

Subgingival Calculus Up Close
When used during minimally invasive periodontal procedures, the dental videoscope offers clinicians direct visualization of nearly undetectable calculus deposits.
When used during minimally invasive periodontal procedures, the dental videoscope offers clinicians direct visualization of nearly undetectable calculus deposits.
PURCHASE COURSE
This course was published in the December 2016 issue and expires December 2019.The author has no commercial conflicts of interest to disclose.This 2 credit self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the role of calculus in periodontal inflammation.
- Compare and contrast the features of the dental videoscope and dental endoscope.
- List clinical applications for the dental videoscope.
Inflammatory periodontal disease affects millions of patients in the United States and is, in fact, responsible for the vast majority of tooth loss in adults. It has also been associated with an increased incidence and prevalence of coronary artery disease, increased stroke risk, poor glycemic control, and increased incidence of preterm birth in expectant mothers.1 Oral health professionals are well aware that biofilm is the primary extrinsic etiologic factor in inflammatory periodontal disease. As the bacterial front progresses in the deepening sulcus, calculus forms on the root surface. It has been clearly shown that calculus deposits concentrate the toxins produced by the bacteria in the biofilm.
possible with the dental endoscope, surgical telescopes (loupes), or surgical microscope.
The complete removal of subgingival calculus remains a significant challenge for oral health professionals, however — and one of the most difficult aspects of deposit removal is the inability to see inside the pocket. The introduction of the dental videoscope (Figure 1) — a component-based intraoral video camera — has greatly aided clinicians’ visibility during nonsurgical periodontal therapy. By assisting in the direct visualization of calculus within the pocket, this device has the potential to help improve patients’ long-term outcomes.
Articles by Listgarten et al2–4 showed that it was possible to grow an epithelial attachment over previously root-planed subgingival calculus. This led to the theory that subgingival calculus was relatively innocuous and not directly involved in the inflammatory process of periodontal breakdown. A significant base of evidence, however, has demonstrated a direct connection between these hardened subgingival deposits and inflammation seen in the pocket wall.5–12 This connection was made possible with the advent of new technology. A study by Wilson et al5 showed that nearly 70% of the inflammation found in the wall of an active periodontal pocket was associated with a combination of calculus and biofilm. Less than 10% of the inflammation noted in periodontal disease was associated with plaque alone. The high level of association between calculus and clinically identifiable inflammation indicates that calculus plays a major role in the inflammatory element of periodontal disease. This suggests complete calculus removal is imperative to successful treatment.
CLOSE-UP VIEW

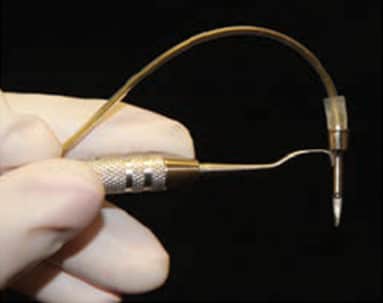
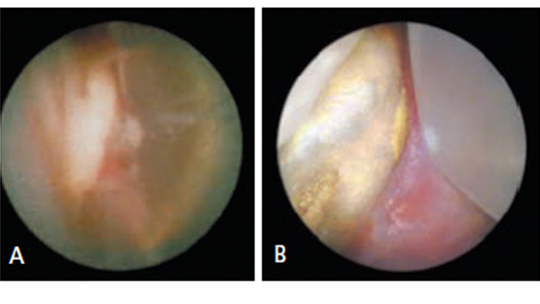
In the late 1990s, the ability to see the subgingival environment in real time increased exponentially as research began to validate the utility of the dental endoscope (Figure 2).13 This device consists ofa 0.9-mm flexible, fiber-optic cord with an externally mounted camera (Figure 3). This allows the operator to view an image on a monitor that represents a 3-mm-diameter subgingival space magnified up to 48 times (Figures 4A and 4B). The dental endoscope revolutionized the treatment of probing depths in the range of 4 to 6 mm.
Based on visualization provided by the dental endoscope, a direct relationship has been established between subgingival calculus and inflammation in the pocket wall.5 Knowing that inflammation is a contributory factor in disease progression, oral health professionals should attempt to remove as much subgingival calculus as possible. In the past, clinicians relied on tactile sense and clinical knowledge of root anatomy to determine the effectiveness of nonsurgical periodontal therapy. With the endoscope, however, clinicians are able to more effectively remove calculus through magnification and enhanced visualization of the subgingival space. Additionally, improved visualization enables clinicians to provide a more thorough diagnosis and definitive nonsurgical therapy.
A series of studies by Stambaugh et al13,14 showed the efficacy of using an endoscope for calculus detection and removal. In the first study, clinicians evaluated 42 teeth with pockets greater than 5 mm.14 The teeth were subsequently extracted and evaluated with direct vision and scanning electron microscopy. The results showed that more than 95% of all root deposits were detected correctly with the endoscope. In a follow-up study, 31 patients with refractory periodontitis were subjected, via endoscope, to scaling and root planing in 73 quadrants.13 The authors saw improvement in 71 out of 73 quadrants tested following calculus removal. They also reported improvements in probing depths and clinical attachment gain, and reductions in bleeding on probing. Additionally, the authors noted that pocket depth reduction continued to improve and was maintained over time.
DENTAL VIDEOSCOPE
enables clinicians to see an image on a
monitor that represents a 3-mm-diameter
subgingival space magnified up to 48 times.
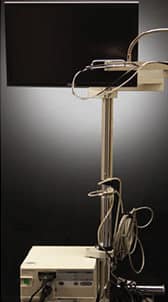
The introduction of the dental videoscope represents a significant advance in viewing technology. This device provides a much more accurate view of the subgingival environment than is available with the dental endoscope, surgical telescopes (loupes), or surgical microscope. Videoscope images are depicted in natural color and can be magnified 20 to 60 times, depending on the distance from the root surface. Unlike the endoscope, which uses a fiber-optic cord to transmit the image to an external camera, the videoscope has a camera at the end of the scope that transmits the digital image to a monitor (Figure 5). A gas shield (i.e., air) is used to keep the field of view clean and prevent the videoscope from fogging. This makes it possible to see calculus deposits that would not be visible with any other approach. It also allows clinicians to remove the calculus in real time and under direct visualization.15
The routine presence of very small lines — or microgrooves — on root surfaces within periodontal defects was an unexpected finding uncovered via the videoscope. These lines or microgrooves are noted in the vast majority of periodontal lesions. Termed “Harrel’s lines” after their discoverer, they appear to be routinely filled with small deposits of subgingival calculus. These calculus-filled microgrooves are not visible by any other device currently available, and certainly not by the naked eye.

The fact that microgrooves had not previously been detected seems to indicate calculus within the grooves has routinely been missed during periodontal treatment. As such, their presence may be a factor in the unpredictability of periodontal therapy outcomes.
CLINICAL APPLICATION
The videoscope is routinely used for a regenerative periodontal surgical procedure known as videoscope-assisted minimally invasive periodontal surgery (VMIS).15 Briefly, VMIS consists of very small incisions of 3 to 5 mm in length that are usually placed only on the lingual side. This avoids surgery on the esthetically sensitive facial aspect of the teeth. Split thickness incisions are recommended to help maintain the blood supply to the flap. Full thickness flap reflection, or reflection with a periosteal elevator often compromises the blood supply to the delicate papillary tissues, and is not recommended for a minimally invasive approach. The lingual flap is carefully reflected just enough to allow for placement of the videoscope, so the periodontal defect can be visualized on a monitor.
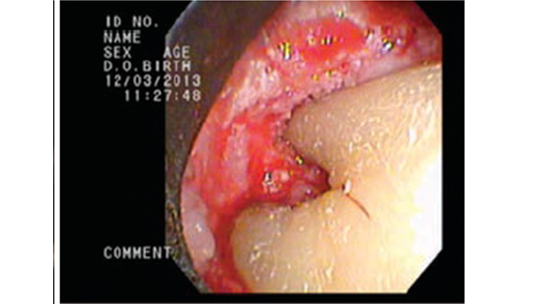
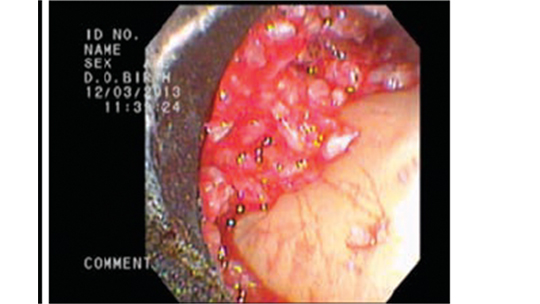
Using a combination of hand curets and ultrasonic instrumentation, the periodontal lesion is debrided to remove the infected granulation tissue, thus producing a smooth root surface with all calculus removed (Figure 6). Following debridement, the root surface is often treated with a root conditioning agent, such as ethylenediaminetetraacetic acid (EDTA), to remove any residual thin sheets of calculus (Figure 7). These sheets are not visible with the endoscope or other types of magnification, and their removal is the critical final step in complete debridement of the defect. In most instances, a bone graft and enamel matrix derivatives are placed in the site (Figure 8), after which a single vertical mattress suture is used to close the surgical site.

These calculus-filled microgrooves are detectable during the debriding and smoothing of the root surface. Sheets of calculus are present in the periodontal defect, even after closed root planing has been performed. After the gross calculus is removed, the underlying root surface (containing microgrooves) can be seen with the videoscope. Traditional root planing motions will not remove the calculus from these grooves because the depths of the microgrooves are not accessible with curets or ultrasonic inserts or tips. Typically, the microgrooves must be cleaned by carefully using the tip of a curet, followed by application of EDTA to dissolve the final smear layer of microscopic calculus. This removal must be performed under direct visualization. Currently, the videoscope is the only method that provides the direct visualization needed for this procedure. Occasionally, the grooves and sheets of calculus need to be removed with a surgical bur to allow for complete debridement of the defect.
Besides providing visualization that allows complete debridement, the use of the dental videoscope in combination with a minimally invasive approach has additional postsurgical benefits for patients. Due to the minimally invasive nature of the incisions and the small amount of soft tissue reflection, patients typically experience less surgical trauma, postoperative pain, postoperative recession, and postoperative cold sensitivity. One of the biggest advantages to the minimally invasive approach is the lack of recession at the surgical site. In a 2010 study, at 12 months postsurgery, Harrel et al16 noted 0.01 mm of recession when using this minimally invasive approach, and 0.08 mm of recession six years postsurgery.
In 2016, Harrel et al17 conducted a study on 30 patients with 110 sites of residual pocket probing depths of at least 5 mm, 2 mm loss of clinical attachment level, and radiographic evidence of bone loss. The patients received VMIS. At six months postsurgery, the patients presented with statistically significant improvements in pocket probing depths and clinical attachment levels. This approach has enabled clinicians to promote the regeneration of bone, ligament and cementum using very small incisions, minimal reflection of tissue, maintenance of the blood supply, and restriction of the surgery only to areas of localized, deep pocketing.
CALCULUS REMOVAL IS KEY
The role of subgingival calculus in the etiology and continuation of inflammatory periodontal disease should be reassessed. The knowledge base regarding periodontal disease and treatment is changing. The relevant issue now becomes to what degree, and with which approaches, should these accretions be removed.
Ample data exist in the literature indicating that individuals with inflammatory periodontal disease who have effective personal oral hygiene, and who comply with routine maintenance visits, tend to keep their teeth longer than noncompliant patients. Routine efforts on the part of patients and oral health professionals often result in stability of the periodontal lesion over the long term. The question is, how many individuals exhibit exemplary oral hygiene and maintain the number of suggested visits for periodontal maintenance? Unfortunately, the answer is a small percentage of patients with periodontal disease. As a result, progression of bone loss often occurs in noncompliant individuals.
These findings suggest that, in addition to encouraging effective oral hygiene and maintenance compliance, successful outcomes depend on a more thorough removal of subgingival calculus. What is the most effective way to achieve this goal, and thereby increase the probability of stability for these lesions over the long term? Traditionally, closed subgingival scaling and root planing has been the answer. Yet, multiple studies indicate the lack of effectiveness in removing subgingival accretions, especially in probing depths deeper than 5 mm.18–20 In 1978, Waerhaug21 noted a high chance of failure in effectively removing all calculus with closed subgingival scaling and root planing in periodontal pockets greater than 5 mm. This led the author to conclude, “one of the human causes of failure in subgingival scaling is that the operator cannot see what he or she is doing. But it may be equally bad that the operator cannot see the results of what he or she did not do. That is so because inflammatory foci caused by plaque remnants do not give clinical symptoms, which are visible at the gingival margin.”21
CONCLUSION
How does a clinician working in private practice deal with this conundrum? For patients with probing depths in the range of 4 to 6 mm, the dental endoscope is a potential answer. For patients whose probing depths are deeper, or in cases in which regeneration of lost periodontal attachment is the goal, the use of the dental videoscope presents the most useful modality at this time.
REFERENCES
- Friedewald VE, Kornman KS, Beck JD, et al. The American Journal of Cardiology and Journal of Periodontology editor’s consensus: periodontitis and atherosclerotic cardiovascular disease. J Periodontol. 2009;80:1021–1032.
- Listgarten MA, Ellegaard B. Electron microscopic evidence of a cellular attachment between junctional epithelium and dental calculus. J Periodontal Res. 1973;8:143–50.
- Listgarten MA, Mayo H, Amsterdam M. Ultrastructure of the attachment device between coccal and filamentous microorganisms in “corn cob” formations of dental plaque. Arch Oral Biol. 1973;18:651–656.
- Listgarten MA. Structure of surface coatings on teeth. A review. J Periodontol. 1976;47:139–147.
- Wilson TG, Harrel SK, Nunn ME, Francis B, Webb K. The relationship between the presence of tooth-borne subgingival deposits and inflammation found with a dental endoscope. J Periodontol. 2008;79:2029–2035.
- Wilson TG Jr, Carnio J, Schenk R, Myers G. Absence of histologic signs of chronic inflammation following closed subgingival scaling and root planing using the dental endoscope: human biopsies — a pilot study. J Periodontol. 2008;79:2036–2041.
- Canis MF, Kramer GM, Pameijer CM. Calculus attachment: review of the literature and findings. J Periodontol. 1979;50:406.
- Kepic TJ, O’Leary TJ, Kafrawy AH. Total calculus removal: an attainable objective? J Periodontol. 1990;61:16–20.
- Fleischer HC, Mellonig JT, Brayer WK, Gray JL, Barnett JD. Scaling and root planing efficacy in multirooted teeth. J Periodontol. 1989;60:402–409.
- Brayer WK, Mellonig JT, Dunlap RM, Marinak KW, Carson RE. Scaling and root planing effectiveness: the effect of root surface access and operator experience. J Periodontol. 1989:60:67–72.
- Stambaugh RV, Myers GC, Watenabe J, Lass C, Stambaugh KA. Clinical response to scaling and root planing aided by the dental endoscope [abstract]. J Dent Res. 2000;79:2762.
- Tan B, Gillam DG, Mordan NJ, Galgut PN. A preliminary investigation into the ultrastructure of dental calculus and associated bacteria. J Clin Periodontol. 2004;31:364.
- Stambaugh RV, Myers GC, Ebling WV, Beckman B, Stambaugh KA. Endoscopic visualization of the submarginal gingiva dental sulcus and tooth root surfaces. J Periodontol. 2002;73:374–382.
- Stambaugh RV, Myers GC, Ebling WV, Beckman B, Stambaugh KA. Endoscopic visualization of submarginal gingival root surfaces. J Dent Res. 2000;79(Spec Issue):600.
- Harrel SK, Abraham CM, Rivera-Hidalgo F, Shulman JD, Nunn ME. Videoscopeassisted minimally invasive periodontal surgery (V-MIS). J Clin Periodontol. 2014;41:900–907.
- Harrel SK, Wilson TG, Nunn ME. Prospective assessment of the use of enamel matrix proteins with minimally invasive surgery: Six year results. J Periodontol. 2010;81:435–441.
- Harrel SK, Abraham CM, Rivera-Hidalgo F, Shulman JD, Nunn ME. Videoscopeassisted minimally invasive periodontal surgery: one-year outcome and patient morbidity. Int J Periodontics Restorative Dent. 2016;36:363–371.
- Deas DE, Moritz AJ, Sagun RS Jr, Gruwell SF, Powell CA. Scaling and root planing vs. conservative surgery in the treatment of chronic periodontitis. Periodontol 2000. 2016;71:128–139.
- Pihlstrom BL, McHugh RB, Oliphant TH, Ortiz-Campos C. Comparison of surgical and nonsurgical treatment of periodontal disease. A review of current studies and additional results after 61⁄2 years. J Clin Periodontol. 1983;10:524–541.
- Heitz-Mayfield LJ, Trombelli L, Heitz F, Needleman I, Moles D. A systematic review of the effect of surgical debridement vs. non-surgical debridement for the treatment of chronic periodontitis. J Clin Periodontol. 2002;29(Suppl 3):92–102.
- Waerhaug J. Healing of the dento-epithelial junction following subgingival plaque control II: As observed on extracted teeth. J Periodontol. 1978;49:119–134.
Featured image courtesy of ERAXION/ISTOCK/ THINKSTOCK
From Decisions in Dentistry. December 2016:2(12):32-35.

