% are affected by cGVHD within three years following HSCT.21
Oral GVHD can present with an array of symptoms that result in significant short- and long-term complications ranging from oral sensitivity to secondary malignancies.23 This condition can also damage the salivary glands. Oral dryness is sometimes underappreciated, as compromised salivary function can lead to caries and risk of secondary fungal infections.23 Many times, patients with GVHD are placed on immunosuppressive medications, increasing the development of oral ulcers. Controlling oral bacterial loads will reduce the chance of oral and/or systemic infection. Oral health professionals are advised to provide individualized, comprehensive instructions to help these patients maintain meticulous self-care regimens at home. Dental recare frequency should be based on clinical symptoms and minimally set at two- to three-month intervals for the year after transplant.
Treatment plans involving HSCT are considered a primary choice for malignant conditions, including leukemias, lymphoma and multiple myeloma. It is important to recognize HSCT as extremely beneficial for treating nonmalignant hematologic disorders, such as aplastic anemia and sickle cell disease, as well as several genetic immunological deficiencies, including chronic granulomatous disease, hyper IgE syndrome, leukocyte adhesion deficiency, Chediak-Higashi syndrome and Papillon-Lefevre syndrome, among others.1,2 When caring for this patient population, it is necessary to obtain and update a thorough medical and medication history at each appointment.

ORAL SCREENING FOR COMPLICATIONS
Common patient-reported symptoms of cGVHD include severe oral dryness, chapped lips, and sensitivity to spicy foods, toothpaste, rinses and carbonated beverages. In addition, cGVHD is an autoimmune disease that will flare with intense oral pain. Evaluation and oral care are largely based on clinical presentation and need for interventional therapy. A primary objective is pain management to reduce and control symptoms; topical corticosteroid therapy, for example, is a common treatment for oral cGVHD.23 Rinses and gels are able to reach areas of the oral cavity that can be difficult to access. While there are few guidelines for medicaments in managing oral ulcers, products used for oral GVHD range from saline rinses, sodium bicarbonate mouthwashes, mixed-medication mouthwashes (such as viscous lidocaine 2%), and nonviscous topical anesthetics. Although there is no substantial evidence to show these medicaments do anything to heal or cure GVHD, patients report they provide short-term pain relief,24 and quality of life and nutritional intake may improve with effective pain relief. Topical corticosteroids, such as dexamethasone solution 0.5 mg/5 ml, are common treatments as swish-and-spit medicaments. In addition, topical betamethasone gel and nystatin rinses can help control the inflammatory effects of cGVHD and fungal infiltrates.25
This patient population should be informed of the importance of oral self-examinations and instructed to report any new or unusual symptoms, such as discoloration of tissue, swelling or pain. Meticulous oral hygiene that includes daily brushing and interproximal biofilm cleansing — along with regular professional prophylaxis — is recommended. Adjunctive therapies, such as fluoride gels or varnishes, might also be prescribed. As noted, patients with oral cGVHD may complain of intense sensitivity to toothpaste, which is usually due to ingredients such as sodium lauryl sulfate or flavoring agents. Toothpastes that lack these ingredients may be warranted. In addition, patients with GVHD and oral sensitivity may find alcohol-free rinses more tolerable than other formulations.
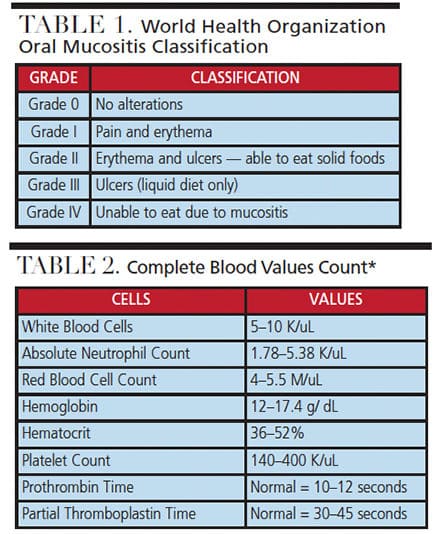
Complete Count and Common Blood Deficiencies. Available at:
https://www.cc.nih.gov/ccc/patient_education/pepubs/cbc.pdf.
Accessed February 15, 2019.
NUTRITIONAL EVALUATION
Nutritional evaluation of transplant patients with cGVHD is important in managing this population. Oral cavity discomfort and other issues, including vomiting, diarrhea, dysphagia, dysgeusia and xerostomia, all play a role in weight loss and malnutrition. Understanding the course of treatment — such as transplant type and graft success — helps clinicians identify the factors associated with malnutrition and quality of life. Foods that are bland and easy to digest may help with discomfort and gastrointestinal healing.26
Gastrointestinal, lung and oral GVHD are associated with weight loss. In addition, Bassim et al26 utilized the patient-generated subjective global assessment questionnaire to assess 210 patients moderately or severely affected by cGVHD. The study revealed oral, lung and gastrointestinal cGVHD were correlated with malnutrition and closely associated with decreased function, reducing the quality of life. These findings may help in developing more accurate interdisciplinary assessments and preventive measures for managing cGVHD.
SECONDARY CANCERS
A study by Hanna et al27 of HSCT posttransplant recipients with cGVHD revealed squamous cell carcinoma of the oral cavity as the most frequent secondary cancer, as these patients face a 16-fold higher risk than the general population. Oral cancer screenings should be a routine part of every dental examination. The oral presentation of GVHD/cGVHD can be complex. Taking photographs of suspicious abnormalities, such as focal masses and nonhealing, deep ulcerations, is useful for documentation during evaluation and follow-up appointments. Being clinically aware of patient behavior and risks for oral cancer can lead to diagnosis of secondary cancers at an early stage for a more favorable prognosis. Educating patients about an effective oral self-examination may prove an important first step in early detection of significant pathology.
CONCLUSION
During the last several decades, HSCT has cured many patients of their underlying hematologic malignancies and other hematologic diseases. To ensure optimal outcomes, it is imperative to adopt a multidisciplinary approach in treating these patients and their complex comorbidities. Among this patient population, systematic treatment planning and multidisciplinary communication, along with frequent dental visits and meticulous oral hygiene, will help in managing OM and GVHD/cGVHD, thus keeping symptoms well controlled and complications minimized.
REFERENCES
- Immune Deficiency Foundation. Organization and development of the immune system. Available at: https:/ / primaryimmune.org/ about-primary-immunodeficiencies/ immune-system-and-primary-immunodeficiency. Accessed February 15, 2019.
- Majhail NS, Tao L, Bredeson C, Davies S, et al. Prevalence of hematopoietic cell transplant survivors in the United States. Biol Blood Marrow Transplant. 2013;19:1498–1501.
- U.S. Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General (2000). Available at: https:/ / profiles.nlm.nih.gov/ ps/ retrieve/ ResourceMetadata/ NNBBJT/ . Accessed February 15, 2019.
- Gabriel DA, Shea T, Olajida O, Serody JS, Comeau T. The effect of oral mucositis on morbidity and mortality in bone marrow transplant. Semin Oncol. 2003; 30(Suppl 18):76–83.
- Pereira NF, Silva PV, Fukuka CY, et al. Measurement of oral health quality of life among patients who underwent haematopoietic stem-cell transplantation. Braz. Oral Res. 2018;32:e78.
- Baird K, Cooke K, Schultz KR. Chronic graft versus host diseases (GVHD) in children. Pediatr Clin North Am. 2010;57:297–322.
- Haverman TM, Rbaer-Durlacher JE, Rademacher W, et al. Oral complications in hematopoietic stem cell recipients: The role of inflammation. Mediators Inflamm. 2014;2014:378281.
- Coracin FL, Santos PS, Gallottini MH, et al. Oral health as a predictive factor for oral mucositis. Clinics. 2013;68:792–796.
- Patussi C, Sassi LM, Munhoz EC, Zanicotti RT, Schussel JL. Clinical assessment of oral mucositis and candidiasis compare to chemotherapic nadir in transplanted patients. Braz Oral Res. 2014;28:1–7.
- Kashiwazaki H, Matsushita T, Sugita J, et al. Professional oral health care reduces oral mucositis and febrile neutropenia in patients treated with allogeneic bone marrow transplantation. Support Care Cancer. 2012;20:367–373.
- McGuire DB, Correa ME, Johnson J, Wienandts P. The role of basic oral care and good clinical practice principles in the management of oral mucositis. Support Care Cancer. 2006;14:541–547.
- Osakabe L, Utsumi A, Saito B, et al. Influence of oral anaerobic bacteria on hematopoietic stem call transplantation patietns: oral mucositis and general condition. Transplantion Proceedings. 2017;49:2176–2182.
- Muro M, Soga Y, Higuchi T, Kataoka K, Ekuni D, Maeda Y. Unusual oral mucosal microbiota after hematopoietic cell transplantation with flycopeptide antibiotics: Potential association with pathophysiology of oral mucositis. Folia Microbiologica. 2018;63:587–597.
- Brennan MT, Hasseus B, Hovan AJ, et al. Impact of oral side effects from condition therapy before hematopoietic stem cell transplantation: Protocol for a multicenter study. JMIR Res Protoc. 2018;7:e103.
- Valeh M, Kargar M, Mansouri A, et, al. Factors affecting the incidence and severity of oral mucositis following hematopoietic stem cell transplantaion. Int J Hematology-Oncolocy Stem Cell Res. 2018;12:142–152.
- Lalla RV, Bowen J, Barasch A, et al. MASCC/ ISSO clinical practice guidelines for the management of mucositis secondary to cancer therapy. Cancer. 2014;120:1453–1461.
- Treister, NS. Chemotherapy-induced oral mucositis. Available at: http:/ / emedicine.medscape.com/ article/ 1079570. Accessed February 15, 2019.
- Stiff PJ, Erder H, Bensinger WI, et al. Reliability and validity of a patient self-administered daily questionnaire to assess impact of oral mucositis (OM) on pain and daily functioning in patients undergoing autologous hematopoietic stem cell transplantation (HSCT). Bone Marrow Transplant. 2006;37:393–401.
- Sonis ST, Oster G, Fuchs H, Bellm L, Bradford WZ, Edelsberg J. Oral mucositis and the clinical and economic outcomes of hematopoietc stem cell transplantation. J Clin Oncology. 2001;9:2201–2205.
- Boguslawska-Kapala A, Halaburda K, Rusyan E, et al. Oral health of adult patients undergoing hematopoietic cell transplantation. Pre-transplant assessment and care. Ann Hematol. 2017;96:1135–1145.
- Margaix-Muñoz M, Bagán JV, Jiménez Y, Sarrión MG, Poveda-Roda R. Graft versus host disease affecting oral cavity. A review. J Clin Exp Dent. 2015;7:138–145.
- Mays J, Fassil H, Edwards D, et al. Oral chronic graft-versus host disease: Current pathogenesis, therapy and research. Oral Diseases.2013;19:327–346.
- Treister N, Duncan C, Culer C, Lehmann L. How we treat oral chronic graft versus-host disease. Blood. 2012;120:3407–3418.
- Meier JK, Wolff D, Pavletic S, et al. Oral chronic graft-versus host disease: Report from the International Consensus Conference on clinical practice in cGVHD. Clin Oral Investig. 2011;15:127–139.
- Stoopler ET. Management of oral chronic graft versus host disease. J Can Dent Assoc. 2013;79:d37.
- Bassim CW, Fassil H, Dobbin M, et al. Malnutrition in patients with chronic GVHD. Bone Marrow Transplant. 2014;49:1300–1306.
- Hanna GJ, Kofman ER, Shazib MA, et al. Integrated genomic characterization of oral carcinomas in post-hematopoietic stem call transplantation survivors. Oral Oncol. 2018;81:1–9.
Featured image by XRENDER/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. March 2019;5(3):30–32,35.

