

Dental Care for Patients With Special Needs
A basic understanding of the oral health challenges faced by this patient population will allow clinicians to provide effective care.
A basic understanding of the oral health challenges faced by this patient population will allow clinicians to provide effective care
PURCHASE COURSEThis course was published in the September 2016 issue and expires 09/30/19. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Define patients with special needs.
- Identify barriers to dental care faced by the special needs population.
- Discuss treatment and oral hygiene strategies to support the oral health of patients with special needs.
According to the U.S. Census Bureau, in 2010, 56.7 million Americans had a diagnosed disability, which comprises 19% of the noninstitutionalized population.1–6 The Americans with Disabilities Act defines disability as a “physical or mental impairment that substantially limits one or more major life activities,” which may include hearing, vision, communication, mobility, or other activities of daily living. A disability can occur at any age.1,7–12 In 2013, more than half of Americans with disabilities were age 18 to 64; 40% were age 65 and older; 7.4% were children age 5 to 17; and 0.4% were younger than 5.1,2,5,6
Providing dental care to patients with disabilities may require modifications to the traditional treatment plan. Patients with special needs include individuals who are disabled due to physical limitations (congenital, traumatic and/or physiological), medical complications (systemic, acquired and/or hereditary), developmental problems (congenital and/or acquired), and cognitive impairments (mental, sensory, emotional and/or behavioral).8–12 Individuals may present with more than one disability that requires medical management or the use of specialized equipment, services or programs.9,12 Dental health professionals need to be prepared to accommodate patients with special needs, regardless of the type of disability.
Patients with broken or amputated limbs, one or more sensory impairments, or who use wheelchairs may require modifications of the oral health care treatment plan. Individuals with medical conditions, such as cancer, diabetes, respiratory disease, stroke, cardiovascular disease, kidney disease, Parkinson’s disease, multiple sclerosis and other illnesses, may also need specialized support to ensure the dental visit is successful. The presence of developmental conditions, such as Down syndrome, epilepsy, cerebral palsy and muscular dystrophy, as well as cognitive challenges (e.g., autism spectrum disorder, attention deficit hyperactivity disorder or dementia), may also require adjustments to treatment planning. 8,10,11,13
BARRIERS TO CARE FACED BY SPECIAL NEEDS POPULATIONS
Many individuals with disabilities are living longer due to advances in medical treatment. While people with disabilities were often institutionalized in the past, today most reside in communities. This has increased the likelihood that health care providers, including oral health professionals, will treat these patients in traditional medical/dental settings.10 Without access to professional dental care, patients with special needs are at risk of oral disease and a reduced quality of life.3,6,8–10
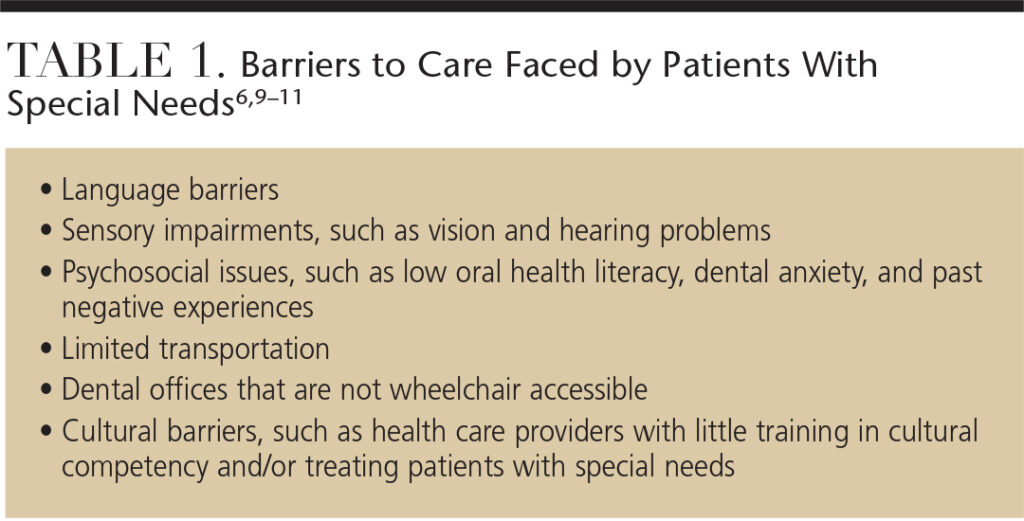
Patients with special needs frequently experience barriers to dental care. The ability to pay for care remains the primary obstacle to obtaining oral health care services for this population.4,6,9–11 Patients with disabilities are often of low socioeconomic status. Many individuals with special needs are without private health insurance and, instead, rely on government programs such as Medicare and Medicaid to pay for their medical and dental care. For those with private insurance, policies may not cover dental care or the cost of modified treatments sometimes required by patients with special needs.8–12 Table 1 lists additional barriers faced by patients with special needs in accessing dental care.6,9–11
STRATEGIES FOR OVERCOMING BARRIERS TO CARE
The addition of education on treating patients with special needs to dental and dental hygiene curriculum is one step toward improving access to care for this patient population. In 2006, for example, the American Dental Association Commission on Dental Accreditation introduced a standard requiring dental hygiene programs to educate students in the treatment of patients with special needs.14 Oral health care teams should embrace an interdisciplinary and interprofessional approach to care when treating this patient cohort.
Legislative reform of private and public reimbursement systems is needed to ensure that dental care for patients with special needs is covered.11,12 This is important because patients with a dental home are more likely to receive appropriate preventive and routine care.8,9,11 Many organizations are working to address barriers to care for these patient populations. These groups include health care professionals who have undergone specialized training on the treatment of patients with special needs.
The Special Care Dentistry Association provides education and networking resources to oral health professionals who serve patients with special needs. Its goal is to increase access to oral health care for special needs populations.15
The National Foundation of Dentistry for the Handicapped is a national organization of volunteer clinicians dedicated to meeting the needs of patients with physical, medical and mental disabilities by providing dental care to those who cannot afford treatment and are not eligible for public aid. Older adults and individuals with disabilities are connected to dentists in their communities who provide comprehensive dental treatment, including prosthetics, at little to no cost. The organization also provides training for parents/caregivers on how to provide appropriate oral hygiene.16
Since 1974, the Dental Education in Care of Persons with Disabilities program at the University of Washington School of Dentistry in Seattle has provided training to oral health professionals on the treatment of special needs populations, in addition to delivering dental care to individuals with disabilities.17 This training program is noteworthy, as most dental and dental hygiene schools have not historically offered such an extensive curriculum aimed at caring for patients with special needs. This lack of training may result in unwillingness to provide treatment to special needs populations. Oral health professionals may be more likely to care for patients with special needs if they receive training early in their academic career and/or when they first begin practicing.17
Established in 1985, Dental Lifeline Network is a national nonprofit organization of volunteer clinicians who provide dental care to older adults, individuals with disabilities, and medically fragile patients who otherwise could not afford care.18
Bridge Campaign of Concern is a dental outreach program in which clinicians, typically dental hygienists, provide preventive services and patient education to individuals with developmental disabilities in schools, vocational centers and group homes. Information from screenings is used to prioritize referrals for treatment and guide staff in providing oral health instruction. The organization operates in both Illinois and Colorado.19
CONSIDERATIONS TO SUPPORT SUCCESSFUL TREATMENT
Before dental treatment can begin, the patient or caregiver must provide informed consent. Clinicians need to provide patients/caregivers with information on all parameters of treatment — including the nature, risk and benefits of the recommended treatment, any evidence-based alternatives to the procedure, an explanation regarding the need for any type of stabilization, and possible complications associated with the proposed treatment — before informed consent can be given.8–11,20
In order to comply with the Americans With Disabilities Act, dental offices must be wheelchair accessible. Some patients with special needs may require transfers from a wheelchair to the dental chair in order to receive treatment.10,11 Patients should be allowed to attempt this transfer by themselves or with assistance from caregivers. Transferring a patient from his or her wheelchair to the dental chair is risky and may result in workplace injury. Modifying the wheelchair to mimic the dental chair or conducting stand-up dental procedures are possibilities when wheelchair transfers are ill advised.
Caregivers are valuable resources when treating patients with special needs because they can provide feedback on the ideal time of day for treatment, behavioral management, communication assistance, insight into treatment needs, and additional information about patients’ disabilities.8,11,12
In addition to obtaining an accurate, comprehensive and current medical history, patient assessment (including range of motion, comprehension level and communication type), and pretreatment planning are essential.8–11 Pretreatment planning should include a thorough review of the patient’s medical history, appropriate intervals for bathroom breaks, completion of forms, discussion of transportation issues, and desensitizing the patient prior to the appointment with a tell-show-do approach aimed at reducing anxiety.8,10,11 The dental team should also coordinate oral care in consultation with patients’ physicians, social workers, nurses and other personnel in order to provide an interdisciplinary approach to comprehensive, safe and effective treatment.8,9,11
Developmentally appropriate communication is critical because patients who are not verbal may communicate in nontraditional ways.9–11 Patients with slight impairments may have increased sensitivity in their other senses.20 Communication in the dental setting is affected by clinicians’ tone of voice, facial expressions and body language. When the clinician’s expression and body language are inconsistent with the intended message, communication may be impaired.11,20 Therefore, dental team members need not only to be attentive to the patient’s body language, but also to their own voices and movements to ensure the messages (verbal or nonverbal) are properly delivered.
Once a patient with special needs is seated securely in his or her wheelchair or the dental chair, the clinician needs to communicate the treatment plan in terms that are appropriate for the patient’s comprehension level. When treating a patient with a hearing impairment, the clinician needs to speak face to face so the patient can read lips.11,21 Some patients may prefer to write messages on a pad of paper or a language board or use sign language.10,11 A patient with a visual impairment may need guidance and verbal directions to experience a successful dental visit. Patients with dental anxiety may fare better with the tell-show-do approach and when provided the opportunity to touch the dental instruments before they are used in their mouths.10,11 Clinicians need to be attentive to the needs of this patient population, beginning with the initial greeting and continuing through the completion of the appointment.
Some patients with special needs have problems with balance, while others may exhibit aggressive behavior. In these cases, supportive and protective stabilization during treatment may be essential to patient comfort and safety during the dental appointment.8,10,11,22 Stabilization of the patient’s head can be accomplished through the use of pillows, rolled blankets or towels. The patient’s head needs to be raised slightly to avoid respiratory compromise.8,10,11,22 During treatment, oral stabilization via mouth props can be achieved with rubber or styrofoam bite blocks (with floss tied through one end to prevent patient aspiration), disposable bite sticks (made of tongue depressors and gauze), cotton rolls and rolled gauze.8,10,11,22
HELPING PATIENTS MAINTAIN EFFECTIVE SELF-CARE

REPRINTED WITH PERMISSION: MANNEN J. ORAL HEALTH AND STROKE. DIMENSIONS OF DENTAL HYGIENE. 2012;10(7):50–55.
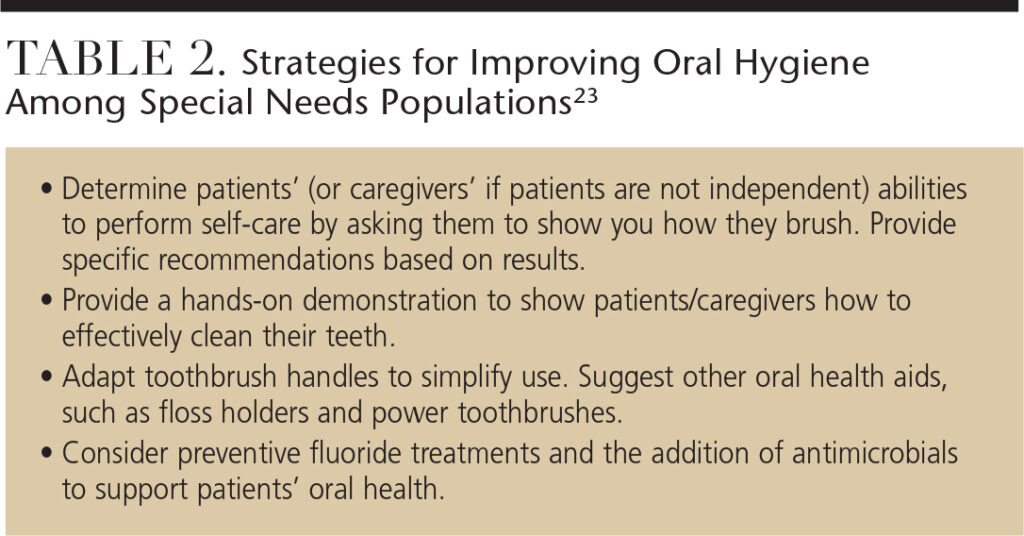
Patients with special needs may exhibit poor oral hygiene due to difficulty in performing self-care and because many take medications that cause negative oral health side effects, such as xerostomia.10,11,22 Clinicians can modify self-care devices to improve the effectiveness of oral hygiene regimens. For patients who have difficulty grasping, the use of a wide-handled power toothbrush is recommended. The addition of bicycle grips, tennis balls or soft plastic to toothbrush handles may also make them easier to hold (Figure 1). An extender (ruler, rod or wooden spoon) can be taped to the handle of a toothbrush to provide assistance for patients with a limited range of motion.10,11,22 Caregivers should also receive patient education on the importance of oral health, the oral/systemic link, optimal nutrition and oral hygiene techniques so they can help patients maintain their oral health. Table 2 provides additional strategies for improving oral hygiene regimens in special needs populations.23
CONCLUSION
Caring for patients with special needs requires pretreatment planning and proper assessment, including scheduling appointments for the appropriate time, performing a thorough medical/dental history in consultation with physicians, social workers and caretakers, and appropriate patient communication. The entire dental team should be educated about how to best care for patients with special needs so the initial impression is an inviting one. Obtaining informed consent and conducting proper documentation are essential prior to treatment. The various treatment modifications for intraoral care can range from pillows and mouth props to toothbrush modifications and stand-up dental treatment. Caregivers, as well as patients, should be educated about nutrition and preventive oral care so that optimal oral health can be achieved and maintained.
References
- U.S. Census Bureau. Americans with Disabilities Act: Population Distribution. Available at: census.gov/newsroom/facts-for-features/2015/cb15-ff10.html. Accessed August 9, 2016.
- Brault MW. Americans with disabilities: 2010. Available at: census.gov/newsroom/cspan/disability/20120726_cspan_disability_slides.pdf. Accessed August 9, 2016.
- Dehaitem MJ, Ridley K, Kerschbaum WE, Inglehart MR, Habil P. Dental hygiene education about patients with special needs: A survey of U.S. programs. J Den Ed. 2008;72:1010–1019.
- Lee HS, Jung HI, Kim SM, Kim J, Doh RE, Lee JH. Attitudes of Korean dental students toward individuals with special health care needs. J Den Ed. 2015;79:1024–1030.
- University of New Hampshire. 2014 Disability Statistics Annual Report. Available at: disabilitycompendium.org/ docs/default-source/2014-compendium/annual-report.pdf. Accessed August 9, 2016.
- World Health Organization. Summary World Report on Disability. Available at: apps.who.int/iris/bitstream/10665/70670/1/WHO_NMH_VIP_11.01_eng.pdf. Accessed August 9, 2016.
- Americans with Disabilities Act. Definition of Disability. Available at: ada.gov/pubs/adastatute08.htm#12102. Accessed August 9, 2016.
- Jaccarino J. General treatment considerations for the patient with special needs. Dent Assist. 2009;78:6–9,34–36.
- American Association of Pediatric Dentistry. Guideline on management of dental patients with special health care needs. Pediatr Dent. 2012;37:166–171.
- Muzzin K. Persons with disabilities. In Darby ML, Walsh MM, eds. Dental Hygiene Theory and Practice. 4th ed. St. Louis: Elsevier Saunders; 2015:786–804.
- Wilkins EM. Patients with special needs. In: Clinical Practice of the Dental Hygienist. 11th ed. Philadelphia: Lippincott Williams & Wilkins; 2013:742–1056.
- DiMatteo AM. Serving patients with special needs. Inside Dentistry. 2009;5(2).
- Szarejko MJ. Dental care for special needs patients. Available at: netce.com/ coursecontent.php?courseid=1316&scrollTo=BEGIN. Accessed August 9, 2016.
- Commission on Dental Accreditation. Accreditation Standards for Dental Hygiene Education Programs. Available at: ada.org/~/media/CODA/Files/ 2016_dh.ashx. Accessed August 9, 2016.
- Special Care Dentistry Association. Definition. Available at: scdaonline.org/. Accessed August 9, 2016.
- National Foundation of Dentistry for the Handicapped. Definition. Available at: 1800dentist.com/national-foundation-of-dentistry-for-handicapped/. Accessed August 9, 2016.
- Dental Education in Care of Persons with Disabilities. Definition. Available at: astdd.org/bestpractices/DES54005WAspecialneedsdecod.pdf. Accessed August 9, 2016.
- Dental Lifeline Network. Definition. Available at: dentallifeline.org/about-us/our-programs/. Accessed August 9, 2016.
- Bridge Campaign of Concern. Definition. Available at: dentallifeline.org/ about-us/our-programs/#HouseCalls. Accessed August 9, 2016.
- American Association of Pediatric Dentistry. Guideline on behavior guidance for the pediatric dental patient. Pediatr Dent. 2011;36:179–191.
- Kibbler B. Are my directions user-friendly? Access. August 2015:41–47.
- Jaccarino J. Helping the special needs patient maintain oral health. Dent Assist. 2009;78:11,12,14,34.
- National Institute of Dental and Craniofacial Research. Practice Oral Care for People With Developmental Disabilities. Available at: nidcr.nih.gov/ oralhealth/Topics/DevelopmentalDisabilities/ContinuingEducation.htm. Accessed August 9, 2016.
From Decisions in Dentistry. September 2016;2(09):50–53.


[…] my career as a dentist, patient care was my favorite part of the job. When providing dental care to patients with special needs, it may require that you modify your traditional treatment […]
[…] to 64; 40% were age 65 and older; 7.4% were children age 5 to 17; and 0.4% were younger than 5” (Decision Dentistry). These staggering statistics bring to light a major need in our health care system that is sadly […]