

Dental Screening for Obstructive Sleep Apnea
By adopting in-office screening, oral health professionals can facilitate obstructive sleep apnea diagnosis and treatment.
By adopting in-office screening, oral health professionals can facilitate obstructive sleep apnea diagnosis and treatment
PURCHASE COURSE
This course was published in the November 2018 issue and expires November 2021. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the November 2018 issue and expires November 2021. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the prevalence of obstructive sleep apnea and the dental team’s role in managing this condition.
- List risk factors and comorbidities associated with this disorder.
- Explain assessment tools and treatment options for managing this patient population.
Obstructive sleep apnea is a medical condition receiving escalated attention due to its associated dangers that range from systemic diseases to fatigue-related accidents. Approximately 5.9 million U.S. adults are diagnosed with this condition, whereas an estimated 23.5 million cases remain undiagnosed.1 The latter may be attributed to minimal sleep disorder training across many health care fields.1,2 This public health issue calls for dental professionals to increase their familiarity with obstructive sleep apnea, and implement screening protocols and an interprofessional approach to patient care. Doing so can contribute to early sleep apnea diagnosis and treatment that result in improved health outcomes.
The most common type of sleep apnea, obstructive sleep apnea is characterized by partial or complete narrowing of the pharyngeal airway during sleep.3 It is defined as a condition in which there is a decrease of oxygen intake (hypopnea) or temporary cessation of breathing (apnea).4 This chronic, multifactorial and potentially life-threatening disorder5 is associated with a reduction in oxygen levels, increased carbon dioxide in the bloodstream,4 and numerous medical conditions.6
Due to the frequency with which patients visit oral health care providers, dental teams are on the frontline of disease detection. Information obtained from the medical history, as well as the extraoral and intraoral examination, can reveal obstructive sleep apnea risk factors.7 Assessment can be used to establish a preliminary sleep apnea diagnosis, allowing referral to a medical specialist for definitive diagnosis.
Obstructive sleep apnea increases the risk of morbidity and mortality,6,8 which underscores the need for interprofessional collaboration in diagnosing and managing this condition. Diagnosis and appropriate treatment can also improve coexisting health conditions.
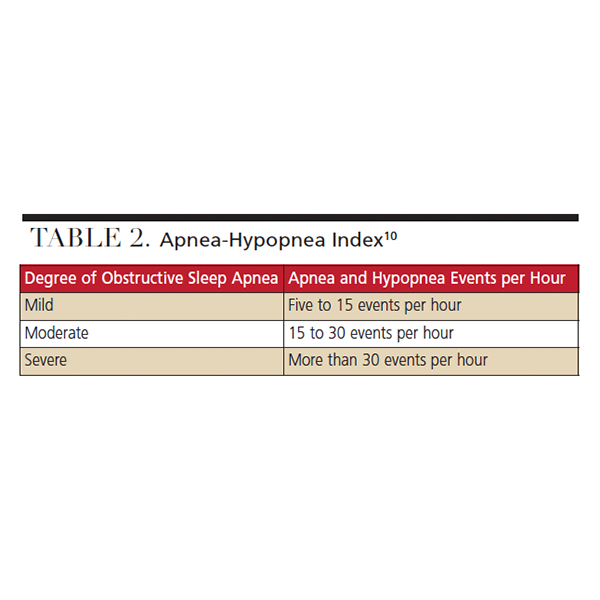
The American Academy of Sleep Medicine developed diagnostic criteria based on reported and observed symptoms, along with polysomnography recordings of hypopnea and apneic episodes.9 Polysomnography is the gold standard for diagnosing this condition,8 and testing occurs at a sleep facility where sleep patterns can be observed. Physiologic data includes the number of apnea and hypopnea events that occur per hour. This is referred to as an apnea-hypopnea index (AHI) that establishes the degree of obstructive sleep apnea: mild (5 ≥ AHI < 15), moderate (15 ≥ AHI < 30), or severe (AHI ≥ 30).10
Obstructive sleep apnea is frequently associated with several comorbidities, such as diabetes mellitus,11 hypertension, cardiovascular disease, cardiac and encephalic alterations,8,11 and periodontitis.12 Affected individuals have higher mortality and medical disabilities.6 In addition to increasing risk for type 2 diabetes, sleep apnea has been linked to insulin resistance and impaired glucose tolerance.13 The American Diabetes Association, International Diabetes Taskforce on Epidemiology and Prevention, and the American Academy of Sleep Medicine recommend routine screening for obstructive sleep apnea within their clinical guidelines for type 2 diabetes.10,13–15
A significant contributor to hypertension, this condition results in airway obstruction, negative intrathoracic pressure swings, and sudden awakening — all of which constrict the peripheral blood vessels, thereby increasing blood pressure.16 Hypertension and untreated obstructive sleep apnea are risk factors for stroke and myocardial infarction.13,17 Research suggests this sleeping disorder has been found in 60% to 80% of post-cerebrovascular events.17 The American Heart Association and American Stroke Association have recognized the significance of a timely obstructive sleep apnea diagnosis, which is reflected in the new guidelines.17
Irregular cardiac rhythms are commonly seen in this patient population; furthermore, it has been reported to be a factor in nocturnal sudden death.6 Neuropsychological dysfunction can also result. Difficulty concentrating, attention deficits, dexterity issues, memory impairment, decreased cognitive processes and reduced visuomotor skills6 can occur, which negatively impact quality of life.
In addition, a correlation between periodontitis and obstructive sleep apnea exists, which is attributed to the elevated inflammatory response associated with each condition.12 The exact etiology of the systemic inflammation that accompanies this sleeping disorder is unclear, but research suggests it may be linked to the oral cavity and periodontal disease.12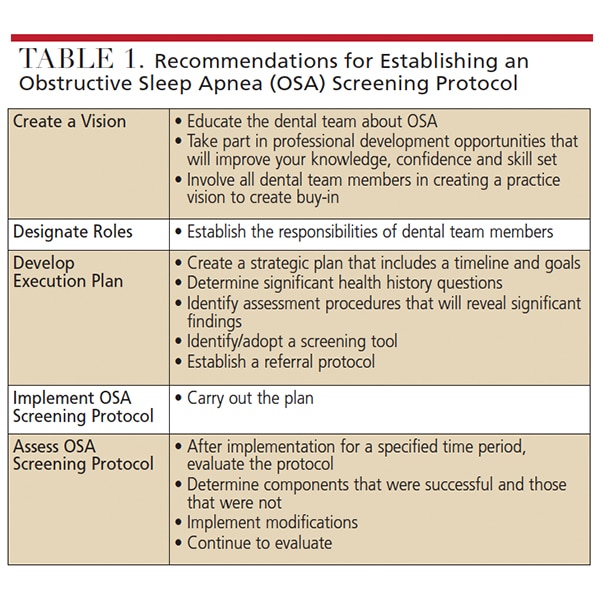
RISK FACTORS
Risk factors include age, obesity, gender, hormones, pregnancy and lifestyle.3,6,7 Prevalence increases with age and plateaus after 60.6 Obesity affects a large number of individuals with obstructive sleep apnea.6 A common characteristic of obesity is excess adipose tissue in the head and neck region that contributes to airway obstruction.6,7
Due to differences in anatomy and physiology, sleep apnea is more common in men than women.6,7 There are also variations in the symptoms experienced by each gender. Lethargy commonly affects women, whereas snoring and apnea episodes are not frequently reported.6 By comparison, affected men often snore loudly and experience cessation of breathing when sleeping. Hormonal changes are associated with prevalence; for example, compared to premenopausal women, a larger number of postmenopausal women have been diagnosed with this condition.6 Postmenopausal women who do not use hormone replacement therapy are at increased risk.18 Pregnant women have increased risk, especially during the third trimester6 when weight gain is greatest. Developing this condition during pregnancy can result in adverse maternal-fetal outcomes, including preeclampsia, intrauterine growth, retardation and low birth weight.19
SYMPTOMS
Symptoms can manifest when the patient is sleeping or awake. Smoking can cause an inflammatory reaction of the pharynx that reduces the airway; similarly, alcohol and sedative use can reduce muscle activity, worsening the symptoms.6 When sleeping, affected individuals may experience nonrestorative sleep6 characterized by feelings of insufficient rest. Individuals experiencing nocturnal symptoms are often unaware of their occurrence. Bed partners frequently report apnea episodes or extreme snoring. Choking, insomnia, restlessness, unsettling dreams, gastroesophogeal reflux (GERD), nocturia, drooling and excess perspiration are also reported symptoms.6
Affected individuals may complain of excessive daytime sleepiness.6 Patients may experience morning headaches,6 irritability20 and depression21 from restlessness and interrupted sleep. Cognitive deficits,6 difficulty focusing20 and xerostomia6 can occur. Experiencing symptoms does not confirm a diagnosis, however. Appropriate testing and medical assessment are required to establish a definitive diagnosis.
CLINICAL FEATURES
Extraoral and intraoral features of the head and neck region may be indicative of obstructive sleep apnea. These clinical presentations can be easily noted during routine assessment. Extraoral findings linked to this disorder include a large neck circumference (> 17 inches for males or > 16 inches for females), as well as what Soo-Lyun and Ransom7 describe as a “small, retrognathic mandible, inferior displacement of the hyoid, increased anterior face height, a steep mandibular plane angle, decrease in nasal patency, and Class II malocclusion.”
Frequent clinical findings include a wide tongue that sits toward the tonsil region7,22 and a narrow, high-vaulted palate.6,7 These anatomical characteristics can reduce the airway passage. A narrow hard palate can decrease nasal airflow.7 Additional intraoral findings include an elongated soft palate and enlarged uvula, tonsils6,23 and adenoids6 — features that can narrow the airway. Erosion attributed to GERD can occur.7 Bruxism and edentulism are also linked to this sleep disorder.7 Affected patients usually grind their teeth and clench their jaw after experiencing an apneic episode.24 Edentulism can cause a reduction of lower face height, anterior rotation of the mandible, and an unnatural position of the tongue — all of which contribute to airway obstruction.25
SCREENING TOOLS
Considering polysomnography is not a feasible option for every patient, clinicians can use various methods to identify patients at risk for obstructive sleep apnea. Easily adopted, these screening tools are simple, effective and provide rapid results. The Berlin questionnaire is composed of three sections assessing snoring, daytime fatigue and sleepiness, as well as medical history and anthropometric measurements.26 The STOP-BANG questionnaire (SBQ) consists of yes-or-no questions.26 The subjective items evaluate snoring, tiredness, observed apnea and blood pressure (hence the acronym STOP).26 The additional items correlate with BANG: body-mass index, age, neck circumference and gender.7 The STOP questionnaire is a more simplified screening instrument, comparable to the SBQ,7,26 and consists of four yes-or-no items correlating to the acronym.
The Sleep Apnea Clinical Score assesses neck circumference, snoring, apnea episodes and hypertension27 to determine the likelihood of obstructive sleep apnea. The Epworth Sleepiness Scale (ESS) assesses daytime sleepiness, a symptom of the disorder. It is composed of a Likert scale in which responses range from zero to three. A total ESS score ≥ 11 suggests excessive daytime sleepiness and high risk.26 The NoSAS score is a quick and efficient way to assesses neck circumference, body mass index, age, sex and snoring28 as they relate to risk for sleep-disordered breathing. The Obstructive Airway Adult Test (OAAT) consists of multiple-choice questions that assess symptoms, apnea episodes, comorbidities and risk factors.8 Scores reflect the degree of obstructive sleep apnea: mild (OAAT score ≥ 38), moderate (score ≥ 57), or severe (score ≥ 73).8 However, additional studies are needed to validate this questionnaire as a screening tool. The American Academy of Sleep Medicine provides self-assessment screening resources.29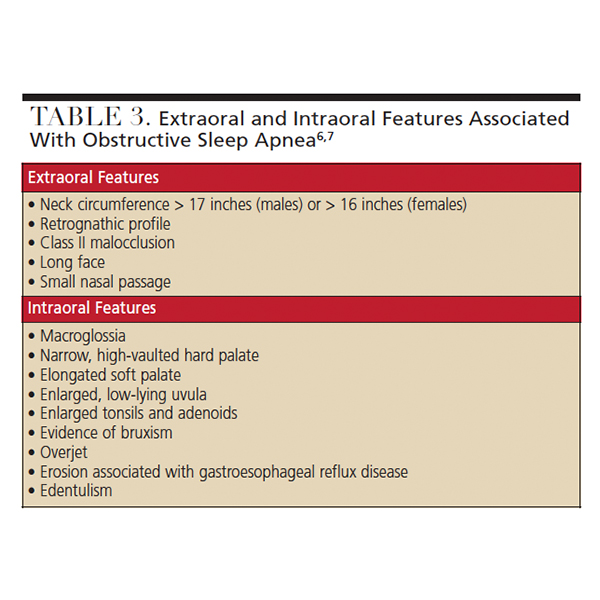
TREATMENT OPTIONS
Obstructive sleep apnea cases vary from patient to patient. After diagnosis, numerous treatment options and lifestyle changes are recommended for patient management, and therapy should be individually tailored. Continuous positive airway pressure (CPAP) is the gold standard for treatment, especially in more severe cases. Use of a CPAP facemask improves quality of life, daytime sleepiness, cognitive function and blood pressure.9 One of the main issues with this treatment is a lack of patient compliance.
Although dentists cannot diagnose obstructive sleep apnea, they can specialize in sleep medicine and play a part in the fabrication of oral appliances to treat the disorder. Oral appliances9 are the treatment option most suitable for mild-to-moderate cases.5 When a patient with a more severe case will not use a CPAP machine, oral appliance therapy can be recommended. Most commonly used are mandibular-repositioning devices designed to hold the mandible in a forward position, enlarge the area posterior to the tongue, and reduce collapse of the pharynx and palate.9 Tongue-retaining devices are splints that hold the tongue in place to maintain an open airway.9
Numerous surgical techniques can be used to treat this patient population, including a variety of upper airway reconstruction or bypass procedures.10 The goal is to remove or bypass the area of upper airway obstruction.6,9 Given the lack of reliable research supporting the outcomes, surgery is a controversial option,9 and is only indicated for patients with severe obstructive sleep apnea who have an anatomic obstruction.9
Myofunctional therapy consists of exercises that target the oral and oropharyngeal structures. It serves as an adjunctive treatment when adhering to the appropriate regimen.30 Research demonstrates that myofunctional therapy reduces AHI levels by approximately 50% in adults and 62% in children.30 Additionally, it improves oxygen saturation, snoring, and the adverse outcomes related to sleepiness.30
Lifestyle modifications are geared toward risk-factor management. Exercise and a healthy diet are encouraged for weight loss; similarly, tobacco cessation and reduced alcohol intake can lessen symptom severity. When the disorder is related to sleep position, positional therapy is recommended to prevent sleeping in a supine position.7,10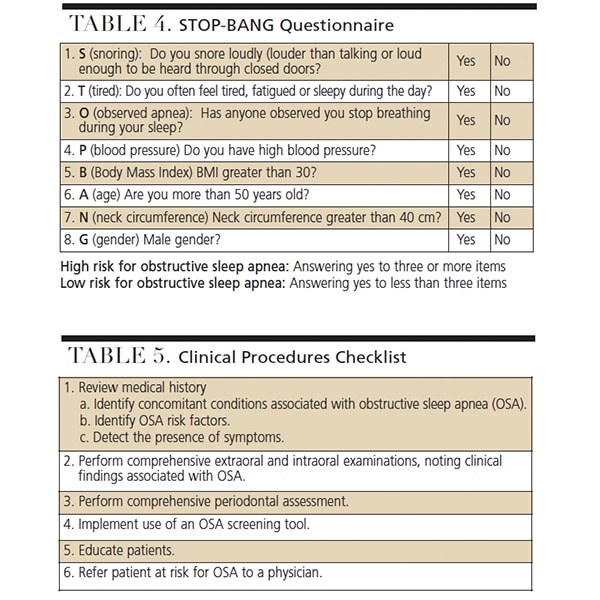
ORAL HEALTH PROFESSIONALS’ ROLE
Oral health professionals are leaders in oral disease detection and prevention. As such, dental teams are encouraged to adopt an appropriate obstructive sleep apnea screening protocol (Table 1). As noted at the outset, research suggests that approximately 80% of individuals with moderate-to-severe obstructive sleep apnea are undiagnosed.26 When a risk assessment is performed and patients are educated about the dangers of this condition, they will be more inclined to seek care.
Performing a comprehensive assessment is key. Reviewing medical histories and asking questions related to risk factors, symptoms and concomitant conditions will help identify patients who may be affected by, or at risk for, obstructive sleep apnea. Performing thorough extraoral and intraoral examinations, and noting any clinical features associated with the disorder, are crucial steps. Clinical signs indicative of parafunctional habits and associated medical conditions should also be documented, as they may be linked to the disorder. Given the correlation between periodontal disease and obstructive sleep apnea, a comprehensive periodontal assessment is needed. Findings from the health history, clinical assessment and screening can help identify patients who should be referred to a physician for further evaluation.
As noted, it is important to educate patients about the health risks, symptoms and treatment options associated with this condition.2,31 Education should also focus on lifestyle modifications, such as smoking cessation and nutritional counseling.
CONCLUSION
Health care providers with diverse areas of expertise should collaborate to identify, educate and treat patients with obstructive sleep apnea.2 An interprofessional approach is required to address disease severity and patient disinclination to follow recommended treatment.2 Oral health professionals should be able to effectively communicate with medical providers about the patient’s risk factors and symptoms. By cultivating an increased understanding of this and other sleep disorders, dental teams can help mitigate issues associated with underdiagnosed and untreated cases. Referrals can lead to a definitive diagnosis, which can improve the management and prognosis of these patients.
In light of the considerable number of undiagnosed cases, oral health professionals can play a significant role in detection and referral. The frequency of dental visits, assessment information obtained, and implementation of screening tools can identify individuals who either have, or are at risk for, obstructive sleep apnea. Educating patients about risk factors, concomitant issues, and treatment options is key to initiating appropriate medical care that will improve quality of life.
REFERENCES
- Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013;177:1006–1014.
- Minichbauer BC, Sheats RD, Wilder RS, Phillips CL, Essick GK. Sleep medicine content in dental hygiene education. J Dent Educ. 2015;79:484–492.
- Kiraç D, Yassa ÖY, Gezmiş H, Domaç SF, Altunok EC, Genç E. The effect of different ApoE genotypes and other risk factors on obstructive sleep apnea syndrome formation. Turk J Neurol. 2017;23:199–204.
- National Institutes of Health U.S. National Library of Medicine. Obstructive sleep apnea. Available at: https://ghr.nlm.nih.gov/condition/obstructive-sleep-apnea#inheritance. Accessed October 15, 2018.
- Maurya R, Singh H, Mishra HA, Gupta A. Modified interim mandibular advancement (MIMA) appliance for symptomatic correction of obstructive sleep apnea. J Clin Diagn Res. 2016;10:ZH01–ZH03.
- Pataka A, Riha RL. The obstructive sleep apnoea/hypopnoea syndrome — An overview. Respir Med CME. 2009;2:111–117.
- Soo-Lyun A, Ranson C. Obstructive sleep apnea for the dental hygienist: overview and parameters for interprofessional practice. Can J Dent Hyg. 2011;45:238–252.
- Gasparini G, Vicini C, De Benedetto M, et al. Diagnostic accuracy of obstructive airway adult test for diagnosis of obstructive sleep apnea. Available at: hindawi.com/journals/bmri/2015/915185/. Accessed October 15, 2018.
- Gutierrez C, Brady P. Obstructive sleep apnea: a diagnostic and treatment guide. J Fam Pract. 2013;62:565–572.
- Epstein LJ, Kristo D, Strollo PJ Jr, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5:263–276.
- Pinto JA, Ribeiro DK, Cavallini AF, Duarte C, Freitas GS. Comorbidities associated with obstructive sleep apnea: a retrospective study. Int Arch Otorhinolaryngol. 2016;20:145–150.
- Famili P. Obstructive sleep apnea and periodontal disease: Review of established relationships and systematic review of the literature. J Dent Oral Health. 2015;1:1–4.
- Shaw JE, Punjabi NM, Wilding JP, Alberti KG, Zimmet PZ, International Diabetes Federation Taskforce on Epidemiology and Prevention. Sleep-disordered breathing and type 2 diabetes: a report from the International Diabetes Federation Taskforce on Epidemiology and Prevention. Diabetes Res Clin Pract. 2008;81:2–12.
- American Diabetes Association. Initial evaluation and diabetes management planning. Diabetes Care. 2015;38(Suppl 1):S17–S19.
- American Academy of Sleep Medicine. Patients with type 2 diabetes or hypertension must be evaluated for sleep apnea. Available at: https://aasm.org/patients-with-type-2-diabetes-or-hypertension-must-be-evaluated-for-sleep-apnea/. Accessed on October 15, 2018.
- Phillips CL, O’Driscoll DM. Hypertension and obstructive sleep apnea. Nat Sci Sleep. 2013;5:43–52.
- Sico JJ, Yaggi HK, Ofner S, et al. Development, validation, and assessment of an ischemic stroke or transient ischemic attack-specific prediction tool for obstructive sleep apnea. J Stroke Cerebrovasc Dis. 2017;26:1745–1754.
- Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med. 2002;165:1217–1239.
- Kapsimalis F, Kryger M. Obstructive sleep apnea in pregnancy. Sleep Med Clin. 2007;2:603–613.
- Qureshi A, Ballard RD. Obstrucive sleep apnea. J Allergy Clin Immunol. 2003;112:643–651.
- Mezick EJ, Hall M, Matthews KA. Are sleep and depression independent or overlapping risk factors for caridometabolic disease? Sleep Med Rev. 2011;15:51–63.
- Kim SW, Kim BY, Han JJ, et al. Major factors affecting severity of obstructive sleep apnea. Indian J Otolaryngol Head Neck Surg. 2015;67(Suppl 1):S114–S118.
- Lim JS, Lee JW, Han C, Kwon JW. Correlation of soft palate length with velum obstruction and severity of obstructive sleep apnea syndrome. Auris Nasus Larynx. 2018;45:499–503.
- Winck M, Drummond M, Viana P, Pinho JC, Winck JC. Sleep bruxism associated with obstructive sleep apnoea syndrome—A pilot study using a new portable device. Rev Port Pneumol (2006). 2017;23:22–26.
- Okşayan R, Sökücü O, Uyar M, Topçuoğlu T. Effects of edentulism in obstructive sleep apnea syndrome. Niger J Clin Prac. 2015;18:502–505.
- Amra B, Rahmati B, Soltaninejad F, Feizi A. Screening questionnaires for obstructive sleep apnea: An updated systematic review. Oman Med J. 2018;33:184–192.
- Ibanez V, Silva J, Cauli O. A survey on sleep questionnaires and diaries. Sleep Med. 2018;42:90–96.
- Marti-Soler H, Hirotsu C, Marques-Vidal P, et al. The NoSAS score for screening of sleep-disordered breathing: a derivation and validation study. Lancet Respir Med. 2016;4:742–748.
- American Academy of Sleep Medicine. Sleep Education Sleep Apnea — Self-Tests. Available at: sleepeducation.org/essentials-in-sleep/sleep-apnea/self-tests. Accessed on October 15, 2018.
- Camacho M, Certal V, Abdullatif J, et al. Myofunctional therapy to treat obstructive sleep apnea: a systematic review and meta-analysis. Sleep. 2015;38:669–675.
- Kornegay EC, Brame JL. Obstructive sleep apnea and the role of dental hygienists. J Dent Hyg. 2015;89:286–292.
Featured image by JUANMONINO/E+/GETTY IMAGES PLUS
From Decisions in Dentistry. November 2018;4(11):38–41.

