

Universal Classification in Endodontic Diagnosis
Establishing a proper pulpal and periapical diagnosis is key to determining appropriate clinical treatment.
Establishing a proper pulpal and periapical diagnosis is key to determining appropriate clinical treatment
Historically, there have been a variety of diagnostic classification systems advocated for determining endodontic disease.1 Unfortunately, the majority of them have been based upon histopathological findings, rather than clinical findings — often leading to confusion, misleading terminology and incorrect diagnoses.2 A key purpose of establishing a proper pulpal and periapical diagnosis is to determine appropriate clinical treatment.3,4 For example, incorrect assessment may lead to improper management. This could include performing endodontic therapy when it is not needed, or providing no treatment or some other therapy when a root canal procedure is truly indicated.
Another important purpose of establishing a universal classification system is to allow for effective communication between educators, clinicians, students and researchers. A simple and practical system that uses terms related to clinical findings is essential, and will help clinicians understand the progressive nature of pulpal and periapical disease, directing them to the most appropriate treatment approach for each condition.
In 2008, the American Association of Endodontists (AAE) held a consensus conference to standardize diagnostic terms used in endodontics.1 The goals were to propose universal recommendations regarding endodontic diagnoses, and develop standardized definitions of key diagnostic terms that will be generally accepted by endodontists, educators, test construction experts, third parties, generalists, specialists and students. Attendees also sought to resolve concerns about testing and interpretation of results, and determine the radiographic criteria, objective test results, and clinical criteria needed to validate the diagnostic terms established at the conference. Both the AAE and American Board of Endodontics have accepted these terms and recommend their use across all dental disciplines and health care professions.5–7
This article will define each diagnostic term and describe each condition’s typical clinical and radiographic characteristics; in addition, representative case examples will be provided, when appropriate. Clinicians must recognize, however, that diseases of the pulp and periapical tissues are dynamic and progressive; as such, signs and symptoms will vary, depending on the stage of the disease and patient status. Coupled with this are the limitations associated with current pulp testing modalities, as well as clinical and radiographic examination techniques. In order to render proper treatment, a complete endodontic diagnosis must include both a pulpal and periapical diagnosis for each tooth evaluated.
![0614-endo-1]() EXAMINATION AND DIAGNOSTIC PROCEDURES
EXAMINATION AND DIAGNOSTIC PROCEDURES
 EXAMINATION AND DIAGNOSTIC PROCEDURES
EXAMINATION AND DIAGNOSTIC PROCEDURESEndodontic diagnosis is similar to a jigsaw puzzle, in that diagnosis cannot be made from a single, isolated piece of information4 (Table 1). The clinician must systematically gather all of the necessary information to make a “probable” diagnosis. When taking the medical and dental history, the clinician should already be formulating in his or her mind a preliminary, but logical, diagnosis — especially if there is a chief complaint. The clinical and radiographic examinations, in combination with a thorough periodontal evaluation and clinical testing (pulp and periapical tests, for example), are then used to confirm the preliminary diagnosis.4 In some cases, the clinical and radiographic examinations are inconclusive or give conflicting results, and, as a result, definitive pulp and periapical diagnoses cannot be made. It is also important to recognize that treatment should not be rendered without a diagnosis — and, in these situations, the patient may have to wait and be reassessed at a later date or referred to an endodontist.
Diagnostic Terminology Approved by the American Association of Endodontists and American Board of Endodontics5–7
PULPAL DIAGNOSES8–13
Normal Pulp is a clinical diagnostic category in which the pulp is symptom free and normally responsive to pulp testing. Although the pulp may not be histologically normal, a “clinically” normal pulp results in a mild or transient response to thermal (cold) testing, lasting no more than one to two seconds after the stimulus is removed. One cannot arrive at a probable diagnosis without comparing the tooth in question with adjacent and contralateral teeth. It is best to test the adjacent teeth and contralateral teeth first so that the patient is familiar with the experience of a normal response to cold.
Reversible Pulpitis is based upon subjective and objective findings indicating that the inflammation should resolve and the pulp return to normal following appropriate management of the etiology. Discomfort is experienced when a stimulus, such as cold or sweet, is applied, and goes away within a couple of seconds after the stimulus is removed. Typical etiologies may include exposed dentin (dentinal sensitivity), caries or deep restorations. There are no significant radiographic changes in the periapical region of the suspect tooth, and the pain experienced is not spontaneous. Following the management of the etiology (e.g., caries removal plus restoration or covering the exposed dentin), the tooth requires further evaluation to determine whether the reversible pulpitis has returned to a normal status. Although dentinal sensitivity is not an inflammatory process, per se, all of the symptoms of this entity mimic those of a reversible pulpitis.
Symptomatic Irreversible Pulpitis is based on subjective and objective findings that the vital inflamed pulp is incapable of healing and that root canal treatment is indicated. Characteristics may include sharp pain upon thermal stimulus, lingering pain (often 30 seconds or longer after stimulus removal), spontaneity (unprovoked pain) and referred pain. Sometimes, the pain may be accentuated by postural changes, such as lying down or bending over. In addition, over-the-counter analgesics are typically ineffective. Common etiologies may include deep caries, extensive restorations, or fractures exposing the pulpal tissues. Teeth with symptomatic irreversible pulpitis may be difficult to diagnose because the inflammation has not yet reached the periapical tissues, thus resulting in no pain or discomfort to percussion. In such cases, the patient’s dental history and thermal testing are the primary tools for assessing pulpal status.
Asymptomatic Irreversible Pulpitis is a clinical diagnosis based on subjective and objective findings indicating that the vital inflamed pulp is incapable of healing and that root canal treatment is indicated. These cases have no clinical symptoms and usually respond normally to thermal testing, but may have had trauma or deep caries that would likely result in exposure following removal.
As with pulp testing, comparative testing for percussion and palpation should always begin with normal teeth as a baseline
Pulp Necrosis is a clinical diagnostic category indicating death of the dental pulp, necessitating root canal treatment. The pulp is nonresponsive to pulp testing and is asymptomatic. Pulp necrosis by itself does not cause apical periodontitis (e.g., pain to percussion or radiographic evidence of osseous breakdown) unless the canal is infected. Some teeth may be nonresponsive to pulp testing because of calcification or recent history of trauma, or it may simply be that the tooth is not responding. As previously stated, this is why all testing must be of a comparative nature (e.g., the patient may not respond to thermal testing on any teeth).
Previously Treated is a clinical diagnostic category indicating that the tooth has been endodontically treated and the canals are obturated with various filling materials (other than intracanal medicaments). The tooth typically does not respond to thermal or electric pulp testing.
Previously Initiated Therapy is a clinical diagnostic category indicating that the tooth has been previously treated by partial endodontic therapy, such as a pulpotomy or pulpectomy. Depending on the level of therapy, the tooth may or may not respond to pulp testing modalities.
key takeaways
- A key purpose of establishing a proper pulpal and periapical diagnosis is to determine appropriate clinical treatment.3,4
- A simple, practical and universal classification system for endodontic diagnosis that uses terms related to clinical findings is essential.
- This system will help clinicians understand the progressive nature of pulpal and periapical disease, and guide them to the most appropriate treatment.
- The American Association of Endodontists and American Board of Endodontics have accepted the terms described in this article, and recommend their use across all dental disciplines.5–7
- In order to render proper treatment, a complete endodontic diagnosis must include both a pulpal and periapical diagnosis for each tooth evaluated.
- If in doubt, general practitioners should always refer patients to an endodontist for further evaluation.
APICAL DIAGNOSES8–13
Normal Apical Tissues are not sensitive to percussion or palpation testing and, radiographically, the lamina dura surrounding the root is intact and the periodontal ligament space is uniform. As with pulp testing, comparative testing for percussion and palpation should always begin with normal teeth as a baseline for the patient.
Symptomatic Apical Periodontitis represents inflammation, usually of the apical periodontium, producing clinical symptoms involving a painful response to biting and/or percussion or palpation. This may or may not be accompanied by radiographic changes (i.e., depending upon the stage of the disease, there may be normal width of the periodontal ligament or there may be periapical radiolucency). Severe pain to percussion and/or palpation is highly indicative of a degenerating pulp, and root canal treatment is needed.
Asymptomatic Apical Periodontitis is inflammation and destruction of the apical periodontium that is of pulpal origin. It appears as an apical radiolucency and does not present clinical symptoms (e.g., there is no pain on percussion or palpation).
Chronic Apical Abscess is an inflammatory reaction to pulpal infection and necrosis characterized by gradual onset, little or no discomfort, and an intermittent discharge of pus through an associated sinus tract. Radiographically, there are typically signs of osseous destruction, such as a radiolucency. To identify the source of a draining sinus tract when present, a gutta-percha cone is carefully placed through the stoma or opening until it stops and a radiograph is taken.
Acute Apical Abscess is an inflammatory reaction to pulpal infection and necrosis characterized by rapid onset, spontaneous pain, extreme tenderness of the tooth to pressure, pus formation, and swelling of associated tissues. There may be no radiographic signs of destruction and the patient often experiences malaise, fever and lymphadenopathy.
Condensing Osteitis is a diffuse, radiopaque lesion representing a localized bony reaction to a low-grade inflammatory stimulus usually seen at the apex of the tooth.
DIAGNOSTIC CASE EXAMPLES
 Figure 1. This mandibular right first molar had been hypersensitive to cold and sweets over the past few months, but the symptoms have subsided. Now there is no response to thermal testing, but there is tenderness to biting and pain upon percussion. Radiographically, there are diffuse radiopacities around the root apices. Diagnosis: Pulp necrosis; symptomatic apical periodontitis with condensing osteitis. Nonsurgical endodontic treatment is indicated, followed by a build-up and crown. Over time the condensing osteitis should regress partially or totally.14
Figure 1. This mandibular right first molar had been hypersensitive to cold and sweets over the past few months, but the symptoms have subsided. Now there is no response to thermal testing, but there is tenderness to biting and pain upon percussion. Radiographically, there are diffuse radiopacities around the root apices. Diagnosis: Pulp necrosis; symptomatic apical periodontitis with condensing osteitis. Nonsurgical endodontic treatment is indicated, followed by a build-up and crown. Over time the condensing osteitis should regress partially or totally.14
 Figure 2. Following the placement of a full gold crown on the maxillary right second molar, the patient complained of sensitivity to both hot and cold liquids; now the discomfort is spontaneous. Upon application of a pulp vitality refrigerant spray on this tooth (i.e., thermal testing), the patient experienced pain, and, upon removal of the stimulus, the discomfort lingered for 12 seconds. Responses to both percussion and palpation were normal; radiographically, there was no evidence of osseous changes. Diagnosis: Symptomatic irreversible pulpitis; normal apical tissues. Nonsurgical endodontic treatment is indicated; access is to be repaired with a permanent restoration. Note that the maxillary second premolar has severe distal caries. Following evaluation, the tooth was diagnosed with symptomatic irreversible pulpitis (hypersensitive to cold, lingering eight seconds), and symptomatic apical periodontitis (pain to percussion).
Figure 2. Following the placement of a full gold crown on the maxillary right second molar, the patient complained of sensitivity to both hot and cold liquids; now the discomfort is spontaneous. Upon application of a pulp vitality refrigerant spray on this tooth (i.e., thermal testing), the patient experienced pain, and, upon removal of the stimulus, the discomfort lingered for 12 seconds. Responses to both percussion and palpation were normal; radiographically, there was no evidence of osseous changes. Diagnosis: Symptomatic irreversible pulpitis; normal apical tissues. Nonsurgical endodontic treatment is indicated; access is to be repaired with a permanent restoration. Note that the maxillary second premolar has severe distal caries. Following evaluation, the tooth was diagnosed with symptomatic irreversible pulpitis (hypersensitive to cold, lingering eight seconds), and symptomatic apical periodontitis (pain to percussion).
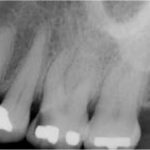 Figure 3. The maxillary left first molar has occlusal-mesial caries and the patient has been complaining of sensitivity to sweets and cold liquids. There is no discomfort to biting or percussion. The tooth is hyperresponsive to thermal (cold) testing, with no lingering pain. Diagnosis: reversible pulpitis; normal apical tissues. Treatment would be excavation of the caries, followed by placement of a permanent restoration. If the pulp is exposed, treatment would be nonsurgical endodontic treatment, followed by a permanent restoration, such as a crown.
Figure 3. The maxillary left first molar has occlusal-mesial caries and the patient has been complaining of sensitivity to sweets and cold liquids. There is no discomfort to biting or percussion. The tooth is hyperresponsive to thermal (cold) testing, with no lingering pain. Diagnosis: reversible pulpitis; normal apical tissues. Treatment would be excavation of the caries, followed by placement of a permanent restoration. If the pulp is exposed, treatment would be nonsurgical endodontic treatment, followed by a permanent restoration, such as a crown.
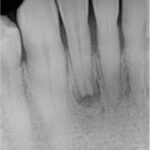 Figure 4. This mandibular right lateral incisor has an apical radiolucency that was discovered during a routine examination. There was a history of trauma more than 10 years ago and the tooth was slightly discolored. The tooth did not respond to thermal (cold) testing or electric pulp testing, although adjacent teeth responded normally to pulp testing. There was no tenderness to percussion or palpation in the region. Diagnosis: pulp necrosis; asymptomatic apical periodontitis. Treatment is nonsurgical endodontic therapy, followed by bleaching and permanent restoration.
Figure 4. This mandibular right lateral incisor has an apical radiolucency that was discovered during a routine examination. There was a history of trauma more than 10 years ago and the tooth was slightly discolored. The tooth did not respond to thermal (cold) testing or electric pulp testing, although adjacent teeth responded normally to pulp testing. There was no tenderness to percussion or palpation in the region. Diagnosis: pulp necrosis; asymptomatic apical periodontitis. Treatment is nonsurgical endodontic therapy, followed by bleaching and permanent restoration.
 Figure 5. The mandibular left first molar demonstrates a relatively large apical radiolucency encompassing both the mesial and distal roots, along with furcation involvement. Periodontal probing depths were all within normal limits. The tooth did not respond to thermal (cold) testing, and both percussion and palpation elicited normal responses. There was a draining sinus tract on the midfacial of the attached gingiva, which was traced with a gutta-percha cone. There was recurrent caries around the distal margin of the crown. Diagnosis: pulp necrosis; chronic apical abscess. Treatment is crown removal, nonsurgical endodontic treatment and placement of a new crown.
Figure 5. The mandibular left first molar demonstrates a relatively large apical radiolucency encompassing both the mesial and distal roots, along with furcation involvement. Periodontal probing depths were all within normal limits. The tooth did not respond to thermal (cold) testing, and both percussion and palpation elicited normal responses. There was a draining sinus tract on the midfacial of the attached gingiva, which was traced with a gutta-percha cone. There was recurrent caries around the distal margin of the crown. Diagnosis: pulp necrosis; chronic apical abscess. Treatment is crown removal, nonsurgical endodontic treatment and placement of a new crown.
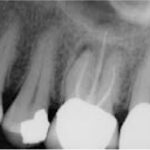 Figure 6. The maxillary left first molar was endodontically treated more than 10 years ago. The patient is complaining of pain to biting over the past three months. There appear to be apical radiolucencies around all three roots. The tooth was tender to both percussion and use of a fracture-detecting device. Diagnosis: previously treated; symptomatic apical periodontitis. Treatment is nonsurgical endodontic retreatment, followed by permanent restoration of the access cavity.
Figure 6. The maxillary left first molar was endodontically treated more than 10 years ago. The patient is complaining of pain to biting over the past three months. There appear to be apical radiolucencies around all three roots. The tooth was tender to both percussion and use of a fracture-detecting device. Diagnosis: previously treated; symptomatic apical periodontitis. Treatment is nonsurgical endodontic retreatment, followed by permanent restoration of the access cavity.
 Figure 7. This maxillary left lateral incisor exhibits an apical radiolucency. There is no history of pain and the tooth is asymptomatic. There is no response to thermal (cold) testing or electric pulp testing, whereas the adjacent teeth respond normally to both tests. There is no tenderness to percussion or palpation. Diagnosis: pulp necrosis; asymptomatic apical periodontitis. Treatment is nonsurgical endodontic therapy and placement of a permanent restoration.
Figure 7. This maxillary left lateral incisor exhibits an apical radiolucency. There is no history of pain and the tooth is asymptomatic. There is no response to thermal (cold) testing or electric pulp testing, whereas the adjacent teeth respond normally to both tests. There is no tenderness to percussion or palpation. Diagnosis: pulp necrosis; asymptomatic apical periodontitis. Treatment is nonsurgical endodontic therapy and placement of a permanent restoration.
CONCLUSION
Recognizing that a key purpose of establishing an accurate pulpal and periapical diagnosis is to determine appropriate clinical treatment,3,4 dental professionals can apply this universal classification system to help ensure sound clinical management. The AAE and American Board of Endodontics have accepted the foregoing terms and recommend their use across all dental disciplines.5–7 But while this practical system goes a long way toward eliminating possible confusion, clinicians must recognize that diseases of the pulp and periapical tissues are dynamic and progressive. As such, signs and symptoms will vary, depending on the stage of the disease and patient status.
It’s important to remember that an accurate diagnosis cannot be made from a single, isolated piece of information,4 and that treatment should not be rendered without a definitive diagnosis. If in doubt, general practitioners should always refer patients to an endodontic specialist.
References
- Glickman GN. AAE consensus conference on diagnostic terminology: background and perspectives. J Endod. 2009;35:1619.
- Seltzer S, Bender IB, Ziontz M. The dynamics of pulp inflammation: correlations between diagnostic data and actual histologic findings in the pulp. Oral Surg Oral Med Oral Pathol. 1963;16:846–871;969–977.
- Berman LH, Hartwell GR. Diagnosis. In: Cohen S, Hargreaves KM, eds. Pathways of the Pulp, 11th ed. St. Louis, MO: Mosby/Elsevier; 2011:2–39.
- Schweitzer JL. The endodontic diagnostic puzzle. Gen Dent. 2009;57(6):560–567.
- AAE Consensus Conference Recommended Diagnostic Terminology. J Endod. 2009;35:1634.
- American Association of Endodontists. Glossary of Endodontic Terms. 8th ed. 2012.
- Glickman GN, Bakland LK, Fouad AF, Hargreaves KM, Schwartz SA. Diagnostic terminology: report of an online survey. J Endod. 2009;35:1625.
- Jafarzadeh H, Abbott PV. Review of pulp sensibility tests. Part I: general information and thermal tests. Int Endod J. 2010;43:738–762.
- Jafarzadeh H, Abbott PV. Review of pulp sensibility tests. Part II: electric pulp tests and test cavities. Int Endod J. 2010;43:945–958.
- Newton CW, Hoen MM, Goodis HE, Johnson BR, McClanahan SB. Identify and determine the metrics, hierarchy, and predictive value of all the parameters and/or methods used during endodontic diagnosis. J Endod. 2009;35:1635.
- Levin LG, Law AS, Holland GR, Abbot PV, Roda RS. Identify and define all diagnostic terms for pulpal health and disease states. J Endod. 2009;35:1645.
- Gutmann JL, Baumgartner JC, Gluskin AH, Hartwell GR, Walton RE. Identify and define all diagnostic terms for periapical/periradicular health and disease states. J Endod. 2009;35:1658.
- Rosenberg PA, Schindler WG, Krell KV, Hicks ML, Davis SB. Identify the endodontic treatment modalities. J Endod. 2009;35:1675.
- Green TL, Walton RE, Clark JM, Maixner D. Histologic examination of condensing osteitis in cadaver specimens. J Endod. 2013;39:977–979.
- Abbott PV, Yu C. A clinical classification of the status of the pulp and the root canal system. Aust Dent J. 2007;52(Endod Suppl):S17–S31.
A version of this article originally appeared in ENDODONTICS: Colleagues for Excellence, Fall 2013. Reused with permission from the American Association of Endodontists, ©2013. The AAE clinical newsletter is available at aae.org/colleagues.
