

Understanding Implant Abutment Connection Interfaces
This site warrants careful consideration when restoring dental implants, as the choice of components can directly impact outcomes.
This site warrants careful consideration when restoring dental implants, as the choice of components can directly impact outcomes
The implant abutment connection interface (IACI) is a key feature to consider when choosing an implant system. It corresponds to the connection site where the implant body connects to the abutment and restoration, so its clinical abilities are vital to successful outcomes, especially as implant failure is now known to be strongly related to how the restorative phase is managed.1 Making the correct decisions when deciding on the IACI can improve esthetics and longevity, and provide for a structurally secure joint. It can also help prevent biological issues, such as peri-implant disease and irreversible implant damage.
Historically, the first IACI was the external hexagon (or hex) configuration introduced by Branemark. This design became the standard for the period, and once it became apparent the external hex could also provide anti-rotational capabilities, the era of the single implant restoration was born. However, the external hex also presents limitations, including issues with micromovement and microgaps developing under lateral loading. This external connection also has a higher center of rotation, which reduces mechanical stability.2 Furthermore, due to masticatory forces and problems with superstructure misfit, screw loosening could be an issue.3
Although the external hex still has a place in implantology, these limitations have led to the development of various IACI connection systems to address these issues. Many contemporary implant systems now have an internal — rather than an external — connection. However, not all internal-connection IACIs are the same. They differ with respect to design features and capability. The consequences of choosing a less-than-ideal interface are mechanical and biological, with potential problems resulting in fatigue failures and/or peri-implantitis.4 Furthermore, some of the latest IACI systems allow for innovative and advanced restorative options.5,6 This article will review the important features of this site and provide information for clinicians who are planning implant-based restorative treatment.
KEY CONSIDERATIONS
When choosing an implant system that provides the most desirable internal IACI features, three essential considerations relate to mechanics, biology and clinical utility. Although described independently, it should be apparent that an intimate relationship exists between these factors.
Mechanics: Important mechanical features include an anti-rotation design for single-unit restorations. This provides the ability to remove the abutment and reattach it in the same position — something that may be required if the implant body must be accessed or the implant restoration needs modification. For example, it has been reported that a large number of open contacts develop between implants and adjacent teeth. The removal and precise replacement of the implant restoration allows for modification to counter this effect.7,8
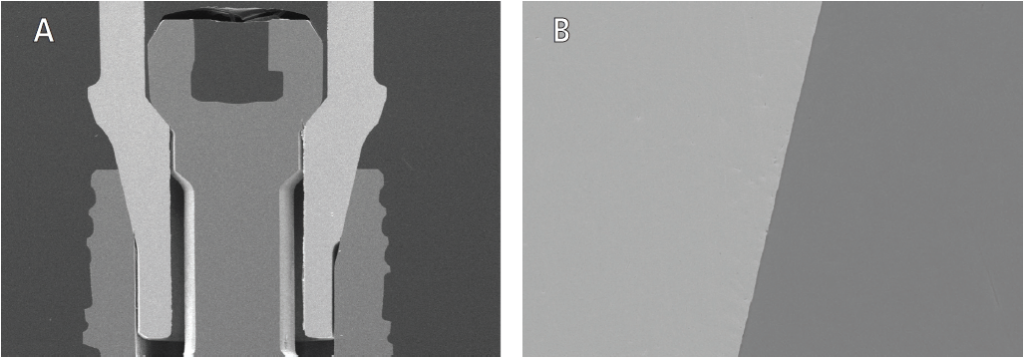
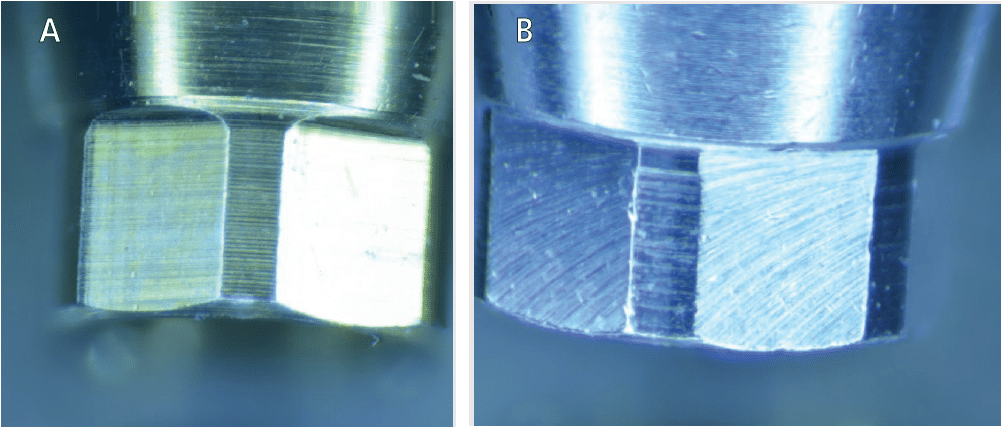
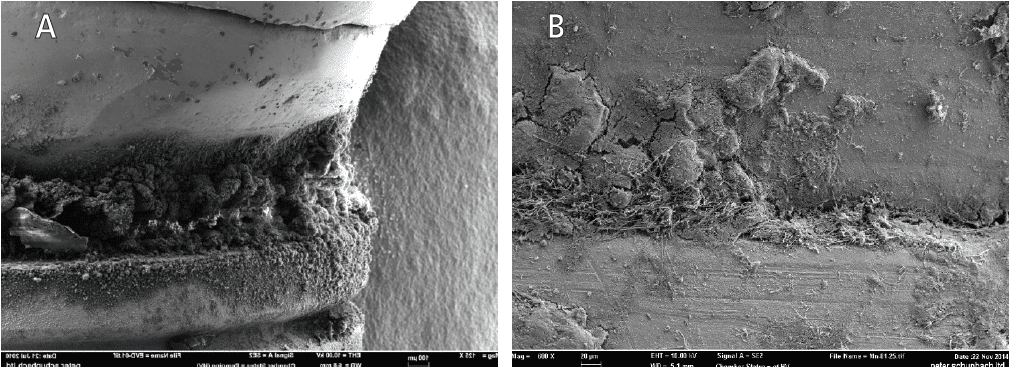
A high quality, intimate union between components in the joint is essential for a tight fit that prevents micromovement of the abutment (Figures 1A and 1B). Any movement between the abutment and implant can be detrimental to the screw, as well as the component gap dimension, further placing the system in jeopardy. Micromovement has been associated with mechanical failure, screw loosening, fracture, and implant and component wear (Figure 2), as well as peri-implant disease.9 Mechanical stress distribution is also vital to maintaining the IACI, as well as protecting the implant from excessive, irregularly distributed forces that can lead to bone loss and implant fracture (Figure 2).
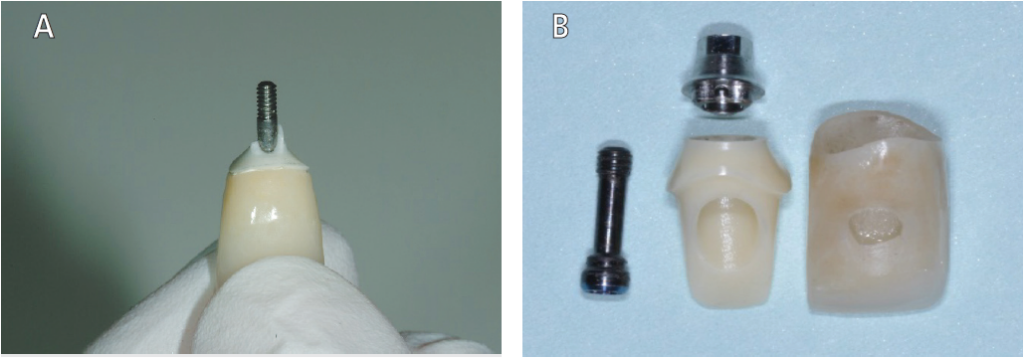
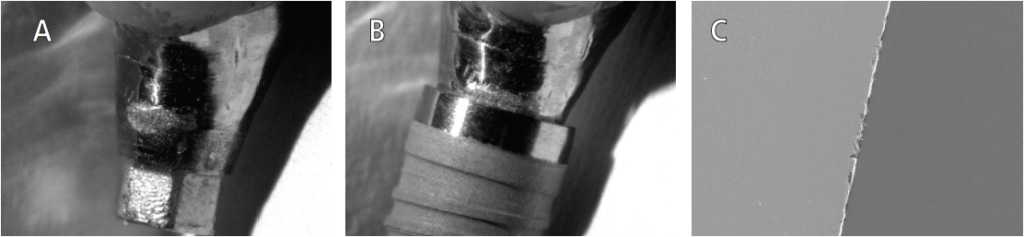
Materials, manufacturing, machining tolerance and quality of the matching parts are all essential to the IACI (Figures 3A and 3B).10 Both micromovements and microgaps are a concern when using damaged (Figures 4A through 4C) or mismatched components (Figures 5A and 5B), in which various parts may be of higher or lower manufacturing standards.11
Biological Considerations: The oral environment is loaded with microbes: some are protective, while others have pathogenic potential. One area that must be considered is microbial contamination of the internal aspect of the implant, where a reservoir of bacteria and yeasts can reside.12 Some IACIs have been shown to significantly limit — and even provide a seal against — bacteria entering the implant (Figure 1). A poor connection clearly would not provide an adequate seal against ingress of bacteria, which, in turn, could lead to peri-implant disease or implant loss (Figures 6A and 6B).
Biocompatibility and material selection also need to be carefully considered. Compared to the use of other materials contacting the peri-implant soft tissues, zirconia and titanium provide excellent biocompatibility and have shown superior biological responses.13 A hybrid design of an abutment containing a titanium base and zirconia provides for excellent mechanics, fit and esthetics (Figure 3B).
Clinical Utility: Platform switching makes use of an internal conical connection to provide a mismatching of a smaller-diameter abutment with the implant platform. When the IACI is coupled with platform switching, studies have shown it can limit stress distribution, resulting in improved marginal bone stability.14 Platform switching also offers the ability to improve esthetics with stabilization of the soft tissues, especially in complex cases in which multiple adjacent implants exist.15
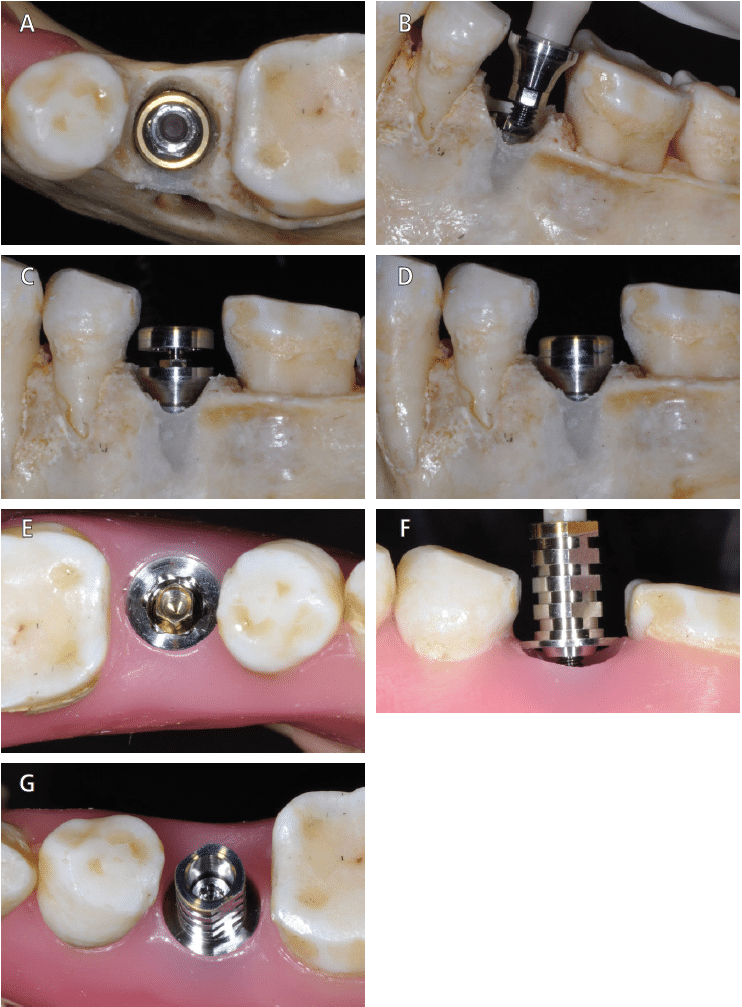
Placing an abutment at the time of surgery (the “one abutment/one time” technique) and maintaining the connection of the IACI has also proven beneficial in maintaining peri-implant tissue stability, limiting bone loss and improving esthetics.5 Some manufacturers have taken advantage of this by introducing innovative designs, such as the On-1 abutment (Nobel Biocare). Designed to be placed at the time of surgery, this two-piece, platform-switched abutment allows for optimizing the biological responses at the IACI by eliminating the need to disturb the soft tissue attachment (Figures 7A through 7G).
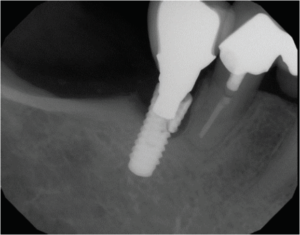
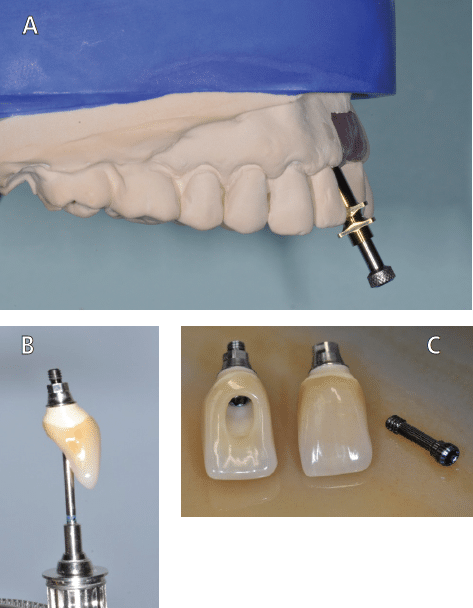
When discussing biological response of the peri-implant tissues, the damage that foreign materials can do is well documented; for example, excess cement has been identified as a cause of implant failure.16,17 However, given implant axial angulation issues — especially in areas of high esthetic concern, such as the anterior maxilla — many implant systems still rely on the use of cemented implant restorations (Figures 8A through 8C, page 34). In these cases, an internal IACI system can be useful alternative to the cemented implant restoration. Requiring no cement, the angulated screw channel (ASC) abutment allows for implant axial inclination changes of up to 25 degrees.6 For example, Nobel Biocare’s ASC combines a tissue-friendly zirconia abutment on a titanium base, both attached through a screw system. Other companies also offer screw channel angulation changing systems, such as Dynamic Abutment Solutions. While this angulated abutment technology provides a choice of compatible components from various companies, clinicians must consider the precision with which the components will ultimately fit.
SUMMARY
Mechanical, biological and design factors will help guide clinicians when choosing an implant system, and the IACI should be considered carefully, as the proper selection of components will help ensure successful outcomes and esthetically pleasing implant restorations.
KEY TAKEAWAYS
- The implant abutment connection interface (IACI) is a key consideration when choosing an implant system.
- The IACI corresponds to the connection site where the implant body connects to the abutment and restoration, so its clinical abilities are vital to successful outcomes.
- When choosing an implant system that provides the most desirable internal IACI features, mechanics and biology are important considerations.
- In implant procedures, materials, manufacturing, machining tolerance and quality of the matching parts are all essential to a clinically acceptable IACI.
Disclosure: Drs. Chandur Wadhwani and Peter Schupbach are consultants for Nobel Biocare.
References
- Pita MS, Anchieta RB, Barao VA, et al. Prosthetic platforms in implant dentistry. J Craniofac Surg. 2011;22:2327–2331.
- Sailer I, Sailer T, Stawarczyk B, Jung R. In vitro study of the influence of the type of connection on the fracture load of zirconia abutments with internal and external implant-abutment connections. Int J Oral Maxillofac Implants. 2009;24:850–858.
- Farina AP, Spazzin AO, Pantoja JM, Consani RL, Mesquita MF. An in vitro comparison of joint stability of implant-supported fixed prosthetic suprastructures retained with different prosthetic screws and levels of fit under masticatory simulation conditions. Int J Oral Maxillofac Implants. 2012;27:833–838.
- Gil FJ, Herrero-Climent M, Lázaro P, Rios JV. Implant-abutment connections: influence of the design on the microgap and their fatigue and fracture behavior of dental implants. J Mater Sci: Mater Med. 2014;25:1825–1830.
- Lazzara RJ, Porter SS. Platform switching: A new concept in implant dentistry for controlling post-restorative bone levels. Int J Periodontics Restorative Dent. 2006;26:9–17.
- Garcia-Gazaui S, Razzoog M, Sierraalta M, Saglik B. Fabrication of a screw-retained restoration avoiding the facial access hole: a clinical report. J Prosthet Dent. 2015;114:621–624.
- Greenstein G, Carpentieri J, Cavallaro J. Open contacts adjacent to dental implant restorations: Etiology, incidence, consequences, and correction. J Am Dent Assoc. 2016;147:28–34.
- Varthis S, Randi A, Tarnow DP. Prevalence of interproximal open contacts between single-implant restorations and adjacent teeth. Int J Oral Maxillofac Implants. 2016;31:1089–1092.
- Liu Y, Wang J. Influences of microgap and micromotion of implant-abutment interface on marginal bone loss around implant neck. Arch Oral Biol. 2017;83:153–160.
- Kelly JR, Rungruanganunt P. Fatigue behavior of computer-aided design/computer-assisted manufacture ceramic abutments as a function of design and ceramics processing. Int J Oral Maxillofac Implants. 2016;31:601–609.
- Hurson S. Use of authentic, integrated dental implant components vital to predictability and successful long-term clinical outcomes. Compend Contin Educ Dent. 2016;37:450–455.
- Baggi L, Di Girolamo M, Mirisola C, Calcaterra R. Microbiological evaluation of bacterial and mycotic seal in implant systems with different implant-abutment interfaces and closing torque values. Implant Dent. 2013;22:344–350.
- Linkevicius T, Vaitelis J. The effect of zirconia or titanium as abutment material on soft peri-implant tissues: a systematic review and meta-analysis. Clin Oral Implants Res. 2015;26 (Suppl 11):139–147.
- Hsu YT, Lin GH, Wang HL. Effects of platform-switching on peri-implant soft and hard tissue outcomes: A systematic review and meta-analysis. Int J Oral Maxillofac Implants. 2017;32:e9–e24.
- Priest GF. The esthetic challenge of adjacent implants. J Oral Maxillofac Surg. 2007;65 (Suppl 1):2–12.
- Wilson TG Jr. The positive relationship between excess cement and peri-implant disease: a prospective clinical endoscopic study. J Periodontol. 2009;80:1388–1392.
- Wadhwani CP, ed. Cementation in Dental Implantology — An Evidence-Based Guide. Heidelberg, Germany: Springer-Verlag Berlin; 2015.
From Decisions in Dentistry. April 2018;4(4):31-34.
