

Special Report–Embracing Precision Dentistry and Medicine
Now is the time to prepare for a major transformation in clinical approaches to personalized care.
Now is the time to prepare for a major transformation in clinical approaches to personalized care
The cornerstone of precision dentistry and medicine is targeting treatment to a patient’s specific needs on the basis of genetic, biomarker, epigenetic, phenotypic, and socioeconomic or psychosocial determinants that distinguish an individual from others with similar clinical presentations. The goal is to minimize errors in diagnosis, improve outcomes, and avoid unnecessary side effects. Precision medicine is poised to profoundly transform how clinicians approach health care. Imagine the right diagnosis for the right patient that enlists a highly personalized treatment with a predictable outcome. This paper will explore the foundations of individualized therapy — as well as the challenges and future opportunities for precision health care.
The following case synopsis helps illustrate how technology is changing clinical approaches to care. Ms. T is a 42-year-old woman who has had a persistent cough for four weeks. During her semiannual dental hygiene appointment, her dental hygienist suggested that she consult a physician. A chest X-ray and computed tomography scan revealed an advanced lung lesion, and a biopsy confirmed it was non-small-cell lung cancer. What can be done for Ms. T? Before 2004, an oncologist likely would have offered a treatment to which 10% of patients have a positive response, with uncertain outcomes and confounding side effects. If she were diagnosed in 2011 or later, Ms. T’s biopsy would be analyzed for a panel of genetic variants that can predict therapies to which she might best respond. The goal is to align a specific gene mutation in a specific molecular pathway with a targeted treatment. In this example, the lung tumor was shown to be responsive to a targeted agent, and the only side effect was a modest skin rash. The point of this clinical scenario is that today’s patients can undergo genomic analysis that helps clinicians identify a panel of targeted agents. Aligning a patient’s gene mutation with a targeted drug treatment is called pharmacogenomics.
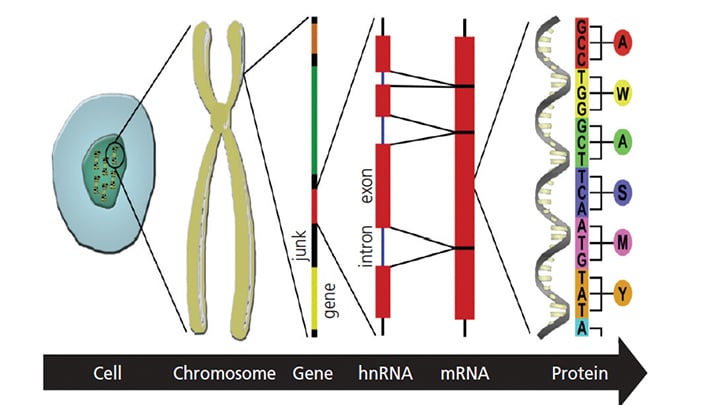
Thanks to more than 100 years of biomedical and behavioral research, a sophisticated synthesis is evolving that helps practitioners understand what makes a specific patient susceptible to disease or responsive to treatment — his or her genotype (an inventory of all that person’s genes), epigenetic profile (i.e., proteins outside of DNA that regulate gene expression but do not alter gene sequence), phenotype (the sum of observable characteristics, from hair color to caries), and the patient’s environment (e.g., socioeconomic status). Understanding the interaction or alignment of these factors is the foundation of precision health care. Aligning genotype with phenotype is termed phenomics, and is a process that entails a sophisticated assessment of the patient’s human biome. The human genome is the complete characterization of all genes found within the 46 pairs of chromosomes packed into the nucleus of every somatic cell in the body, plus all of the genes found specifically only within the DNA of mitochondria (Figure 1).
The term microbiome is the characterization of all genes within various viruses, bacteria and yeast associated with a given individual. Further, epigenome reflects the patterns of methylation associated with nucleotides within DNA that are cytosine and guanosine. The epigenetic mechanisms — such as methylation, acetylation and phosphorylation — involve chromosomal and nonchromosomal protein interactions with nucleotides that, in part, form the genetic code with DNA. Additional information and assessment will help determine a patient’s susceptibility to certain diseases and disorders, so that risk assessment and diagnosis, coupled with precise therapeutic protocols, can be individually tailored. This was the strategy used for Ms. T.
TECHNOLOGICAL ADVANCES
The confluence of genomics, bioinformatics and digital technology is accelerating the use of genetic information to enhance health care. Seventeen years ago, when the Human Genome Project completed the first draft of the 3 billion base pairs (i.e., A, C, T and G nucleotides or bases) that make up a person’s genomic DNA, it took a decade and nearly $300 million to complete a single person’s genome.1–4 By 2013, sequencing a patient’s genome with annotation could be accomplished in less than a day for less than $1000 per genome.1–5 The goal is to reduce the cost to less than $1000 per person.1,2 Knowing that the linear code of DNA determines the structure of the protein “robots” and ribonucleic acids (RNAs) that actually run our cells — and that this structure determines the functions of the proteins and RNAs — the question becomes: How do health care professionals read and make sense of the life code so they can understand the “software” of life in health and disease?
The advent of genomic sequencing has also produced an understanding of single nucleotide polymorphisms often associated with point mutations within a gene that cause specific diseases or disorders.6 Genetic analysis for single — as well as multiple — gene mutations is revolutionizing health care by enabling earlier disease or disorder detection and diagnosis, and advancing treatment for heritable, as well as acquired, conditions. Such information improves preventive efforts and treatment for high-risk patients, possibly resulting in smarter, better and more cost-effective health care.
Since the 1950s, clinicians have known that family health history often points to risk or susceptibility for certain diseases, but oral health professionals lacked the prognostic tools or biomarkers that allow identification of patients at greatest risk for an array of craniofacial and oral diseases or disorders.3–5,7–30 Through government, foundation and industry investment, the human genome was sequenced, single nucleotide polymorphisms were discovered, and a large number of genetic variations or mutations were identified that relate to craniofacial and oral birth defects, as well as chronic human diseases and disorders (including caries, oropharyngeal cancer and periodontal disease).5,7–36
CHALLENGES AND IMPLEMENTATION
Until now, extremely limited access to a patient’s genome content — analogous to peeking through a keyhole — limited clinicians’ view to a few genes and their products. Now, with relatively inexpensive, fast and highly accurate technology, whole-genome sequencing reveals an individual’s entire gene content within hours.1,2 Heralded by advances in cancer diagnostics and therapeutics (including pharmacogenomics), precision health care is a reality — although it’s still in its infancy. As these tools become available, oral health professionals — as an integral part of the interprofessional health care team — should consider embracing genomics to identify patients at risk.10,12,14–26,34–36
For example, traditional diagnoses for periodontal disease are based on the patient’s history (e.g., smoking and oral hygiene), evidence of bacterial infection (often within biofilm), inflammation, pocket probing depth (coupled with radiographs that indicate position and extent of bone loss), tooth mobility, and the presence of specific strains of bacteria.14–16,29,30 In some cases, clinicians also analyze a blood, saliva or crevicular fluid work-up to gain further insight into the patient’s phenotype. In this example, phenotype is the composite of observable and measurable data that include tooth, bone and soft tissue morphologic characteristics, the patient’s developmental and pathogenesis stages, biochemical or physiological properties, and behavioral factors.15 It is accepted that specific bacteria, modified by host and environmental factors, initiate caries and periodontal disease. It’s also known that patients experience significant differences in their rates of disease progression.9–13 Although clinicians recognize that phenotypes result from the expression of an organism’s genes and interactions between genes and the micro- and macro-environments, the current assessment typically stops there. Under the tenets of precision health care, an analysis of genetic information for each patient would be integrated into the phenotype assessment.
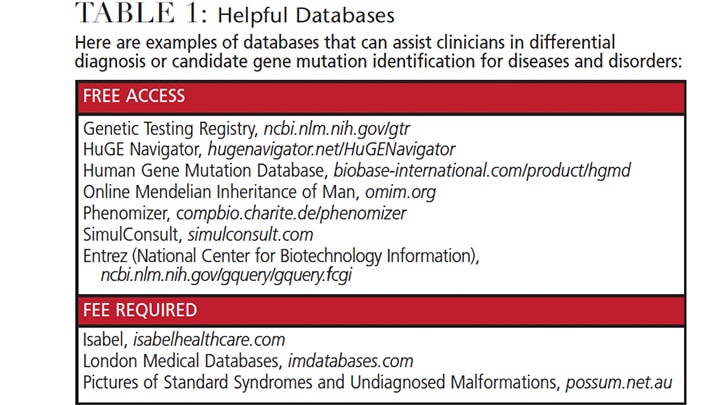
With the goal of improving care and outcomes, oral health professionals should prepare now to provide precision dentistry that utilizes genome-wide sequencing and state-of-the-art analyses.1–5,9–30,34–40 Implementing precision health care into practice is not without challenges, however. It raises the question, for example, of whether clinicians should assess microbial genomic variations (i.e., the oral microbiome) as they relate to disease progression. Also yet to be determined are best practices for accessing and managing the anticipated large genetic and phenotypic data sets. (Table 1 provides a sampling of web-based resources to access data to identify specific diseases and disorders.)
The oral microbiome is central to genomics in dentistry, as an estimated 6 billion microbes representing 700 strains or species, plus spirochetes, reside within the average healthy human oral cavity.5,8,14–16 Oral diseases, such as caries or periodontitis, reflect a bidirectionality between host human genomics and microbial genomics, plus confounding environmental effects, such as diet or smoking. Phenomics is the emerging transdiscipline dedicated to the systematic study of phenotypes on a genome-wide scale at both the DNA and RNA levels. In the future, such information will become increasingly important when counseling patients, communicating with colleagues and making referrals.
Use of genomic screening already enables health professionals to identify and stratify patients at high risk for specific diseases.5,11,13–15,19–21,23–25 The congenital absence of a few teeth is common, for example, and often not associated with other health problems. In some families, however, individuals who lack teeth are at risk for neoplastic changes in the colon. Specifically, mutations in the Axin2 gene causes familial tooth agenesis and predispose individuals to colorectal cancer.14,33 This indicates that a single gene mutation can cause tooth agenesis at one stage of development and cancer at yet another stage.
KEY TAKEAWAYS
- Precision health care tailors treatment to a patient’s specific needs on the basis of genetic, biomarker, epigenetic, phenotypic, and socioeconomic or psychosocial determinants that distinguish an individual from others with similar clinical presentations.
- The goal is to minimize errors in diagnosis, improve outcomes, and avoid unnecessary side effects.
- A sophisticated synthesis of genomics, bioinformatics and digital technology is helping researchers and clinicians understand what makes a specific patient susceptible to disease or responsive to treatment
- The advent of genomic sequencing has produced an understanding of single nucleotide polymorphisms often associated with point mutations within a gene that cause specific diseases or disorders.6
- As new assessment tools become available, oral health professionals — as an integral part of the interprofessional health care team — should consider embracing genomics to identify and stratify patients at risk.10,12,14–26,34–36
FUTURE OPPORTUNITIES
Precision health care is an emerging approach for disease prevention and treatment that accounts for variability in a patient’s genes, environment and lifestyle. Within the next decade, it is likely to positively impact treatment planning, care delivery and outcomes. Understanding and utilizing correlations between genotype, phenotype, environment, psychosocial and socioeconomic determinants will become the new norm. And while early research focused on single gene/single nucleotide mutations associated with disease, ongoing and future research will determine how to use genomic assays when multiple mutations are found in a disease, such as head and neck cancers. This will entail basic, translational, clinical and behavioral studies, as well as implementation science.
The Precision Medicine Initiative introduced by the Obama administration in 2015 seeks to identify new approaches for detecting, measuring and analyzing a wide range of biomedical information, including molecular, genomic, cellular, clinical, behavioral, physiological and environmental parameters. Its mission also includes advancing digital platforms to expand patient-based genetic and phenotype databases. The ultimate goal is to aid accurate and timely diagnoses, and improve treatment and outcomes. Now is the time to prepare oral health professionals, as well as the larger society (through health literacy programs), to embrace the advantages of precision dentistry.
References
- Davies K. The $1,000 Genome: The Revolution in DNA Sequencing and the New Era of Personalized Medicine. New York: Free Press; 2010.
- Collins FS, Hamburg MA. First FDA authorization for next-generation sequencer. N Engl J Med. 2013;369:2369–2371.
- Collins FS. The Language of Life: DNA and the Revolution in Personalized Medicine. New York: HarpersCollins; 2010.
- Venter JC. A Life Decoded: My Genome: My Life. New York: Penguin Group; 2007.
- Slavkin HC, Navazesh M, Patel P. Basic principles of human genetics: a primer for oral medicine. In: Glick M, ed. Burket’s Oral Medicine. 12th ed. Shelton, Conn: People’s Medical Publishing House; 2015:625–652.
- Sachidanandam R, Weissman D, Schnidt SC, et al. A map of human genome sequence variation containing 1.42 million single nucleotide polymorphisms. Nature. 2001;409:928–933.
- Slavkin HC. What the future holds for ectodermal dysplasias: future research and treatment directions. Am J Med Genet A. 2009;149:2071–2074.
- Slavkin HC. Birth of a Discipline: Craniofacial Biology. Newtown, Penn: Aegis Communications; 2012.
- Kornman KS, Duff GW. Personalized medicine: Will dentistry ride the wave or watch from the beach? J Dent Res. 2012;91(Suppl):8s–11s.
- Glick M. Personalized oral health care: Providing “-omic” answers to oral health queries. J Am Dent Assoc. 2012;143:102–104.
- Giannobile WV, Braun TM, Caplis AK, Doucette-Stamm L, Duff GW, Kornman KS. Patient stratification for preventive care dentistry. J Dent Res. 2013;92:694–701.
- Giannobile WV, Kornman KS, Williams RC. Personalized medicine enters dentistry: What might this mean for clinical practice? J Am Dent Assoc. 2013;144:874–876.
- Kornman KS. Diagnostic and prognostic tests for oral diseases: practical applications. J Dent Educ. 2005;69:498–508.
- Slavkin HC. Personalized oral medicine and the contemporary health care environment. In: Polverini PJ, ed. Personalized Oral Health Care: From Concept Design to Clinical Practice. Cham, Switzerland: Springer International Publishing; 2015:1–18.
- Slavkin HC. From phenotype to genotype: enter genomics and transformation of primary health care around the world. J Dent Res. 2014;93(Suppl 1):3s–6s.
- Snead ML, Slavkin HC. Science is the fuel for the engine of technology and clinical practice. J Am Dent Assoc. 2009;140:17s–24s.
- Viera AR. Genomic approaches to disease diagnosis and prevention. In: Polverini PJ, ed. Personalized Oral Health Care: From Concept Design to Clinical Practice. Cham, Switzerland: Springer International Publishing; 2015:19–26.
- Johnson LA, Quintero E. Health information technology (Health IT): the future of personal medicine. In: Polverini PJ, ed. Personalized Oral Health Care: From Concept Design to Clinical Practice. Cham, Switzerland: Springer International Publishing; 2015:27–42.
- D’Silva NJ. Biomarkers for individualized oral cancer therapy. In: Polverini PJ, ed. Personalized Oral Health Care: From Concept Design to Clinical Practice. Cham, Switzerland: Springer International Publishing; 2015:43–60.
- Plonka AB, Giannobile WV. Clinical diagnostics and patient stratification for use in the dental office. In: Polverini PJ, ed. Personalized Oral Health Care: From Concept Design to Clinical Practice. Cham, Switzerland: Springer International Publishing; 2015:61–72.
- Kapila YL. Metabolomics and oral disease diagnosis. In: Polverini PJ, ed. Personalized Oral Health Care: From Concept Design to Clinical Practice. Cham, Switzerland: Springer International Publishing; 2015:73–86.
- Wright JT. Genomics of dental caries and caries risk assessment. In: Polverini PJ, ed. Personalized Oral Health Care: From Concept Design to Clinical Practice. Cham, Switzerland: Springer International Publishing; 2015:87–98.
- Garaicoa-Pazmino C, Decker AM, Polverini PJ. Personalized medicine approaches to the prevention, diagnosis, and treatment of chronic periodontitis. In: Polverini PJ, ed. Personalized Oral Health Care: From Concept Design to Clinical Practice. Cham, Switzerland: Springer International Publishing; 2015:99–112.
- DaSilva AF. The brain as a therapeutic target in TMD and orofacial pain: the next frontier in personalized pain medicine and health technology. In: Polverini PJ, ed. Personalized Oral Health Care: From Concept Design to Clinical Practice. Cham, Switzerland: Springer International Publishing; 2015:113–122.
- Polverini PJ. Preparing the next generation of oral health care professionals for a personalized oral health care environment. Personalized Oral Health Care: From Concept Design to Clinical Practice. Cham, Switzerland: Springer International Publishing; 2015:123–132.
- Edelstein BL. Policy and personalized oral health care. In: Polverini PJ, ed. Personalized Oral Health Care: From Concept Design to Clinical Practice. Cham, Switzerland: Springer International Publishing; 2015:133–144.
- Venter JC. Life at the Speed of Light: From the Double Helix to the Dawn of Digital Life. New York: Penguin Books; 2016.
- Slavkin HC. Gender gap. Dimensions of Dental Hygiene. 2014;12(5):19–22.
- Slavkin HC. Applications of pharmacogenomics in general dental practice. Pharmacogenomics. 2003;4:163–170.
- Slavkin HC. The new genetics: genomes, biofilms, and implications for oral health professionals. Dimensions of Dental Hygiene. 2003;1(1):16–21.
- Slavkin HC. Recombinant DNA technology in oral medicine. Ann NY Acad Sci. 1995;758:314–328.
- Satcher D. Oral Health in America: A Report of the Surgeon General. Available at: profiles.nlm.nih.gov/ps/access/nnbbjv.pdf. Accessed February 2, 2017.
- Lammi L, Arte S, Somer M, et al. Mutations in AXIN2 cause familial tooth agenesis and predispose to colorectal cancer. Am J Hum Genet. 2004;74:1043–1050.
- Collins F, Tabak L. A call for increased education in genetics for dental health professionals. J Dent Educ. 2004;68:807–808.
- Genco RJ, Tabak LA, Tedesco LA, et al. Genetics and its implications for clinical dental practice and education: Report of Panel 3 of the Macy Study. J Dent Educ. 2008;72:86–94.
- Garcia I, Tabak L. A view of the future: dentistry and oral health in America. J Am Dent Assoc. 2009;140(Suppl 1):44S–48S.
- Birkeland AC, Brenner JC. Personalizing medicine in head and neck squamous cell carcinoma: the rationale for combination therapies. Med Res Arch. 2015;3.
- Beachy SH, Olson S, Berger AC. Genomics-Enabled Learning Health Care Systems: Gathering and Using Genomic Information to Improve Patient Care and Research. Availble at: ncbi.nlm.nih.gov/pubmed/25996024. Accessed February 2, 2017.
- National Academy of Sciences, Engineering, and Medicine. Relevance of Health Literacy to Precision Medicine: Proceedings of a Workshop. Available at: nationalacademies.org/hmd/Reports/2016/relevance-of-health-literacy-to-precision-medicine-proceedings.aspx. Accessed February 2, 2017.
- National Academy of Sciences, Engineering, and Medicine. Applying an Implementation Science Approach to Genomic Medicine: A Workshop Summary. Available at: nap.edu/read/23403/chapter/1. Accessed February 2, 2017.
The author has no commercial conflicts of interest to disclose.
Featured photo by COSMIN4000/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. March 2017;3(3):12–14,16.
