
Clinical Presentation of Behçet’s Disease
Featuring oral symptoms similar to herpes simplex virus Type 1 and aphthous ulcer, Behçet’s disease may initially be detected by oral health professionals.
Featuring oral symptoms similar to herpes simplex virus Type 1 and aphthous ulcer, Behçet’s disease may initially be detected by oral health professionals
Increasingly, clinicians understand that careful examination of the oral cavity may reveal findings indicative of an underlying systemic condition. Early diagnosis facilitates timely treatment, and thus improves expected health outcomes. Dental professionals may be the first providers to recognize the oral features of systemic diseases. Common in many parts of the world, Behçet’s disease (BD) or Behçet’s syndrome, for example, is a distinct disorder with oral symptoms similar to those seen in herpes simplex virus Type 1 (HSV-1) and aphthous ulcer. The following discussion will offer a brief history of BD, as well as mechanisms to distinguish its oral symptoms from those of HSV-1 and aphthous ulcers.
BEHÇET’S DISEASE
This is a chronic, systemic, autoimmune inflammatory disease that affects several body systems and may be fatal.1 While uncommon in the United States, BD is very common in other nations, specifically in Asia (Japan and Korea), the Mediterranean basin (including Turkey, where it is most prevalent), and Middle Eastern countries.2 In 1937, Turkish physician Hulusi Behçet described the cardinal signs of the disease: oral and genital ulcerations, hypopyon uveitis, and inflammation and pus in the uvea of the eye (which includes the iris, choroid and ciliary body).3 Other symptoms may include arthritis, blood clots, and inflammation in the central nervous system, digestive organs and joints. Although BD affects men and women, is usually more severe in men;2 children and older adults can also develop the condition. The etiology is unknown, but genetic and environmental factors, working in concert, contribute to the pathogenesis of BD. Recent advances have allowed researchers to identify putative genes (HLA-B51) associated with the disease.4 Research on viruses and bacteria suggests that microorganisms may play a role, and Behçet himself suspected a virus may be responsible. Anti-HSV-1 serum antibodies have been found in a higher proportion of individuals with BD, and parvovirus B19 IgG antibodies were detected in 82.5% of patients with BD.5
Host genetic factors play a pivotal role in determining susceptibility to BD,1 but there are no specific tests to confirm a diagnosis.1,6–8 A pathergy test (in which a small, sterile needle is inserted into the skin of the forearm) is sometimes performed. A positive result is noted if a small, red bump or pustule forms at the site in one to two days. However, reactivity varies greatly among populations, and the test’s sensitivity has declined over the years.7 A diagnosis of BD is made on the basis of the presentation of several symptoms and, until 2006, relied on criteria created by a collection of scientists from seven countries known as the International Study Group. Evaluation of the group’s criteria revealed shortcomings, however: The patient populations were selected from seven countries and were limited, and oral aphthosis was a mandatory requirement — even though this symptom was not seen in a significant percentage of patients diagnosed with BD. Consequently, the necessity of a more comprehensive approach to diagnosis became obvious.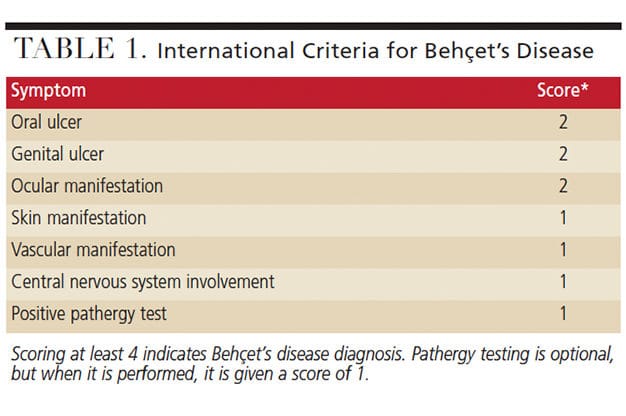
In 2006, the International Criteria for Behçet’s Disease was developed by researchers from 27 countries and included data from 2556 clinically diagnosed BD patients and 1163 controls. The authors’ consensus statement promulgated use of a weighted point value system that assigned a numerical value to each symptom. It also expanded the criteria to include six symptoms and an optional pathergy test.7 As noted in Table 1, a patient scoring higher than 4 is diagnosed with BD (Figure 1 and Figure 2).

disease 4). GWEN COHEN BROWN, DDS, FAAOMP, New York city college of technology

disease 8). GWEN COHEN BROWN, DDS, FAAOMP, New York city college of technology
Oral ulcers are the most common lesions of this disease, and are seen in 97% of patients with BD.9 Individual sores or ulcers are usually identical to canker sores, which are common in many people; with BD, however, the lesions are more numerous, more frequent, and often larger and more painful.
Genital ulcers are seen in approximately 75% of patients with BD. Lesions affect the vulva, vagina and cervix in women, and the scrotum and shaft of the penis in men.10
Eye involvement affects nearly 50% of patients with BD. Unless treated, recurrent attacks of panuveitis and retinitis can result in irreversible damage and vision loss.8
Skin lesions of BD appear red and raised, or as bruises or pus-filled bumps that leave faint scars or discolorations; some may develop eruptions that resemble acne.11
The short- and long-term outcomes of patients with BD depend on the patient’s gender, age at disease onset and disease duration. The two main goals in management are to prevent damage caused by repeated exacerbations of inflammation in major organs, such as the eyes, vascular system, central nervous system and gastrointestinal system, and to prevent skin, mucosa and joint lesions.7,8 While the latter do not cause life-threatening or serious damage, they negatively affect quality of life. Rheumatologists often provide care for patients with BD, but other providers — such as gynecologists, ophthalmologists and dentists — are crucial to treating system-specific symptoms, which can be controlled with palliative medication (such as corticosteroids, TNF inhibitors, cyclosporine and colchicine), a healthy diet, rest and exercise.12
APHTHOUS ULCER
Recurrent aphthous ulcers (RAU) or recurrent aphthous stomatitis (RAS) are commonly known by the general population as canker sores. They are clearly defined, shallow, round or oval lesions with a shallow necrotic center covered with a yellow-grayish pseudomembrane and surrounded by erythematous halos.9 Most patients have one to three ulcers present at any one time. The lesions are painful and affect a patient’s ability to eat, swallow and speak. Onset is usually during childhood and 80% of patients with RAS develop the condition prior to age 30. According to Scully et al,6 manifestation after the age of 30 “suggests a possibility… that the ulceration is not simple RAS, but, rather, part of a more complex disorder, such as BD.” Diagnosis is based on history and clinical criteria, and no laboratory procedures exist to confirm the diagnosis. Research indicates RAS is recurring and not contagious or precancerous. In most cases, no additional body systems are affected, and patients are otherwise healthy. Aphthous ulcers are classified as minor, major or herpetiform.
Minor aphthous ulcers (aka minor apthae, Mikulicz’s aphthae or mild aphthous ulcers): The most common type of aphthous ulcer occurring in 75% to 85% of all cases of RAS, these usually appear on the labial and buccal mucosa, the floor of the mouth, and the ventral or lateral surface of the tongue. They are less than 10 mm in diameter.6,13
Major aphthous ulcers (aka major apthae, periadenitis mucosa necrotica recurrens or Sutton’s disease): These ulcers are greater than 10 mm in size, are usually deeper than minor apthae, and take longer to heal (Figure 3). Typically appearing on the lips, soft palate and throat, they account for 10% to 15% of all RAS cases.6,13
Herpetiform ulcers: Similar in appearance to herpetic lesions (hence, the name), HSV cannot be isolated from them. This is a rare form of aphthous ulcer, seen only in 5% to 10% of RAS cases (Figure 4). They appear as multiple clusters of small, round ulcers (as many as 100), and are seen anywhere on the mucosa. The small clusters may merge and form one larger lesion. They occur more often in women and have an older age of onset.6,13

patient with human immunodeficiency virus.
GWEN COHEN BROWN, DDS, FAAOMP

While the etiology is unknown, there appears to be a genetic component, as an individual who experiences RAS often has either one or both parents also experiencing the condition. The pathogenesis involves a predominantly cell-mediated immune response in which tumor necrosis factor α (TNF α) plays a significant role.13 Various factors thought to provoke immunological responses include:
- Trauma: Although the exact mechanism is unknown, trauma — such as anesthetic injections, sharp foods, toothbrushing and dental treatment — can trigger aphthous ulcerations.4
- Stress: Everyday stress contributes to inflammation by releasing the hormone cortisol. When cortisol is depleted, the natural immune response becomes less effective. The pathways by which the steady infusion of cortisol facilitates chronic inflammation are complex, but it is thought that cortisol inhibits the production of immunoglobulin A (IgA), immunoglobulin G and neutrophil function.14 Immunoglobulins are protein molecules produced by special cells of the immune system that neutralize pathogens by enhancing bacterial phagocytosis and limiting microbial adherence and penetration into the mucosa.15,16 IgA is the predominant immunoglobulin found in saliva and constitutes a first line of defense against pathogens.15
- Food and food allergy sensitivities: Cow’s milk, gluten, chocolate, nuts, cheese, azo dyes (food coloring dyes), flavoring agents and preservatives have all been implicated in exacerbating RAS.13
- Hormonal imbalance: Studies suggest oral ulceration may be related to the onset of menstruation or the luteal phase of the menstrual cycle.13
- Tobacco smoking: For some time, researchers have noted decreased prevalence of RAS among smokers. While the exact mechanism is unknown, hypotheses for this finding include mechanical and chemical barrier formation due to increased keratinization of the oral mucosa. Others have suggested nicotine’s ability to reduce production of TNF α and interleukins 1 and 6 (immunologic response agents that are thought to induce the epithelial damage seen in RAU) by inducing the production of adrenal steroids.
- Systemic conditions and diseases: These include a variety of gastrointestinal diseases, such as Crohn’s disease, ulcerative colitis and Celiac disease.
HERPES SIMPLEX VIRUS
Exposure to HSV presents in biphasic pattern, most commonly occurring in early childhood. Most patients exposed to the virus do not develop primary herpetic gingivostomatitis, and less than 10% develop a primary clinical infection. Up to 90% have a subacute infection without clinical presentation of disease. In either situation, following exposure, the virion travels to either the trigeminal root ganglion or cervical ganglia, where it remains dormant until it is reactivated. Although the trigger is unknown, animal models are being tested to determine etiology of reactivation of the herpes virus in the ganglion.17 The most common secondary manifestation of HSV infection is herpes labialis. Recurrent herpes may present intraorally, as well, affecting only the attached, nonmovable keratinized mucosa, such as the attached alveolar mucosa or hard palate (Figure 5).18 Symptoms of HSV-1 include painful sores that appear on the oral and labial mucosa, herpetic whitlow, herpes ocular infections and keratitis.19,20 Infected individuals often experience a tingling, itching or burning sensation (prodrome) before sores appear, which will typically resolve within seven to 14 days. Infection is lifelong, with periods of eruption coinciding with emotional stress, illness, sunlight, menstruation and physical trauma.21 The frequency of recurrences varies, as humoral and cellular immune responses regulate reactivation.5 Extremely common, HSV-1 occurs in 67% of the global population22 and in approximately 80% of the U.S. population.23

Lesions appear as fluid-filled vesicles that rupture and produce a painful area of ulceration. The exudate is highly infectious at this stage, containing up to 1 million viral particles per ml.20 Within a few days, the ulcer dries up, leaving a scab that is much less infectious. Eventually, the area heals, leaving newly formed tissue. A definitive diagnosis of HSV-1 requires a virus culture, blood test or biopsy. However, most oral health professionals diagnose the condition based on history and visual inspection of the lesions. Lesions have been effectively treated with acyclovir and penciclovir.21 However, the emergence of drug-resistant viral isolates, combined with the potential for toxicity with overuse (in immunocompromised populations), has led to the creation of new antiherpetic medications with different mechanisms of action.18
CONCLUSION
Globalization has introduced new challenges to health care providers. Dentists who serve populations that are continually diversifying should be cognizant of disorders prevalent in other countries that may produce oral pathology. Only a biopsy can provide a definitive diagnosis of an oral lesion. However, conducting a thorough health history review prior to performing a comprehensive clinical examination will provide information vital to an accurate diagnosis. Such an exploration would allow clinicians to differentiate between common oral lesions, such as HSV-1 and RAS, and the lesions seen in BD, a systemic disease that requires interprofessional collaboration to properly treat.
KEY TAKEAWAYS
- Oral health professionals may be the first providers to recognize the oral features of Behçet’s disease (BD), a potentially fatal disorder that is common in many parts of the world.
- Dentists who serve populations that are continually diversifying should be cognizant of disorders prevalent in other countries that may produce oral pathology.
- A chronic, systemic, autoimmune inflammatory condition, BD presents with symptoms similar to those seen in herpes simplex virus Type 1 and aphthous ulcer, making early
diagnosis key to timely treatment. - Working in concert, genetic and environmental factors contribute to the pathogenesis of BD.
- A patient scoring higher than 4 on the International Criteria for Behçet’s Disease is diagnosed with BD (Table 1).
REFERENCES
- Oğuz AK, Yılmaz ST, Oygür ÇŞ, et al. Behçet’s: a disease or a syndrome? Answer from an expression profiling study. PLoS One. 2016;11e0149052.
- Pineton de Chambrun M, Wechsler B, Geri G, Cacoub P, Saadoun D. New insights into the pathogenesis of Behçet’s disease. Autoimmun Rev. 2012;11:687–698.
- Saylan T. Life story of Dr. Hulusi Behçet. Yonsei Med J. 1997;38:327–332.
- Hatemi G, Yazici H. Behçet’s syndrome and micro-organisms. Best Pract Res Clin Rheumatol. 2011;25:389–406.
- Kapsimali VD, Kanakis MA, Vaiopoulos GA, Kaklamanis PG. Etiopathogenesis of Behçet’s disease with emphasis on the role of immunological aberrations. Clin Rheumatol. 2010;29:1211–1216.
- Scully C, Gorsky M, Lozada-Nur F. The diagnosis and management of recurrent aphthous stomatitis: a consensus approach. J Am Dent Assoc. 2003;134:200–207.
- Kronborg C, Mahar PD, Kelly R. Should we keep changing the diagnostic criteria for Behçet’s disease? Dermatology. 2014;228:1–4.
- Rhee SH, Kim YB, Lee ES. Comparison of Behçet’s disease and recurrent aphthous ulcer according to characteristics of gastrointestinal symptoms. J Korean Med Sci. 2005;20:971–976.
- Taylor J, Glenny AM, Walsh T, et al. Interventions for the management of oral ulcers in Behçet’s disease. Cochrane Database Syst Rev. 2014;9:CD011018.
- American Behçet’s Disease Association. Signs and Symptoms. Available at: www.behcets.com/site/c.8oIJJRPsGcISF/b.9145375/k.E8A8/Symptoms.htm. Accessed June 14, 2018.
- U.S. Department of Health and Human Services. Behçet disease. Available at: https://rarediseases.info.nih.gov/diseases/848/behcet-disease. Accessed June 14, 2018.
- American Behçet’s Disease Association. Diagnosis. Available at: www.behcets.com/site/c.8oIJJRPsGcISF/b.9145377/k.ED52/Diagnosis.htm. Accessed June 14, 2018.
- Natah SS, Konttinen YT, Enattah NS, Ashammakhi N, Sharkey K, Häyrinen-Immonen R. Recurrent aphthous ulcers today: a review of the growing knowledge. Int J Oral Maxillofac Surg. 2004;33:221–234.
- Rosania AE, Low KG, McCormick CM, Rosania DA. Stress, depression, cortisol, and periodontal disease. J Periodontol. 2009;80:260–266.
- Giuca MR, Pasini M, Tecco S, Giuca G, Marzo G. Levels of salivary immunoglobulins and periodontal evaluation in smoking patients. BMC Immunol. 2014;15:5.
- Srinivasan PC. Immunoglobulin levels and periodontal diseases-a clinical immunological study. Open Access Scientific Reports. 2012;4:1–4.
- Kollias, CM, Huneke RB, Wigdahl B, Jennings SR. Animal models of herpes simplex virus immunity and pathogenesis. J Neurovirol. 2015;21:8–23.
- Vadlapudi AD, Vadlapatla RK, Mitra AK. Update on emerging antivirals for the management of herpes simplex virus infections: a patenting perspective. Recent Pat Antiinfect Drug Discov. 2013;8:55–67.
- Stanfield B, Kousoulas KG. Herpes simplex vaccines: prospects of live-attenuated HSV vaccines to combat genital and ocular infections. Curr Clin Microbiol Rep. 2015;2:125–136.
- Lewis MA. Herpes simplex virus: an occupational hazard in dentistry. Int Dent J. 2004;54:103–111.
- Femiamo F, Gombos F, Scully C. Recurrent herpes labialis: efficacy of topical therapy with penciclovir compared with acyclovir (aciclovir). Oral Dis. 2001;7:31–33.
- World Health Organization. Herpes simplex virus. Available at: www.who.int/mediacentre/factsheets/fs400/en/. Accessed June 14, 2018.
- Johns Hopkins Medicine. Oral herpes. Available at: www.hopkinsmedicine.org/healthlibrary/conditions/adult/infectious_diseases/Oral_Herpes_22,OralHerpes. Accessed June 14, 2018.
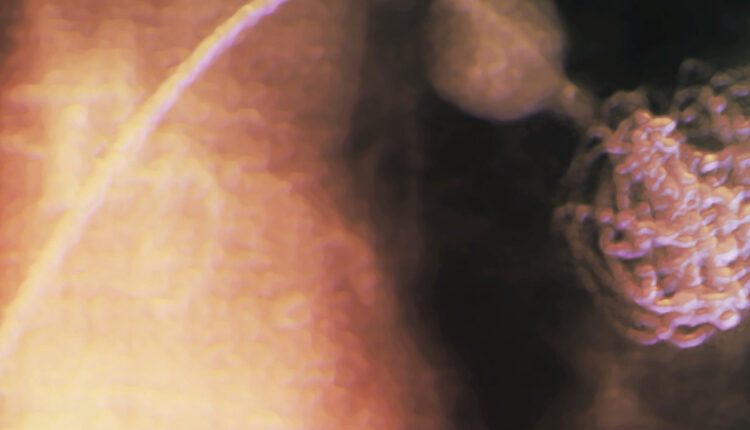
Colored radiograph of a 49-year-old patient with Behçet’s disease, showing a catheter inserting a coil into an aneurysm of a pulmonary artery in the lung. Endovascular coiling initiates a clotting reaction that helps eliminate the aneurysm. Featured Image by ZEPHYR/SCIENCE PHOTO LIBRARY
From Decisions in Dentistry. July 2018;4(7):19-22.
