

Risk Assessment for Peri-Implantitis
An examination of locally delivered antimicrobials/antibiotics as adjunctive treatment for peri-implant disease.
An examination of locally delivered antimicrobials/antibiotics as adjunctive treatment for peri-implant disease
Implants have become an accepted treatment to replace lost teeth, help increase surface area for chewing, maintain alveolar bone, and restore up to 100% of normal occlusal function.1,2 In an ideal world, this occlusal function and the health of the surrounding hard and soft tissue would remain stable. The reality, however, is that some implants fail. Given rising demand for dental implants and the significant cost and time investment for patients, dental professionals should be well versed in strategies that support implant health.2
Excluding preplacement contributors to implant failure — such as bone quality/quantity, presence of chronic periodontitis or systemic disease, and axial/acentric effects — implant failure is caused by either biomechanical or biological factors.3,4 Biomechanical failures occur due to functional overload, while biological failures are caused by increases in biofilm, inflammation, infection, extruded cement or surgical complications.3 Implant failure most frequently results from the biological factor peri-implantitis, which is an inflammatory cycle that causes increased pocket formation, gingival edema and erythema, leading to destruction of supporting bone.5 Implants are most vulnerable to peri-implantitis and potential failure during the initial 12 months post-placement.3,6 Studies report the prevalence of peri-implant mucositis and peri-implantitis as 19% to 65% and 1% to 47%, respectively.2,3,6–8 This paper will examine the treatment of peri-implantitis with controlled-release drug therapy as an adjunct to mechanical instrumentation.
Proper identification, early diagnosis and effective management of peri-implant disease are necessary to promote successful long-term outcomes. The use of periapical radiographs, accurate measurements of periodontal pocket depth, mobility assessment, and clinical evidence of infection are key to proper treatment. Risk assessment is also essential to preventing dental implant failure. Patients with risk factors — such as diabetes, osteoporosis, past or current smoking, and a history of periodontitis — should be carefully observed throughout implant treatment and follow-up care.9–11
ROLE OF LOCALLY DELIVERED ANTIMICROBIALS/ANTIBIOTICS
When efforts to prevent peri-implantitis are not successful, the use of locally delivered antimicrobials/antibiotics — including chlorhexidine wafers, doxycycline biosorbable gel and minocycline microspheres — can reduce biofilm, thus decreasing the risk of implant failure.2,3,12 In addition to other nonsurgical treatment options, controlled-release drug therapy can help mitigate the need for surgical intervention. Careful consideration of the method of delivery of substances subgingivally to the surface of pure titanium or alloy-derived implants is imperative, as rubbing, combined with an acidic environment, have the potential to corrode the implant’s surface. This was demonstrated in a study by Wheelis et al,13 who subjected pure titanium and the alloy Ti6Al4V to a series of chemical treatments and mechanical abrasion simulating surface decontamination of dental implants. The morphology and roughness of the surface layer before and after treatment with these solutions were investigated using optical and atomic force microscopy. The solutions evaluated are typically used for detoxification of dental implants and included citric acid, 15% hydrogen peroxide, chlorhexidine gluconate, tetracycline, doxycycline, sodium fluoride and peroxyacetic acid. The investigators also examined the effects of a carbon dioxide laser. The treatments consisted of immersion of the samples in solution and rubbing with cotton swabs soaked in solution. The used cotton swabs were analyzed with energy dispersive spectroscopy, which revealed titanium particles on all rubbing samples. In addition, the microscopy investigation showed that corrosion and pitting were present in both metal grades after immersion and rubbing with more acidic solutions (pH < 3).
Scaling and debridement alone may reduce inflammation around implants, but research shows this approach provides only minimal improvement in periodontal pocket depth.2,10 The use of antimicrobials/antibiotics as an adjunct to nonsurgical periodontal therapy can lead to reductions in subgingival periodontal pathogens and decreases in bleeding on probing, periodontal pocket depth and inflammation around implants with peri-implantitis.9,12–16 Surgical interventions to reconstruct bone by reducing inflammation with photodynamic therapy, curettage to remove granulation tissue, and bone augmentation have integrated locally applied antimicrobial/antibiotic therapy to improve outcomes.12,17
Both nonsurgical therapy and surgical intervention for peri-implantitis rely on the reduction of inflammation due to diminished biofilm, detoxification of the implant surface and regeneration of attachment.17 Research has shown that residual cement surrounded by inflammatory cells may not be visible to the unaided eye, but can be found at the scanning electron microscope level around implants. This may support the need for surgical removal of the soft tissues surrounding implants if tissues do not respond to a nonsurgical approach.18 Systematic reviews, randomized controlled trials, and cohort and case-control studies suggest the use of local delivery antimicrobials/antibiotics, in addition to nonsurgical periodontal therapy, is more effective in reducing periodontal pocket depth than scaling and debridement alone.12,15,19–25
Some studies, however, suggest that nonsurgical treatment of peri-implantitis is unpredictable due to the difficulty in fully removing factors that contribute to peri-implant inflammation, as well as the need to rely on patient compliance with self-care.17,26 A Cochrane Database Systematic Review concluded the evidence is insufficient to support one clinical treatment modality as being more effective than another.12 In addition to clinical prevention of infection, recent manufacturing methods have incorporated bacterial pathogen inhibition (in the form of nanocoatings) into implants, with the overarching goal of minimizing pathogenic biofilm. The application of dual-layered silver nanocoating to the surfaces of titanium implants may provide antibacterial effects that last longer than clinical measures.24 While the studies in this review did not deny the effectiveness of the clinical and manufacturing treatment modalities reviewed, they cited the need for improved study design and longer follow-up for documentation of clinical results.12,26
ASSESSMENT
The focus of any peri-implant disease treatment should be improvement in surrounding tissue health.8,11 When assessing an implant, clinicians must differentiate between peri-implant mucositis and peri-implantitis. The former is the presence of inflammation without discernible bone loss, and is similar to gingivitis.27,28 Koldsland et al27 defined peri-implant inflammation as a modified sulcus bleeding index score < 0 and/or bleeding on probing, and bleeding on probing/suppuration with or without the presence of peri-implant bone loss. Peri-implantitis is the presence of discernible radiographic bone loss and inflammation. The degree of peri-implant bone loss, including its relation to the overall length of the implant and load-bearing weight it will carry, should be considered in the diagnosis. These data are important in assessing the potential for successful intervention with a controlled-release antimicrobials/antibiotics as an adjunct to nonsurgical periodontal therapy.27
The possibility of adverse reactions to antimicrobial/antibiotic therapy should be considered during assessment. Individuals with tetracycline or minocycline allergies, pregnant and nursing women, and patients younger than 15 are contraindicated for the doxycycline biosorbable gel and minocycline microspheres. The use of chlorhexidine wafers should be avoided in patients with sensitivity or allergy to chlorhexidine.
INTERDISCIPLINARY COLLABORATION
Prior to treating peri-implantitis with a controlled-release drug therapy, the provider should collaborate with the patient’s attending specialist (if applicable). Comprehensive interdisciplinary collaboration is imperative to ensure the accuracy of patient assessment, establish a history of peri-implant infection and achieve positive outcomes.29 The clinician should confirm when the implant was placed and whether there were postsurgical complications. It will also be necessary to review baseline data to track changes in bleeding on probing, inflammation and probing measurements, as well as obtain periapical radiographs and a medical history. The provider should review the proposed treatment with the patient and obtain informed consent prior to initiating therapy.
IMPLEMENTATION
As noted, there are three types of locally delivered antimicrobials/antibiotics to choose from: chlorhexidine wafers, doxycycline biosorbable gel and minocycline microspheres.
The chlorhexidine wafers contain 2.5 mg of chlorhexidine each and are placed subgingivally with pliers.15 Chlorhexidine is an antiseptic, not an antibiotic, so this approach is well suited for patients with antibiotic allergies. The wafers are indicated for use in pocket depths of 5 mm or greater, in conjunction with scaling and debridement. Providing action against a wide variety of pathogens, chlorhexidine wafers are effective for seven to 10 days, and have been shown to reduce pocket depths.22
Another option is the subgingival application of 10% doxycycline hyclate gel. This product comes with two syringes that are mixed chairside.15 The gel flows freely into the pocket and hardens once exposed to crevicular fluid. The doxycycline is released over seven days, with effects lasting up to six months.15 In conjunction with scaling and debridement, studies show the gel is effective in reducing pocket depths.23,25
Intended for use with a syringe provided by the manufacturer, minocycline microspheres are packaged in single-dose vials consisting of 1 mg minocycline hydrochloride. Generally, each vial is enough to fill one to two 4-mm to 6-mm pockets. The exact dosage depends on size, depth, morphology of the implant, and degree of bone loss. The product comes in powder form and is dispensed from the base of the pocket and extruded until the gingival margin is reached. The microspheres should be used in the treatment of pocket depths ≥ 5 mm. The following case study details the treatment of a patient with peri-implantitis using this technique.
Once the controlled-release drug therapy has been administered, the patient is given postoperative instructions specific to the product administered. The recare interval is once per month for three consecutive months, beginning 30 days posttreatment. At the recare appointment, clinical response to treatment is documented by careful evaluation of bleeding on probing and pocket depth measurements. If clinical evidence of inflammation, bleeding, or a pocket depth of 4 mm or greater exists, treatment with the controlled-release drug regimen should continue until the clinical signs of inflammation are resolved or three consecutive treatment intervals are completed. During the month following the third treatment of the peri-implantitis area, radiographs, pocket depth and bleeding on probing measurements should be recorded.30
Following each treatment appointment, an overview of the care rendered, plans for additional treatment, and outcomes should be reported to the patient’s specialist. Clinicians who closely manage care and work collaboratively with specialists help support patient compliance.29
CASE STUDY
A 58-year-old man presented in an oral surgery practice for a postoperative visit to evaluate the status and health of a previously placed implant #5. His medical history was relatively unremarkable. Review of previous chart notes revealed the extraction of a retained root tip #5, with an associated draining fistula. At the initial visit, Class I molar relationship on both the right and left sides was noted, with a Class II tendency on the left side and a deep bite. After the extraction, a three-month healing time ensued before the implant was placed. Subsequent postoperative examinations revealed integration of the implant with a light contact, no sign of extruded cement, slight inflammation (with bleeding on probing), mild gingival edema on the facial aspect of the implant, and periodontal pockets of 2 mm to 4 mm from both the facial and palatal aspects.
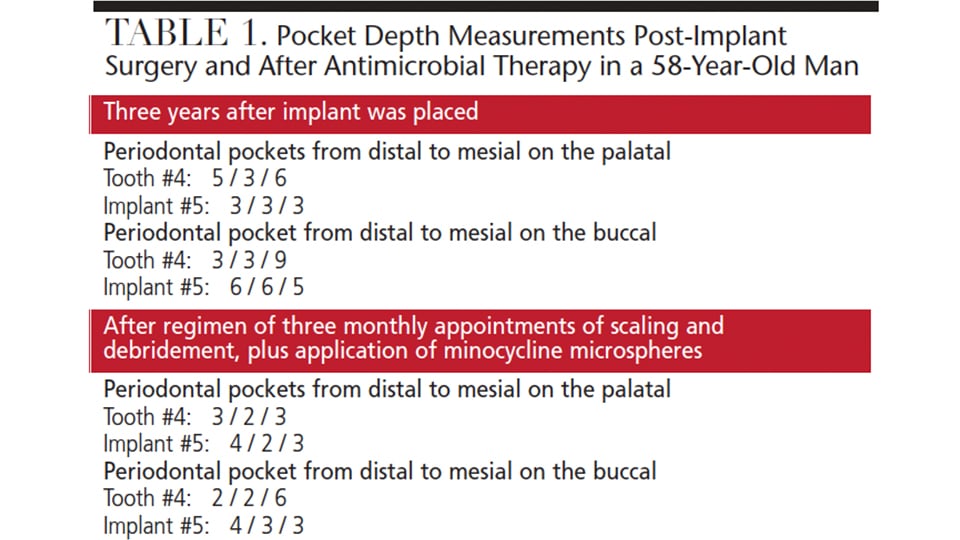
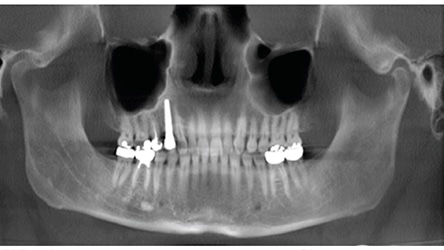
Three years after the final restoration was placed, the patient noted bleeding around the implant when using a rubber tip stimulator. Periodontal pockets were present with bleeding on probing (Table 1). A cone beam computed tomography scan revealed a small radiolucency at the apex of tooth #4 (Figure 1). The periapical radiograph revealed excellent bone-to-implant opposition in area #5, but blunting of the septal bone between the fixture area #5 and tooth #4. Peri-implantitis was diagnosed around implant #5 and periodontal disease around tooth #4.
A treatment plan was proposed and informed consent signed. Both areas were hand scaled with plastic instruments under local anesthesia, and minocycline microspheres were placed subgingivally at both sites. A chlorhexidine mouthrinse was also prescribed.
The patient underwent the recommended treatment plan of three subsequent visits, with hand instrumentation and subgingivally placed minocycline microspheres. Periodontal probing and bleeding points were taken at each visit, with a final postoperative periapical radiograph taken four weeks after treatment was completed. The final evaluation, completed four months later, revealed decreased pocket depths and bleeding points on the mesiopalatal of tooth #4 and distobuccal and distopalatal sites of implant #5. Radiographically, the implant area #5 appeared stable and well integrated.
At subsequent postoperative follow-ups, the patient continued to present with no clinical signs of inflammation or bleeding points, and had periodontal pockets measuring 2 mm or less. In addition, there was radiographic evidence of crestal bone approximating the first thread on the distal and above the implant table on the mesial of the implant.
CONCLUSION
The treatment of peri-implantitis with controlled-release drug therapy as an adjunct to mechanical instrumentation is an effective modality to decrease infection. Reducing biofilm accumulation and inflammation around implant areas decreases the need for surgical intervention and helps support successful implant outcomes.
KEY TAKEAWAYS
- Proper identification, early diagnosis and effective management of peri-implant disease are necessary to promote successful implant outcomes.
- Excluding preplacement factors, implant failure is caused by either biomechanical or biological forces, and most frequently results from peri-implantitis, a biological condition.
- The focus of any peri-implant disease treatment should be improvement in surrounding tissue health.8,11
- Treating peri-implantitis with controlled-release drug therapy as an adjunct to mechanical instrumentation has shown potential clinical benefits.
- Studies suggest the use of locally delivered antimicrobials/antibiotics, in addition to nonsurgical periodontal therapy, is more effective at reducing periodontal pocket depth than scaling and debridement alone.12,15,19–25
- Given rising demand for dental implants, dental professionals should be well versed in strategies that support implant health.2
References
- Maló P1, de Araújo Nobre M, Lopes A, Francischone C, Rigolizzo M. “All-on-4” immediate-function concept for completely edentulous maxillae: a clinical report on the medium (3 years) and long-term (5 years) outcomes. Clin Implant Dent Relat Res. 2012;14 (Suppl 1):e139–e150.
- American Academy of Implant Dentistry. Dental implants facts and figures. Available at: aaid.com/about/press_room/ dental_implants_faq.html. Accessed April 18, 2017.
- Norowski PA Jr, Bumgardner JD. Biomaterial and antibiotic strategies for peri-implantitis: a review. J Biomed Mater Res B Appl Biomater. 2009;88:530–543.
- Porter JA, von Faunhofer JA. Success or failure of dental implants? A literature review with treatment considerations. Gen Dent. 2005;53:423–432.
- Avila-Ortiz G. Encouraging success. Dimensions of Dental Hygiene. 2013;11(5):57–62.
- Schmidlin PR, Sahrmann P, Ramel C, et al. Peri-implantitis prevalence and treatment in implant-oriented private practices: a cross-sectional postal and Internet survey. Schweiz Monatsschr Zahnmed. 2012;122:1136–1144.
- Derks J, Tomasi C. Peri-implant health and disease. A systematic review of current epidemiology. J Clin Periodontol. 2015;42 (Suppl 16):S158–S171.
- Monje A, Aranda L, Diaz KT, et al. Impact of maintenance therapy for the prevention of peri-implant diseases. A systematic review and meta-analysis. J Dent Res. 2016;95:372–379.
- Renvert S, Persson GR. Periodontitis as a potential risk factor for peri-implantitis. J Clin Periodontol. 2009;36 (Suppl 10):9–14.
- Froum S. Supporting implant success. Dimensions of Dental Hygiene. 2012;10(2):19–21.
- Jepsen S, Berglundh T, Genco R, et al. Primary prevention of peri-implantitis: managing peri-implant mucositis. J Clin Periodontol. 2015;42 (Suppl 16):152–157.
- Esposito M, Grusovin MG, Worthington HV. Interventions for replacing missing teeth: treatment of peri-implantitis. Cochrane Database Syst Rev. 2012;1:CD004970.
- Wheelis SE, Gindri IM, Valderrama P, Wilson TG Jr, Huang J, Rodrigues DC. Effects of decontamination solutions on the surface of titanium: investigation of surface morphology composition, and roughness. Clin Oral Implants Res. 2016;27:329–340.
- American Academy of Dental Research. Adjunctive minocycline microspheres decrease periodontal pathogens around implants with peri-implantitis. Available at: iadr.org/AADR/About-Us/News/ArtMID/134369/ArticleID/219/Adjunctive-Minocycline-Microspheres-Decrease160Periodontal-Pathogens-around-Implants-with-Peri-implantitis. Accessed April 18, 2017.
- Paquette DW, Ryan ME, Wilder RS. Locally delivered antimicrobials: clinical evidence and relevance. J Dent Hyg. 2008;82 (Suppl 3):10–15.
- Renvert S, Samuelsson E, Lindahl C, Persson GR. Mechanical non-surgical treatment of peri-implantitis a double-blind randomized longitudinal clinical study. I: clinical results. J Clin Periodontol. 2009;36:604–609.
- Machtei EE, Frankenthal S, Levi G, et al. Treatment of peri-implantitis using multiple applications of chlorhexidine chips: a double-blind, randomized multi-centre clinical trial. J Clin Periodontol. 2012;39:1198–1205.
- Wilson TG Jr, Valderrama P, Burbano M, et al. Foreign bodies associated with peri-implantitis human biopsies. J Periodontol. 2015;86:9–15.
- Hanes PJ, Purvis JP, Gunsolley JC. Local anti-infective therapy: pharmacological agents. A systematic review. Ann Periodontol. 2003;8:79–98.
- Gopinath V, Ramakrishnan T, Emmadi P, Ambalavanan N, Mammen B, Vijayalakshmi. Effect of a controlled release device containing minocycline microspheres on the treatment of chronic periodontitis: A comparative study. J Indian Soc Periodontol. 2009;13:79–84.
- Ahamed S, Jalaluddin M, Khalid I, Moon N, Shaf TK, Ali FM. The use of controlled release locally delivered 10% doxycycline hyclate gel as an adjunct to scaling and root planing in the treatment of chronic periodontitis: clinical and microbiological results. J Contemp Dent Pract. 2013;14:1080–1086.
- Jeffcoat MK, Bray KS, Ciancio SG, et al. Adjunctive use of a subgingival controlled-release chlorhexidine chip reduces probing depth and improves attachment level compared with scaling and root planing alone. J Periodontol. 1998;69:989–997.
- Garrett S, Johnson L, Drisko CH, et al. Two multi-center studies evaluating locally delivered doxycycline hyclate, placebo control, oral hygiene, and scaling and root planing in the treatment of periodontitis. J Periodontol. 1999;70:490–503.
- Paquette DW, Oringer R, Lessem J, et al. Locally delivered minocycline microspheres for the treatment of periodontitis in smokers. J Clin Periodontol. 2003;30:787–794.
- Wennström JL, Newman HN, MacNeill SR, et al. Utilization of locally delivered doxycycline in non-surgical treatment of chronic periodontitis. A comparative multi-centre trial of 2 treatment approaches. J Clin Periodontol. 2001;28:753–761.
- Besinis A, Hadi SD, Le HR, Tredwin C, Handy RD. Antibacterial activity and biofilm inhibition by surface modified titanium alloy medical implants following application of silver, titanium dioxide and hydroxyapatite nanocoatings. Nanotoxicology. 2017;11:327–338.
- Koldsland OC, Scheie AA, Aass AM. Prevalence of peri-implantitis related to severity of the disease with different degrees of bone loss. J Periodontol. 2010;81:231–238.
- Zitzmann NU, Berglundh T. Definition and prevalence of peri-implant diseases. J Clin Periodontol. 2008;35 (Suppl 8):286–291.
- Vanderbilt AA, Isringhausen KT, Bonwell PB. Interprofessional education: the inclusion of dental hygiene in health care within the United States — a call to action. Adv Med Educ Pract. 2013;4:227–229.
- Ghahroudi RA, Talaeepour A, Mesgarzadeh A, et al. Radiographic vertical bone loss evaluation around dental implants following one year of functional loading. J Dent (Tehran). 2010;7:89–97.
The authors have no commercial conflicts of interest to disclose.
FEATURED IMAGE BY DANIELZGOMBIC/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. May 2017;3(5):28—31.
