

Techniques to Enhance Radiographic Utility
The diagnostic quality of any X-ray depends on the quality of the technique used in producing the image.
The diagnostic quality of any x-ray depends on the quality of the technique used in producing the image
Bitewing radiographs are a primary source of adjunctive information in the detection and diagnosis of dental caries.1 In addition, clinicians can compare serial bitewings to identify crestal bone changes, and horizontal and vertical bone loss to aid in the diagnosis of periodontitis.1 Unlike periapical radiographs, bitewings display the crowns of teeth and crestal bone in both arches. According to the American Dental Association, bitewing radiographs should be used to help detect interproximal caries in the context of patient risk factors, age, and information gleaned from previous radiographs.2

Prior to ordering radiographs, the dentist should always consider the risks and benefits of exposing radiographs compared to the diagnostic value of the information gained. As such, the operator should conduct a clinical exam and evaluate the patient’s health and dental histories. In conjunction with the patient’s age, these factors will guide the clinician in selecting the appropriate radiographic projections. Once this is determined, it is the responsibility of the dentist to make sure the dose rendered is as low as reasonably achievable (the ALARA principle). One method for achieving this is to select radiographic projections based on the patient’s need. Radiographs should not be used for screening prior to a clinical exam. Another way is to use radiographic equipment that minimizes dose — such as rectangular collimation, fast-speed film or digital receptors, and beam-alignment devices; it’s also important to use correct exposure settings. Lastly, the quality of the radiographer’s technique is paramount for rendering images of diagnostic value.

The exposure geometry used with bitewing radiography enhances its ability to identify interproximal caries that are not readily detectable by other means. Errors in technique, however, can limit radiographs’ diagnostic utility. In fact, research has shown that the majority of retakes stem from poor image quality in the initial X-ray.3 Errors in density and contrast can limit a practitioner’s ability to capture the maximum information available.1 Inappropriate exposure parameters can easily be corrected by displaying a wall-mounted technique chart that includes information regarding appropriate exposure settings.
Digital-based systems typically include software that enhances image quality in problematic exposures, thus avoiding the need to reexpose the patient to ionizing radiation. A clinician’s choice of digital detector or receptor and geometrical alignment device can also introduce errors. This article will discuss methods for ensuring diagnostic-quality, error-free imaging. It will also explore common technique errors, as well as clinical solutions.
PERFORMANCE CRITERIA
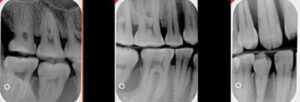
A bitewing survey is typically composed of four horizontal projections, two on each side of the mouth (premolar and molar).1 One exception is when vertical bitewings are indicated (or when larger detectors are used). So as to better reveal the relationships of the dentition to interproximal crestal bone levels, vertical bitewings are often indicated in cases in which current or past periodontitis is suspected. Furthermore, a bitewing survey using vertical bitewings may require three bitewings per side to cover the entire area of interest (Figure 1). Another exception is when a single Size 3 detector is used on each side. While this technique reduces radiation exposure, it may not depict the interproximal areas of all teeth without image overlap.
Regardless of the devices or receptors used, when exposing bitewing radiographs, it is important to focus on five performance criteria:
- The maxillary and mandibular arches should be imaged equally.
- The premolar image should display the distal surfaces of the maxillary and mandibular canines.
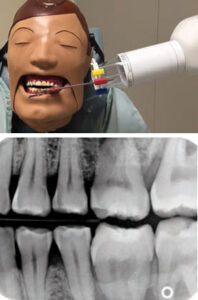
- In the molar image, the distal of the second premolar should be visible, as should the complete terminal molars on each side of the mouth.
- When exposing the premolar image, there should be no overlap of the distal surface of the first premolars with the mesial surfaces of the second premolars.
- In the molar exposure, there should be no overlap of the distal surface of the maxillary first molars and the mesial surfaces of the second molars (Figure 2).
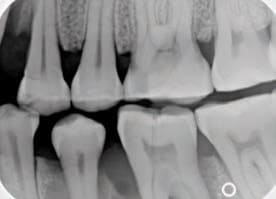
Figure 3 displays a half-mouth example of vertical bitewings. The number of vertical bitewings may range from two to three per side, depending on how many teeth are present. Here, a Size 1 detector was used to display the interproximal area between the canines and first premolars. The middle image should depict the interproximal spaces between the first and second premolars, as well as between the second premolars and first molars. The molar image displays the interproximal spaces between the first, second and third molars.
Key Takeaways
- The quality of the radiographer’s technique is paramount to rendering high-quality images of diagnostic value.
- Unlike periapical radiographs, bitewing images display the crowns of teeth and crestal bone in both arches, making them a primary source of adjunctive information in the detection and diagnosis of dental caries.1
- Clinicians should always consider the risks and benefits of exposing radiographs compared to their diagnostic value. It is the operator’s responsibility to make sure the dose rendered is as low as reasonably achievable (ALARA principle).
- Inappropriate exposure parameters can easily be corrected by displaying a wall-mounted technique chart that includes information regarding appropriate exposure settings.
- Technique errors most commonly occur due to incorrect placement of the detector, erroneous vertical or horizontal beam alignment, or collimator centering.
PROJECTION GEOMETRY
One of the most common errors when exposing bitewing images is failing to prevent horizontal overlapping. Horizontal overlap is a result of the X-ray beam not passing through the open interproximal area at right angles to a properly positioned detector. Correcting this error can usually be achieved by inclining the tubehead in a more mesial or distal direction. The “same lingual/opposite buccal” rule can be used to determine which direction the tubehead and/or receptor-holding device should be adjusted. In a normal anatomical relationship, the cusps should appear almost directly on top of one another radiographically. If they don’t, adjust the tubehead in a mesial or distal direction. If the lingual cusp appears mesial to the facial cusp, the tubehead was angled too far in the mesial direction in relation to the interproximal contact. To correct this horizontal overlap, the tubehead should be shifted horizontally in a distal direction. If the lingual cusp was distal to the facial cusp, the tubehead should be shifted horizontally in the mesial direction to open the interproximal area of interest (Figure 4).


Vertical angulation errors may also produce a diagnostically unacceptable bitewing. The “buccal object” rule may be used to help correct angulation; this states that a buccal object will appear in the same direction as the beam is overly angulated. Thus, in the bitewing projection, the images of the arches may be shifted up or down, depending on vertical angulation. This problem can be eliminated if the tubehead is positioned in a +10° vertical angulation (i.e., the tubehead beam is angled slightly downward when the patient’s occlusal plane is parallel to the floor). If a beam-alignment device is used, the operator should position the device in the mouth so the beam is pointing down slightly (Figure 5).
If the beam is pointing up (Figure 6), the holder isn’t positioned correctly. The operator should determine why this is happening and reposition the biteblock to achieve an appropriate vertical angle.
RECEPTOR PLACEMENT
Detector placement errors often occur because the receptor is uncomfortable. To improve patient comfort, the receptor can be repositioned more toward the midline of the palate or tongue to avoid placement too close to the alveolar ridges. Another receptor placement error is not positioning the detector to image the distal of the canine (Figure 7). This issue is commonly encountered among patients with small mouths. If the detector cannot be positioned more mesially, attempt to position the detector more toward the center of the mouth by displacing the tongue to the contralateral side. This provides more anterior space for the mesial margin of the detector (although it can induce gagging). Asking patients to hold their breath or concentrate on breathing through the nose can ease the gagging reflex.


CONE CUTS AND COLLIMATOR CENTERING
Collimator cuts (also known as cone cuts) result from incorrect centering of the collimator over the receptor and its holder apparatus (if the latter is in use). Cone cuts are fairly common when tightly confined X-ray beams, characterized by rectangular collimation, are used (Figure 8). Regardless of whether a beam-alignment device is used, collimator cuts will occur if the beam cross-section fails to expose the entire receptor. To decrease the likelihood of cone cuts, the operator must carefully align properly positioned detectors and holders to ensure the X-ray beam’s cross-section includes the entire receptor.
SOLUTIONS TO COMMON ERRORS
Technique errors most commonly occur due to incorrect placement of the detector, erroneous vertical or horizontal beam alignment, or collimator centering. Clinicians should be able to determine the causes of errors in order to correct them.
In Figure 9, the image displays more of the maxillary arch than the mandibular arch. A good diagnostic image would display equal amounts of the maxillary and mandibular arches. Additionally, the mandibular crestal bone was not imaged. The error seen in Figure 9 is most likely due to the vertical angulation being positioned too steeply (i.e., the collimator was aimed too far downward). To correct this, the vertical alignment of the collimator should be repositioned at +10°, figured from an occlusal plane that is parallel with the floor.
As seen in the premolar bitewing image in Figure 10, the projection is missing the distal of the maxillary canine and mesial of the maxillary first premolar. There is slight horizontal overlap between the maxillary premolars. But is this a detector placement error or horizontal angulation error? This may have occurred because of incorrect detector placement and/or incorrect horizontal angulation. The detector may not have been placed sufficiently mesial, and/or the tubehead may have been aimed too mesially, thus projecting the mesial of the premolar off the receptor and causing horizontal overlap.



A bitewing image that has a clear diagonal area in the right corner, thus preventing the display of diagnostic information from the maxillary second molar, is evident in Figure 11. This error is caused by the rectangular collimator being seated improperly in the indentations of the aiming ring, and can be prevented by checking both sides of the aiming ring for complete placement of the collimator into the ring indentations.
Figure 12 displays a premolar bitewing in which the distal of the canine and first premolars are not imaged in the projection. This error stems from improper detector placement, with the receptor positioned too far to the distal. This is a common problem with patients with small mouths. To correct this, place the detector more mesially. If this isn’t possible, attempt to position the detector more toward the center of the mouth by displacing the tongue to the contralateral side, thereby providing more anterior space for the mesial margin of the detector.
FUTURE TECHNOLOGY
Traditionally, bitewing radiographs have been used in caries diagnosis, especially for detecting interproximal caries. In recent years, however, panoramic imaging technology has improved, and now produces images comparable to traditional bitewings. An in vitro study published by Abu El-Ela et al4 in 2016 compared digital images for the detection of interproximal caries using photostimulable receptors, complementary metal oxide semiconductor receptors, and a panoramic X-ray unit. The findings indicated no significant difference between the three radiographic bitewing techniques for the detection of enamel caries.
A similar study published by Abdinian et al5 in 2015 compared a variety of panoramic radiographs with intraoral bitewing images in the detection of interproximal caries. They reported the improved panoramic and extraoral bitewing radiographic images were superior to conventional panoramic images. In contrast, Kamburoglu et al6 noted in 2012 that intraoral bitewing images were better for diagnosing interproximal caries than extraoral bitewing and panoramic images. The difference in results may be due to improvements in imaging technology since 2012. Thus, continued research is needed to assess new technology as it is introduced.
Contemporary dental radiography continues to incorporate new techniques and technology for the detection of anatomical changes suggestive of disease or healing.7 Regardless of the equipment used, clinicians must utilize sound radiographic techniques and strive to improve their skills in order to produce consistently useful diagnostic images while minimizing patient exposure to radiation in accordance with the ALARA principle.
References
- White SC, Pharoah MJ. Intraoral projections. In: Oral Radiology: Principles and Interpretation. Philadelphia: Elsevier Mosby; 2014:91–130.
- American Dental Association Council on Scientific Affairs: Dental Radiographic Examinations: Recommendations for Patient Selection and Limiting Radiation Exposure. Available at: http://www.ada.org/~/media/ADA/Member%20Center/FIles/ Dental_Radiographic_Examinations_2012.pdf Accessed August 15, 2016.
- Platin E, Janhom A, Tyndall D. A quantitative analysis of dental radiography quality assurance practices among North Carolina dentists. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;86:115–120.
- Abu El-Ela WH, Farid MM, Mostafa MS. Intraoral versus extraoral bitewing radiography in detection of enamel proximal caries: an ex vivo study. Dentomaxillofac Radiol. 2016;45:20150326.
- Abdinian M, Razavi SM, Faghihian R, Samety AA, Faghihian E. Accuracy of digital bitewing radiography vs different views of digital panoramic radiography for detection of proximal caries. J Dent (Tehran). 2015;12:290–297.
- Kamburoglu K, Kolsuz E, Murat S, Yüksel S, Ozen T. Proximal caries detection accuracy using intraoral bitewing radiography, extraoral bitewing radiography and panoramic radiography. Dentomaxillofac Radiol. 2012;41:450–459.
- Fuhrmann AW. Current practice in conventional and digital intraoral radiography: problems and solutions. Int J Comput Dent. 2006;9:61–68.
From Decisions in Dentistry. September 2016;2(09):22–24,26–27.
