
Applications for Facial Injectables In Dentistry
As the field of esthetic facial injectables continues to grow, dentists interested in expanding their practice will benefit from this systematic approach to evidence-based treatment.
As the field of esthetic facial injectables continues to grow, dentists interested in expanding their practice will benefit from this systematic approach to evidence-based treatment
PURCHASE COURSE
This course was published in the March 2019 issue and expires March 2022. The author reports she holds stock in Allergan plc. This 2 credit hour self-study activity is electronically mediated.
This course was published in the March 2019 issue and expires March 2022. The author reports she holds stock in Allergan plc. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss dentists’ qualifications for performing facial injectable therapy, and the importance of staying abreast of the latest evidence-based approaches to cosmetic treatment.
- Explain clinical strategies for patient assessment, communication, treatment planning and therapy in this field.
- Describe the specialized knowledge and training required to provide this form of treatment.
Dentists are de facto specialists in the head and neck area, with a rich education in cephalometry and facial esthetics. The field of facial injectables is a natural appendix to the existing scope of practice and continues its expansion in dental offices across the country. Each state decides its own position on cosmetic injectables, and readers are cautioned to consult state dental boards for current rules. As this area of practice evolves, the importance of continuing education in this young field cannot be overstated. Evolution in the understanding and scientific basis of what causes facial aging is generating rapid change, with techniques and standards for injectable therapy sometimes becoming obsolete within a year.
As a result, dentists can unknowingly trap themselves in outdated techniques. For example, the once state-of-the-art approach of “following the wrinkle” will certainly now fail to realize the full benefits of facial injectables. The goal of this article is to provide summary information on the most current treatment approach in cosmetic injectables. A case presentation will serve as a practical demonstration.
Facial aging is a universal human experience. Yet despite its universality, or perhaps because of it, most clinicians spend little time considering how it occurs. However, for practitioners dedicated to treating the aging face, its study is both fascinating and clinically important. In addition to a thorough understanding of facial anatomy and the biochemistry of products used, successful injectable treatment requires comprehensive knowledge of the process of facial senescence.
Knowing where to look for signs of aging requires special training. Humans view the face in a holistic fashion and not as separate units — meaning, facial components are not assessed independently.1 Proficiency in the art of facial rejuvenation requires practitioners to view the face in its totality and determine which units evoke the impression of senescence. Because innate brain biology directs humans to read faces much like a scanner reads a barcode, this skill must be learned and refined.
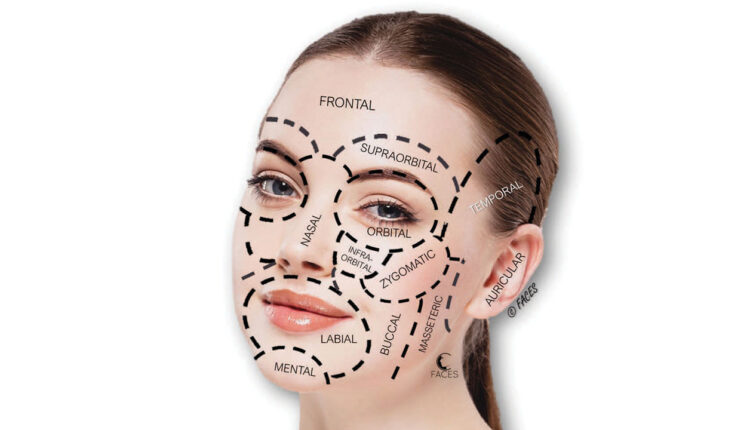
Signs of facial aging result from changes in the soft tissue envelope, as well as the underlying skeletal framework.2 Study in this area led to the description of facial esthetic units (anatomic areas of similar characteristics that can be distinguished from other areas) by Gonzalez-Ulloa and Flores3 in 1965. For assessment purposes, the six major units of the face (forehead, eyes/eyebrows, cheeks, chin, lips and nose) can be further divided into subunits (Figure 1) that serve as a useful construct when training the eye to evaluate facial esthetics.

HOW THE FACE AGES
These esthetic units join seamlessly in young individuals, as the full contours blend without interruption — with little or no shadowing between them. Facial fat exists in discrete compartments and not simply as one large amorphous sheet.4 As a person ages, folds and hollows emerge at transition points between fat compartments, with esthetic units gradually becoming more distinct. Moreover, these units may not age at the same rate; differences in tissue thickness, bony support and facial ligamentous attachments are likely drivers of such disparate changes. Given the lack of uniformity in aging, a universal template for rejuvenation is untenable. Diagnosing a patient’s unique facial aging etiology requires systematic evaluation of each esthetic unit. This provides the basis for a rational approach to facial rejuvenation and prevents constriction of focus. Moreover, site-specific changes of individual esthetic units lend themselves to the targeted approach afforded by facial injectables.
Factors influencing the signs of aging are intrinsic or extrinsic. Intrinsic factors are genetically determined and include cell apoptosis and inherent events that result in changes in skin elasticity and collagen, as well as fat distribution. Extrinsic factors are considered lifestyle and environmental in origin, and include sun exposure, hydration, nutrition, smoking and alcohol use. It has been estimated that up to 90% of visible skin aging stems from sun exposure.5
NOT ALL WRINKLES ARE EQUAL
In the context of skin, so-called “wrinkles” (rhytids) can have multiple causes. Based on their etiology, rhytids can be categorized as superficial, hyperdynamic or volume deficit (Figure 2).

Superficial wrinkles remain visible even when the face is in repose. These are largely attributable to photoaging from the sun (actinic elastosis). Chronic sun damage affects all dermal layers and cell types, and can produce multiple changes in the skin, especially in individuals of fair complexion. Besides wrinkles, sun damage can produce unevenness in skin color, spider veins, raised and exophytic lesions, and skin cancers.6
Hyperdynamic wrinkles are produced during facial animation. With repeated facial expression, fixed lines and creases begin to appear. Common areas include horizontal forehead lines and the “11s” that appear between the eyebrows (glabella). These are due to extrinsic insults to the skin (e.g., sun and smoking) and biological aging of skin cells. With age, epidermal cell turnover begins to slow, affecting repair and function. Additionally, cellular metabolism results in a buildup of reactive oxygen species, which, over time, causes damage to essential cellular components, such as enzymes and deoxyribonucleic acid (or DNA).7
Estrogens play a dominant role in male and female skin health and directly impact skin thickness, repair and healing. Their presence can delay the visible signs of aging.8 The dermis is considered a stratified endocrine organ and can synthesize hormones by itself.9 Hormonal changes in postmenopausal women accelerate the skin changes associated with aging. As a consequence, women frequently present for facial rejuvenation soon after menopause has started. Manifestations of decreased estrogen include thinner, less elastic skin, more numerous and deeper facial wrinkles, and increased dryness.
Volume deficits are the result of fat loss and redistribution. These changes create distinct folds and troughs, and are compounded by remodeling of the facial skeleton. The once-popular theory of gravitational facial aging — the belief that vertical decent of facial soft tissue is attributed solely to age-related elastosis and attenuation of the ligaments anchoring the skin to the underlying fibro-osseous structure — has been largely supplanted by volumetric theory.10 Seminal work by Donofrio,11 Lambros,12 and Rohrich and Pessa13 refocused attention on facial fat, ultimately demonstrating via photographic longitudinal studies and cadaver research concomitant gains and losses in superficial and deep fat compartments, as well as segmentation within each fat layer.
FACIAL REJUVENATION GOALS
Progressive distortions in the three-dimensional topography of underlying structures, as well as superficial skin changes, create what is recognized as facial aging. The goals of facial rejuvenation are to decrease visible transitions between facial esthetic units, diminish or eliminate senescent changes in skin tone and texture, and resuspend ptotic tissue. Because facial injectables cannot successfully treat every type of defect, selection of the optimal treatment modality depends on the presenting problem(s). The current array of cosmetic injectables can affect dynamic rhytids (neuromodulation), volume deficits (soft tissue fillers), and selective volume excesses (deoxycholic acids).
Clearly, practitioners must possess the skills to perform any procedure they elect to offer; these are acquired by attending certification courses, workshops and hand-on training. In addition to anatomy, high-quality training includes identification and management of all potential adverse events (including rare complications), proper photo-documentation and informed consent. If correction of a patient’s chief complaint requires a treatment modality outside of the practitioner’s area of expertise, a suitable referral should be provided.
SEEING THE UNSEEN
Patients are often motivated to seek treatment after seeing advertisements and marketing claims. This information is usually incomplete and generates a narrow focus on U.S. Food and Drug Administration-approved areas, such as nasolabial folds and crow’s feet. Most patients have limited medical knowledge and cosmetic injectable information presented by the lay media can be confusing and misleading. Responsibility rests with the provider to educate and fully inform the patient.
Seasoned practitioners know that a “problem” visible in one area may be a downstream effect of the true etiology from an adjacent area. Once the patient’s area(s) of concern is/are understood, the provider should start with a full-face assessment. A systematic evaluation creates a balanced perspective that is less reliant on patient bias. Knowledge of facial aging and the structural reasons for changes provides a rubric for assessment and treatment planning. With this in mind, the dentist should evaluate facial esthetic units, discern where those units may have become distinct, and thereby determine their effects on the whole. If treatment of an adjacent area is deemed necessary to meaningfully correct the patients’ chief complaint, the rationale must be clearly explained.
CONSULTATION PEARLS AND PITFALLS
The consultation is a forum for essential information for the practitioner and patient. In facial injection therapy, dentists must determine a patient’s chief complaint, expectations, motivations and suitability for treatment. The patient should understand treatment options, expected outcomes and, when indicated, given an appropriate specialty referral.
When discussing esthetic injections with patients, questions should be encouraged and all conversations should be in laymen’s terms, as medical jargon can be intimidating and confusing. Moreover, in situations in which information asymmetry exists (when one person has better information than the other), the professional relationship can degrade quickly, often leaving the patient with the impression of being upsold. The essential ingredient of trust dissolves when the patient believes the practitioner is merely attempting to increase the bottom line. This underscores the importance of being able to communicate — and, when possible, demonstrate — the interdependence of facial units, and how an area of patient concern is affected by adjacent structures.
The importance of elucidating a patient’s area of concern cannot be overstated. Miscommunication in this area is not uncommon and warrants any time necessary to provide clarity. Treatment satisfaction is primarily determined by understanding a patient’s desires, and practitioners are cautioned not to assume they know what a patient wants. To that end, the merits of a complete facial evaluation should be explained. This also ensures that nothing is overlooked (as previously noted, facial areas are interconnected and problems appearing in one area may be the result of a defect in an adjacent area).
CASE PRESENTATION: PATIENT EVALUATION

The patient presented with specific concerns about her lower face and marionette lines (Figure 3). A pan-facial esthetic evaluation revealed the following: beginning with the skin, signs of actinic damage were apparent, including elastosis, unevenness of skin tone and freckling. Years of hyperdynamic muscular movement had produced etched lines on her forehead, periocular and perioral areas. From an esthetic unit perspective and looking more critically at her ocular components, her brow position appeared low, she had mild lateral canthal droop, as well as under-eye hollows. The patient’s nose was unremarkable with the exception of skin changes already mentioned and some light horizontal banding at the radix related to procerus muscle contraction. Her cheeks exhibited mild fat atrophy and ptosis, which was evident in the loss of anterior projection (malar flattening). As the patient observed, her perioral area showed conspicuous signs of aging. This included radial lip lines, moderate lip volume loss, philtral column effacement, marionette lines, downturned oral commissures, deepened perimental hollows, and prejowl sulci (with resulting loss of jawline definition). Her nasolabial folds were mild in depth. Due to volume losses, her under-eye hollows, marionette lines and pre-jowl sulci created abrupt and noticeable transitions between esthetic units.
PATIENT EDUCATION
From an injectable standpoint, optimal treatment for this patient would include a combination of neuromodulators and soft tissue fillers. The patient’s assessment of her lower face proved accurate. The perioral unit was a dominant contributor to her facial senescence; however, her periocular components were also a factor. Once it was determined injectables could improve her lower face (the patient’s chief complaint), treatment options were outlined. If injectables were not appropriate, however, the patient would have been referred to a specialist for consultation.
TREATMENT OPTIONS
Clinically, it is helpful to discuss treatment in front of a mirror. Starting the conversation by pointing out areas that do not require treatment can set a positive tone and put the patient at ease. Next, the conversation should address the patient’s chief complaint. In this case, a cotton tip applicator was used to point to her perioral areas while explaining how soft tissue filler can treat the volume losses, and how small amounts of neuromodulator can soften the radial lip lines. It is equally important to disclose treatment limitations. For example, this patient was told her solar elastosis (superficial skin wrinkling) could not be addressed with injectables. Neuromodulators decrease muscular contraction and dermal fillers replace lost volume, but neither can treat superficial skin rhytids that result from extrinsic insults to the dermis. These areas would be amenable to a laser or chemical peel.
Encouraging questions helps bring the patient into the dialogue; this ensures the patient understands the process and is clear on expected outcomes. Taking the time to discuss these themes during the consultation will often decrease the time needed on the day of treatment when the patient is giving informed consent. It also allows assessment of the patient’s psychological state with respect to treatment motivation and outcome expectations.
At this point (and in a clinically compassionate way), the periocular components that contribute to the patient’s facial aging should be discussed, and the patient made aware of any areas that will require further attention at the time of her choosing. An astute practitioner will sense if the patient is receptive to this information, and proceed accordingly.
READING THE PATIENT
This patient was new to facial injectables. During the consultation, she was interested in addressing her chief complaint, but appeared cautious when discussing areas beyond her primary concern. Therefore, the focus remained exclusively on her perioral area. The benefits of combined neuromodulator and soft tissue filler effects were explained. The conversation revealed the patient was psychologically balanced and had reasonable expectations of results. Thus, she was deemed an excellent candidate for treatment.
Despite the patient’s reluctance to address the periocular area at this time, the expected improvement in her lower face would likely enhance her overall facial appearance. Moreover, once treatment was complete, the patient would have a better understanding of achievable results. She would know what to expect regarding the level of procedure discomfort and any postoperative downtime. Armed with this information, patients are generally more accepting and motivated to pursue additional injectable treatments.
Figure 4 shows the patient’s pretreatment and immediate-postoperative photos. The oral commissures and prejowl sulci were treated with a 30-gauge needle. A blunt-end microcannula was used in the remaining areas, and 3 cc of dermal filler was used to complete the case. Besides increased patient comfort, the blunt-end microcannula does not require nerve block anesthesia — and the lack of tissue trauma with the microcannula is evident with the absence of bruising in the postoperative photo. In addition to dermal filler, the patient received small doses of onabotulinumtoxinA in her mentalis and each depressor anguli oris muscle. Final photographs were taken, postoperative instructions issued, and the patient was scheduled for a follow-up appointment in two weeks.

SUMMARY
As with all therapies, successful outcomes rely on an accurate diagnosis, selection of the appropriate treatment modality (or modalities), and a skilled practitioner. It is also important to ensure patients have realistic expectations. In contrast to traditional medical treatments that measure success by mortality and morbidity, successful facial injectable therapy is primarily determined by patient satisfaction. Therefore, understanding the factors influencing this measure is one of the most important ingredients in a successful esthetic practice.
The days of line-and-wrinkle chasing are over. Patients have many choices when selecting an esthetic practitioner. Consistent delivery of excellence with cosmetic facial injectables demands that dentists continue to learn and stay abreast of state-of-the-art, evidence-based treatment. This includes training the esthetic eye to correctly identify areas of the face that convey the impression of senescence. Moreover, a systematic approach to examination — which ultimately guides correct diagnosis and decision-making — will help ensure successful outcomes and overall patient satisfaction.
REFERENCES
- Tsao DY, Livingstone MS. Mechanisms of face perception. Annu Rev Neurosci. 2008;31:411–437.
- Mendelson B, Wong CH. Changes in the facial skeleton with aging: Implications and clinical applications in facial rejuvenation. Aesthetic Plast Surg. 2012;36:753–760.
- Gonzalez-Ulloa M, Flores ES. Senility of the face — Basic study to understand its causes and effects. Plast Reconstr Surg. 1965;36:239–246.
- Rohrich RJ, Pessa JE. The fat compartments of the face: Anatomy and clinical implications for cosmetic surgery. Plast Reconstr Surg. 2007;119:2219–2227, discussion 2228–2231.
- Terrence C. Keaney, MD. Aging in the male face: Intrinsic and extrinsic factors. Dermatol Surg. 2016;42:797–803.
- Bilaç C, Şahin MT, Ozturcan S. Chronic actinic damage of facial skin. Clin Dermatol.2014;32:752–762.
- Farage MA, Miller KW, Elsner P, Maibach HI. Characteristics of the aging skin. Adv Wound Care (New Rochelle). 2013;2:5–10.
- Stevenson S, Thornton J. Effect of estrogens on skin aging and the potential role of SERMs. Clin Interv Aging. 2007;2:283–297.
- Markiewicz E, Idowu OC. Involvement of the nuclear structural proteins in aging-related responses of human skin to the environmental stress. Clin Cosmet Investig Dermatol. 2018;11:297–307.
- Wan D, Amirlak B, Rohrich R, Davis K. The clinical importance of the fat compartments in midfacial aging. Plast Reconstr Surg Glob Open. 2014;1:e92.
- Donofrio LM. Fat distribution: a morphologic study of the aging face. Dermatol Surg. 2000;26:1107–1112.
- Lambros V. Observations on periorbital and midface aging. Plast Reconstr Surg. 2007;120:1367–1376, discussion 1377.
- Rohrich RJ, Pessa JE. The fat compartments of the face: Anatomy and clinical implications for cosmetic surgery. Plast Reconstr Surg. 2007;119:2219–2227, discussion 2228–2231.
From Decisions in Dentistry. March 2019;5(3):40–43.

