

Alveolar Ridge and Socket Preservation Techniques for Implant Therapy
An examination of the significance of alveolar ridge and socket preservation in implant therapy.
An examination of the significance of alveolar ridge and socket preservation in implant therapy

Maintaining optimal alveolar ridge dimension and socket preservation following tooth extraction are key goals in implant therapy. Once the tooth is extracted, hard and soft tissue remodeling is part of the normal physiologic healing process that occurs to the remaining edentulous ridge. This remodeling negatively affects the ridge dimensions in the buccolingual and apicocoronal aspects. For premolar and molar sites, Schropp et al1 report ridge width reductions up to 50% (an average loss of 6.1 mm) within the first year post-extraction. With respect to anterior and premolar sites, a systematic review described an average loss of 3.87 mm in ridge width, and 1.67 to 2.03 mm in ridge height.2 Considering these ridge alterations may hinder optimal implant placement, compromise esthetics, and create unfavorable defects around neighboring teeth and prostheses, minimizing this bone-resorptive process has been extensively researched. For clinicians, the goal is to provide treatment that preserves the natural tissue contours of the ridge following tooth extraction.

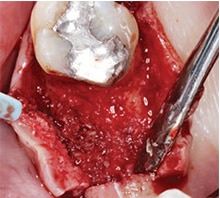
clinical image.

atraumatic extraction, the socket was grafted with allograft particles.
Alveolar socket preservation has been used to describe “a technique in which completely contained extraction sockets are filled with a bone substitute material and/or sealed with membranes, whereas in alveolar ridge preservation, damaged extraction sockets are also included.”3 Conversely, some review articles consider the terms interchangeable and mainly use alveolar ridge preservation, which has been described as “any procedure developed to eliminate or limit the negative effect of postextraction resorption, maintain the soft and hard tissue contour of the ridge, promote bone formation within the socket, and facilitate implant placement in a prosthetically driven position.”4 The term alveolar ridge preservation will be used throughout this article, and the reviewed literature will involve intact or mild-to-moderately damaged extraction sockets, rather than severely compromised sockets. This paper will also present a visual clinical comparison of two socket preservation cases (Case 1: Figures 1 through 11B; and Case 2: Figures 12 through 22B).

Ridge preservation is indicated in situations in which immediate or early implant placement is not possible due to patient- or site-specific reasons.5 In these scenarios, the main significance of ridge preservation lies within limiting alveolar ridge contraction over the healing period. A systematic review by Avila-Ortiz et al6 reports alveolar ridge preservation was effective with a clinical magnitude of 1.89 mm in terms of buccolingual width, and 2.07 mm for midbuccal height. Maintaining adequate ridge dimensions may help achieve prosthetically driven implant therapy, while avoiding or minimizing the need for additional ridge augmentation at the time of implant placement. A systematic review by Weng et al7 notes “the need for hard tissue augmentation at implant placement was five times higher if no socket preservation/ridge preservation was performed on the day of tooth extraction.” This agrees with a more recent systematic review by Mardas et al8 noting that in comparison with unassisted socket healing, alveolar ridge preservation procedures significantly decrease the need for further ridge augmentation during implant placement.
PRESERVATION TECHNIQUES
It is established that tooth extraction is a traumatic procedure causing severance of the soft tissue and periodontal ligament attachment, along with disruption of vascular structures within the socket walls.9 Therefore, the first critical step is the use of minimally invasive techniques and instruments — such as tooth sectioning, periotomes and vertical extraction systems10 — to prevent additional trauma during extraction (particularly fractures and expansion of socket walls). Following extraction, ridge preservation techniques can be divided into the surgical aspect and material selection aspect.



Surgical Considerations: These mainly relate to the extent of soft tissue manipulation surrounding the extracted tooth. A flapless approach generally means no soft tissue manipulation or only limited undermining was performed to allow for extension of the barrier material under the tissues beyond the defect, and no primary closure was attempted. In comparison, a flapped approach usually involves vertical-releasing incisions, flap reflection and coronal advancement to achieve primary closure.11,12 Studies report mixed results when comparing flap and flapless approaches in alveolar ridge preservation; some authors describe more pronounced ridge resorption when flap reflection is performed to achieve primary closure,12 while others note no significant difference between the two approaches.13,14 However, one of these studies found significantly higher postoperative discomfort associated with the flapped group, and a more coronally displaced mucogingival junction as a result of the associated tissue release for primary closure.13 Additional studies also report no major adverse outcomes and favorable ridge preservation results, despite the fact no primary closure was attempted and treated sockets were left exposed to the oral cavity.15–17

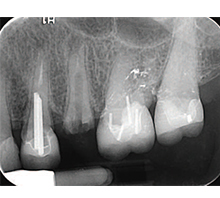
postoperative visit revealed
favorable healing of the
edentulous ridge, with adequate
keratinized tissue.
adequate ridge dimensions for
implant placement, without the
need for further augmentation.

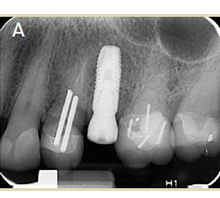
placement was performed and
resorbable, chromic gut
sutures were used to
approximate tissues.

immediately following implant
placement.
Material Selection: Alveolar ridge preservation procedures have been extensively tested with numerous materials and combination of materials, such as:
- Bone grafting alone (including autografts, allografts, xenografts and alloplasts)
- Membrane alone (including resorbable or nonresorbable)
- Combinations of membrane and bone grafting



BONE GRAFTS
Although autografts were considered the gold standard for augmentation procedures, an animal study was conducted to evaluate its efficiency in ridge preservation. The researchers compared autogenous bone chips to anorganic bovine bone and, after three months of healing, significantly more resorption was noted in the autogenous group. The authors attribute this to rapid resorption associated with autogenous bone, which was demonstrated by minimal remaining autogenous chips in the histologic analysis.18 On the other hand, two of the most commonly used grafting materials for alveolar ridge preservation are allografts and xenografts, which were recently compared in a human study that revealed no significant differences in vertical and horizontal dimensional changes after six months of healing.19 With regard to allografts, they are available in mineralized and demineralized forms, and studies comparing the two in ridge preservation have not found one superior to the other.20 Finally, alloplasts — such as hydroxyapatite, tricalcium phosphate, calcium sulfate and bioactive glass polymers — are common examples discussed in the literature. These grafts have shown mixed results in studies, with some authors noting favorable ridge preservation abilities,21 while others report inferior outcomes.22
BARRIER MEMBRANES AND SOCKET SEALING
Clinicians can choose between resorbable and nonresorbable membranes, and both types have been extensively discussed in the literature. Lekovic and colleagues23,24 published some of the earlier studies on the use of membranes alone for ridge preservation. When compared to unassisted socket healing, they found less bone resorption when resorbable or nonresorbable membranes were used. That noted, the use of membranes alone is not widely discussed in the current literature because the focus has chiefly centered on combination approaches in which a graft acts as a socket filler, and either a membrane or socket seal is used to cover the material.


atraumatic extraction,
the socket was grafted
with allograft particles.


When used in combination with bone grafts, resorbable15,19 and nonresorbable16,25 membranes have shown positive results in ridge preservation. With regard to the use of socket sealers in conjunction with bone grafts, a recent study compared four groups: bovine graft with soft tissue punch (from the palate); bovine graft without soft tissue punch; bovine graft with absorbable collagen membrane; and unassisted socket healing as a control. The researchers reported significantly less ridge width loss with the soft tissue punch and membrane groups, as compared to the other two.26 It is generally accepted that covering the underlying bone graft is beneficial. In fact, studies have shown favorable ridge preservation by simply covering the graft material with various collagen wound dressing materials (either tape or plugs).20,27–31


favorable healing of the
edentulous ridge, with
adequate keratinized tissue.

reveals adequate ridge
dimensions for implant
placement, without the need for further augmentation.

placement was performed and resorbable, chromic gut
sutures were used to
approximate tissues.
CONCLUSION
It is accepted that ridge preservation procedures are beneficial in limiting alveolar bone resorption following tooth extraction. The buccal plate is usually thin in nonmolar sites,32,33 and when its thickness is < 2 mm, ridge dimensions are more prone to resorption33 — thus, some form of alveolar ridge preservation is advised. Although ridge preservation may not be advisable in molar sites with a thick buccal plate,34 studies have reported that sinus pneumatization may occur, especially after extraction of second maxillary molars.35 One study showed alveolar ridge preservation in the posterior maxilla may reduce the need for sinus augmentation for implant placement.36 In addition, as noted earlier, alveolar ridge preservation has generally reduced the need for further augmentation at the time of implant placement.7,8


In situations in which immediate or early implant placement is not possible due to patient- or site-specific reasons, alveolar ridge preservation is indicated.5 However, the 2012 Osteology Consensus Conference37 and recent systematic reviews3,38 have not demonstrated clear superiority regarding technique or choice of biomaterials. With respect to the surgical aspect, it seems prudent to choose a ridge preservation technique that involves the least tissue manipulation and surgical trauma, as this will speed healing, while minimizing patient discomfort and postoperative complications. Even so, flap elevation may still be justified for adequate tooth removal and extraction site management.34

In terms of material selection, operators may choose from biomaterials that have been well documented in the literature, taking into account handling characteristics, as well as clinician and patient preference. Ultimately, the choice of technique and material is based on the individual patient and specific clinical situation.
KEY TAKEAWAYS
- The clinical goal in implant therapy involving tooth extraction is to provide treatment that preserves the natural tissue contours of the alveolar ridge, as alterations may hinder optimal implant placement.
- The chief significance of ridge preservation is to limit alveolar ridge contraction over the healing period.
- Compared to unassisted socket healing, alveolar ridge preservation procedures significantly decrease the need for further ridge augmentation during implant placement.
- When used in combination with bone grafts, resorbable15,19 and nonresorbable16,25 membranes have shown positive results in ridge preservation.
- Recent systematic reviews3,38 have not demonstrated clear superiority regarding a specific technique or choice of biomaterials.
REFERENCES
- Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent. 2003;23:313–323.
- Van der Weijden F, Dell’Acqua F, Slot DE. Alveolar bone dimensional changes of post-extraction sockets in humans: a systematic review. J Clin Periodontol. 2009;36:1048–1058.
- Willenbacher M, Al-Nawas B, Berres M, Kämmerer PW, Schiegnitz E. The effects of alveolar ridge preservation: a meta-analysis. Clin Implant Dent Relat Res. 2016;18:1248–1268.
- Horváth A, Mardas N, Mezzomo LA, Needleman IG, Donos N. Alveolar ridge preservation. A systematic review. Clin Oral Investig. 2013;17:341–363.
- Chappuis V, Araújo MG, Buser D. Clinical relevance of dimensional bone and soft tissue alterations post‐extraction in esthetic sites. Periodontol 2000. 2017;73:73–83.
- Avila-Ortiz G, Elangovan S, Kramer KW, Blanchette D, Dawson DV. Effect of alveolar ridge preservation after tooth extraction: a systematic review and meta-analysis. J Dent Res. 2014;93:950–958.
- Weng D, Stock V, Schliephake H. Are socket and ridge preservation techniques at the day of tooth extraction efficient in maintaining the tissues of the alveolar ridge? Systematic review, consensus statements and recommendations of the 1st DGI Consensus Conference in September 2010, Aerzen, Germany. European J Oral Implantology. 2011;4:59–66.
- Mardas N, Trullenque‐Eriksson A, MacBeth N, Petrie A, Donos N. Does ridge preservation following tooth extraction improve implant treatment outcomes: a systematic review: Group 4: therapeutic concepts and methods. Clin Oral Implants Res. 2015;26(Suppl 11):180–201.
- Cardaropoli G, Araújo M, Lindhe J. Dynamics of bone tissue formation in tooth extraction sites. An experimental study in dogs. J Clin Periodontol. 2003;30:809–818.
- Muska E, Walter C, Knight A, et al. Atraumatic vertical tooth extraction: a proof of principle clinical study of a novel system. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;116:e303–e310.
- Barone A, Borgia V, Covani U, Ricci M, Piattelli A, Iezzi G. Flap versus flapless procedure for ridge preservation in alveolar extraction sockets: a histological evaluation in a randomized clinical trial. Clin Oral Implants Res. 2015;26:806–813.
- Barone A, Toti P, Piattelli A, Iezzi G, Derchi G, Covani U. Extraction socket healing in humans after ridge preservation techniques: comparison between flapless and flapped procedures in a randomized clinical trial. J Periodontol. 2014;85:14–23.
- Engler-Hamm D, Cheung WS, Yen A, Stark PC, Griffin T. Ridge preservation using a composite bone graft and a bioabsorbable membrane with and without primary wound closure: a comparative clinical trial. J Periodontol. 2011;82:377–387.
- Araújo MG, Lindhe J. Ridge alterations following tooth extraction with and without flap elevation: an experimental study in the dog. Clin Oral Implants Res. 2009;20:545–549.
- Barone A, Ricci M, Tonelli P, Santini S, Covani U. Tissue changes of extraction sockets in humans: a comparison of spontaneous healing vs. ridge preservation with secondary soft tissue healing. Clin Oral Implants Res. 2013;24:1231–1237.
- Barber HD, Lignelli J, Smith BM, Bartee BK. Using a dense PTFE membrane without primary closure to achieve bone and tissue regeneration. J Oral Maxillofac Surg. 2007;65:748–752.
- Fotek PD, Neiva RF, Wang HL. Comparison of dermal matrix and polytetrafluoroethylene membrane for socket bone augmentation: a clinical and histologic study. J Periodontol. 2009;80:776–785.
- Araújo MG, Lindhe J. Socket grafting with the use of autologous bone: an experimental study in the dog. Clin Oral Implants Res. 2011;22:9–13.
- Serrano Mendez C, Lang NP, Caneva M, Ramirez Lemus G, Mora Solano G, Botticelli D. Comparison of allografts and xenografts used for alveolar ridge preservation. A clinical and histomorphometric RCT in humans. Clini Implant Dent Related Res. 2017;19:608–615.
- Wood RA, Mealey BL. Histologic comparison of healing after tooth extraction with ridge preservation using mineralized versus demineralized freeze-dried bone allograft. J Periodontol. 2012;83:329–336.
- Camargo PM, Lekovic V, Weinlaender M, et al. Influence of bioactive glass on changes in alveolar process dimensions after exodontia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;90:581–586.
- Jung RE, Philipp A, Annen BM, et al. Radiographic evaluation of different techniques for ridge preservation after tooth extraction: a randomized controlled clinical trial. J Clin Periodontol. 2013;40:90–98.
- Lekovic V, Kenney EB, Weinlaender M, et al. A bone regenerative approach to alveolar ridge maintenance following tooth extraction. Report of 10 cases. J Periodontol. 1997;68:563–570.
- Lekovic V, Camargo PM, Klokkevold PR, et al. Preservation of alveolar bone in extraction sockets using bioabsorbable membranes. J Periodontol. 1998;69:1044–1049.
- Hoffmann O, Bartee BK, Beaumont C, Kasaj A, Deli G, Zafiropoulos GG. Alveolar bone preservation in extraction sockets using non-resorbable dPTFE membranes: a retrospective non-randomized study. J Periodontol. 2008;79:1355–1369.
- Fickl S, Fischer K, Petersen N, et al. Dimensional evaluation of different ridge preservation techniques: a randomized clinical study. Int J Periodontics Restorative Dent. 2017;37:403–410.
- Brownfield LA, Weltman RL. Ridge preservation with or without an osteoinductive allograft: a clinical, radiographic, micro-computed tomography, and histologic study evaluating dimensional changes and new bone formation of the alveolar ridge. J Periodontol. 2012;83:581–589.
- Beck TM, Mealey BL. Histologic analysis of healing after tooth extraction with ridge preservation using mineralized human bone allograft. J Periodontol. 2010;81:1765–1772.
- Sclar AG. Preserving alveolar ridge anatomy following tooth removal in conjunction with immediate implant placement. The Bio-Col technique. Atlas Oral Maxillofac Surg Clin North Am. 1999;7:39–59.
- Wang HL, Tsao YP. Mineralized bone allograft-plug socket augmentation: rationale and technique. Implant Dent. 2007;16:33–41.
- Wang HL, Tsao YP. Histologic evaluation of socket augmentation with mineralized human allograft. Int J Periodontics Restorative Dent. 2008;28:231–237.
- Januário AL, Duarte WR, Barriviera M, Mesti JC, Araújo MG, Lindhe J. Dimension of the facial bone wall in the anterior maxilla: a cone-beam computed tomography study. Clin Oral Implants Res. 2011;22:1168–1171.
- Cook DR, Mealey BL, Verrett RG, et al. Relationship between clinical periodontal biotype and labial plate thickness: an in vivo study. Int J Periodontics Restorative Dent. 2011;31:345–354.
- Frost NA, Banjar AA, Galloway PB, Huynh-Ba G, Mealey BL. The decision-making process for ridge preservation procedures after tooth extraction. Clin Advances Periodontics. 2014;4:56-63.
- Sharan A, Madjar D. Maxillary sinus pneumatization following extractions: a radiographic study. Int J Oral Maxillofac Implants. 2008;23:48–56.
- Rasperini G, Canullo L, Dellavia C, Pellegrini G, Simion M. Socket grafting in the posterior maxilla reduces the need for sinus augmentation. Int J Periodontics Restorative Dent. 2010;30:265–273.
- Hämmerle CH, Araújo MG, Simion M, Osteology Consensus Group 2011. Evidence-based knowledge on the biology and treatment of extraction sockets. Clin Oral Implants Res. 2012;23(Suppl 5):80–82.
- MacBeth N, Trullenque-Eriksson A, Donos N, Mardas N. Hard and soft tissue changes following alveolar ridge preservation: a systematic review. Clin Oral Implants Res. 2017;28:982–1004.
- Laurito D, Cugnetto R, Lollobrigida M, et al. Socket preservation with d-PTFE membrane: histologic analysis of the newly formed matrix at membrane removal. Int J Periodontics Restorative Dent. 2016;36:877–883
The authors have no commercial conflicts of interest to disclose.
From Decisions in Dentistry. October 2018;4(10):42–46.
