

Restorative Dentistry in the Primary Dentition
Selecting the right material for the right situation will help ensure optimal function, longterm performance and esthetics.
Selecting the right material for the right situation will help ensure optimal function, long-term performance and esthetics
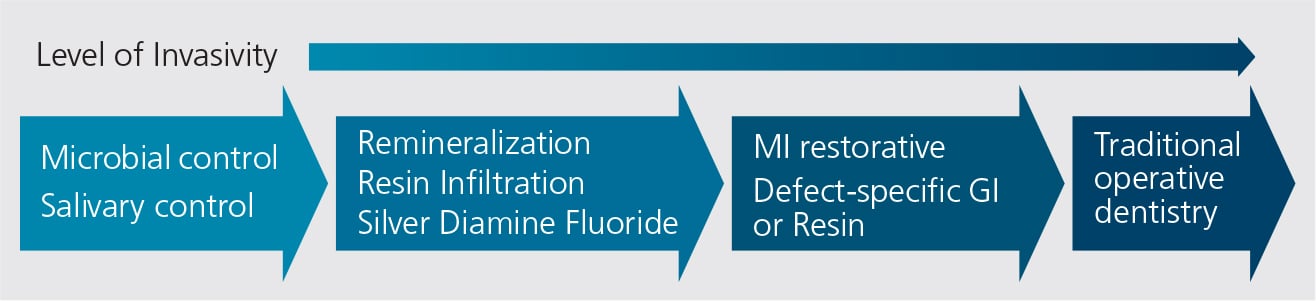
The practice of dentistry for children requires extensive knowledge and understanding of restorative materials and techniques. Restorative procedures should be the last approach in managing caries; unfortunately, is often the first step. The progressive philosophy in today’s caries management continuum (Figure 1) is managing biofilm and demineralization, and taking a proactive therapeutic approach in the early stages of caries lesion development. The later stages include minimally invasive restoration, followed by traditional operative dentistry. This paper will discuss various aspects of restorative dentistry for children, and some common techniques in caring for primary teeth.
While early lesions may be detected clinically or radiographically, or by the newer caries detection tools, only clinicians can synthesize all the information, and make the decision to restore the tooth. Prior to the restorative procedure, it is important to distinguish the diagnosis of caries or other need for restoration. Dental charts commonly contain only information about what restorations were performed — with the assumption there must have been a caries lesion, but without specific delineation and determination of the diagnostic component prior to engaging in restorative dentistry. Clinicians should carefully document the method and basis of the diagnosis or other justification for restoration, such as trauma or hypomineralization/hypocalcification, as well as the extent and depth of the lesion requiring restoration. Although it may seem routine and mundane, this diagnostic documentation is essential in order to provide the best quality care, and to ensure treatment is justified based on diagnostic determinations.
ISOLATION TECHNIQUES
Prior to restorative dentistry for children, proper isolation is essential. The surgical environment should be isolated from potential contaminants. This will also protect the patient from swallowing or inhaling materials, water or other contaminants during the procedure. Additionally, all restorative materials have some technique sensitivity, and contamination with moisture, water, saliva or other debris could affect retention and, thus, long-term outcomes. This is particularly true for composites resins, but also applies to the more moisture-tolerant glass ionomer materials.
A rubber dam is the preferred isolation technique. It provides excellent isolation and visualization during the procedure, and it also serves as a behavior management tool. It is worth taking the time to train the team to place dental dams. A properly trained staff will enjoy the opportunity to place dams and be part of the team delivering care in the best possible manner.1
Although a dam is recommend for each pediatric restorative procedure, there may be circumstances, such as partially erupted teeth, in which the patient cannot tolerate a dam. In situations in which it is believed that contamination will not be a factor (permanent anterior teeth, for example), alternative isolation techniques can be used — including devices that provide light, suction and physical isolation from contaminants. These devices are also useful for shorter procedures, such as sealant placement.
GLASS IONOMER
Glass ionomer is a salt created by a chemical reaction between a polyalkenoic acid and an aluminum-containing glass powder. The glass powder includes fluoride so the latter can be released — and recharged — after restoration with glass ionomer. This is the only material used in restorative dentistry that chemically bonds to tooth structure.2 Because the glass ionomer bonds to calcium ions in dentin and enamel, it bonds independently of the morphology of the dentin surface, which can vary from patient to patient and tooth to tooth. Other materials, such as composites, require a specific morphological structure of the intertubular dentin in order to create the so-called hybrid layer that allows the composite to adhere to the tooth substrate.
Additionally, glass ionomer contains water. Combined with its chemical bonding to tooth structure, this makes it biocompatible and somewhat moisture tolerant. Glass ionomer cannot be placed in a “fully wet” environment in which there is excess water or saliva. In situations in which there is humidity, but not a visible “thickness of fluid,” glass ionomer is useful and can easily be bonded to the tooth substrate. By comparison, resin sealants, as well as resin composites, are not as moisture tolerant.
Because glass ionomer restorations release fluoride, they can be beneficial in preventing recurrent decay around the margins of restorations. They can also prevent adjacent structures from demineralizing when subject to acidic attack.
Clinicians commonly encounter situations in which the proximal surface of a primary tooth shows a small caries lesion, but there is also decay on the approximal surface that is not detected radiographically. In these cases, it is logical to assume that whatever forces allow the caries lesion to form where it is radiographically visualized also act on the adjacent approximal surface, causing demineralization not yet perceptible via bitewing radiography. Placing glass ionomer in the lesion obviously requiring restoration will also provide the possibility of remineralization of the adjacent surface.3
It is reasonable to suggest that using glass ionomer as a healing material for adjacent structures will become more prevalent as newer technologies emerge that allow visualization of lesions at a very early stage. The ability of glass ionomer to remineralize adjacent lesions is an advantage that no other material possesses.4
COMPOSITE RESTORATIONS
Composite materials are commonly used for pediatric restorations. In a scenario in which a cooperative child, ideal isolation, and adequate time for the procedure all exist, a resin composite should be used. Composite is the strongest material within the armamentarium of intracoronal direct restoratives, and is also the most esthetic. In addition, new devices are available that facilitate composite placement; these includes systems for restoring primary molars that provide simultaneous wedging and banding during placement in interproximal situations (Figures 2A through 2C).

When a composite’s technique sensitivity and moisture intolerance do not allow it to be placed properly — perhaps due to issues stemming from cooperation, isolation or time — an alternative material, such as glass ionomer or resin-modified glass ionomer, should be used. The advantages of glass ionomer and resin-modified glass ionomer are many, and the fact that several materials have emerged (and more will be emerging over the next year or two) support the discussion that, together with composites, glass ionomer will continue to play an important role in restorative dentistry for children.5
Key Takeaways
- The continuum of caries management philosophy (Figure 1) dictates that clinicians manage biofilm and demineralization, and implement other steps to arrest caries lesions during the early stages of their development.
- Lesions that are addressed in the later stages should be treated with minimally invasive restoration, followed by traditional operative or restorative dentistry.
- Early caries lesions may be detected clinically or radiographically, or by newer caries detection tools — but only clinicians can synthesize all the information and decide to go forward with a restorative procedure.
- Proper isolation (e.g., the use of rubber dams) is essential prior to restorative pediatric dentistry.
- Achieving the best combination of function, esthetics and performance hinges on choosing the right material for the right situation.
STAINLESS STEEL CROWNS
Stainless steel crowns (SSCs) are another commonly used restorative solution. There is significant literature demonstrating that extracoronal coverage is helpful in primary teeth with extensive caries.6 Besides protecting the tooth from additional decay and infection, SSCs prevent lesion progression and leakage, and allow the tooth to remain until natural exfoliation. Consequently, they are indicated for children with high decay rates, patients with multiple lesions, and in younger children where longevity is needed before exfoliation. They can also be used when isolation presents challenges, or when children are being treated under general anesthesia due to their precooperative or uncooperative presentation.
Conversely, SSCs might be contraindicated when the decay rate is low or only one tooth is effected, or in cooperative children whose lesions can be restored with intracoronal restorations.
Multiple steps are involved in placing SSCs. After a local anesthetic is delivered, a dental dam is placed. Following isolation, the tooth’s occlusal surface is reduced to the extent necessary (generally, 1.0 to 1.50 mm) to create space for the crown and cement. This reduction should follow the original contour of the occlusal surface (Figure 3). In creating interproximal separation, clinicians must take crown thickness into account. This generally requires reductions of 1 mm or more so an explorer can pass through the proximal space (Figure 4). When SSCs are placed adjacent to primary molars, the reduction for each crown must be made as if they were placed independently.



Finally, buccal and lingual bevels are placed, extending from the occlusal surface onto the respective buccal and lingual surfaces. These long bevels, generally at a 45-degree angle, will allow reduction of the buccal and lingual surfaces without removing the important buccal and lingual bulges present in primary molars. These bulges are essential for the retention of the crown as its “snaps” over these surfaces during placement. After smoothing the preparation, a crown is selected based on the mesio-distal size of the tooth. Once the crown is fitted, contoured and crimped, it can be cemented, generally with glass ionomer cement (Figure 5).
ESTHETIC CROWNS FOR PRIMARY TEETH
Restoring the esthetic form and function of caries-affected primary anterior teeth presents unique challenges. While it is unclear whether less esthetic restorations in primary anterior teeth have negative psychosocial impact on children, an increased demand is evident among parents and caregivers for esthetic pediatric restorations.7,8 Though many options have been proposed to address this concern, strong evidence of efficacy or superiority of any particular technique or option is still lacking. Intracoronal tooth-colored restorations, including glass ionomer, resin-modified glass ionomer, or composite, can be considered.9 In addition, full-coverage restorations — such as composite resin strip crowns, preveneered SSCs, and the newly introduced prefabricated primary zirconia crowns — may be used to achieve optimal esthetics and retention.9 Each of these techniques has its advantages and limitations.
Both Class V and Class III restorations can be placed on primary anterior teeth. While Class V restorations are relatively easy to place and usually provide good retention, Class III restorations in primary anterior teeth are among the most technique-sensitive procedures a pediatric dentist performs. A conservative preparation may be indicated due to small crown size and close proximity of the pulp horns to the interproximal surfaces. Clinicians must also take into account that slot preparations could result in less than ideal retention because of the small area for etching and bonding,10 Studies comparing Class III slot preparations with dovetail preparations have demonstrated no clinically significant differences between two designs.11,12 Besides preparation, the material placement can be also challenging in terms of isolation, and moisture and hemorrhage control.
According to guidelines from the American Academy of Pediatric Dentistry,9 full coverage coronal restorations are indicated when:
- Decay is present on multiple surfaces
- An incisal edge is involved
- There is extensive cervical decalcification
- Pulpal therapy is indicated
- The caries lesion is small, but oral hygiene is poor
- Patient behavior makes moisture control or precision preparations difficult to achieve
COMPOSITE STRIP CROWNS
Among esthetic full-coverage restorations in primary anterior teeth, the use of the composite “strip crowns” (CSCs) has the longest history. A survey among pediatric dentists showed that 46% of respondents chose CSCs as their first choice for full-coverage restorations of primary anterior teeth.13 Retrospective studies indicate that overall retention of CSCs ranges from 49% to 80%.14–17 Lower retention rates were noted in children following dental rehabilitation under general anesthesia, possibly due to the greater propensity for developing new and recurrent caries in this high-risk population.17 In spite of high parental satisfaction with CSCs, durability is most likely to cause concerns among parents/caregivers.18,19 Parental dissatisfaction was also noted regarding color changes.14,18 Instead of composite, some practitioners have suggested using resin-modified glass ionomer as an interim restorative material for CSCs when ideal isolation is not possible.20
Occlusion and the extent of the lesion should likewise be considered when placing CSCs. Leaving adequate tooth structure during preparation will ensure sufficient surface area for bonding. Low retention rates have been seen in teeth with decay in three or more surfaces.16 In addition, due to high probability of resin fracture, CSCs should be avoided in patients with anterior crossbites or severe bruxism.
PREVENEERED STAINLESS STEEL CROWNS
Although SSCs may be the most durable restoration for primary anterior teeth with large lesions, they are not esthetically acceptable to many parents. Open-face SSCs were introduced to improve the appearance of SSCs by removing the metal facing after cementation and replacing it with a tooth-colored material.21 Placement of these crowns is technically challenging and time consuming, however.
Preveneered SSCs (PVSSCs) were introduced approximately 20 years ago. In a survey by Oueis et al, 41% of respondents selected PVSSCs as their first choice for restoring primary anterior teeth.13 Esthetically pleasing, the crowns earn high levels of parental satisfaction.22–24 Unlike SSCs, the fitting of PVSSCs should be passive, as any forceful placement or excessive pressure could cause the white facing to break, crack or chip.7 Only slight crimping of the lingual surface should be used for margin adaption and retention, but minimal adjustment of the lingual margin does not seem to decrease facial veneer facture resistance.25 Several retrospective studies have demonstrated the high retention rates of PVSSCs.22,23,26,27 The biggest issues with these crowns are fracture and loss of some, or all, of the veneer — which is challenging to repair.22,23,24 Consequently, PVSSCs should also be avoided in patients with anterior crossbites or where occlusion precludes their use.
ZIRCONIA CROWNS

Recently, prefabricated zirconia crowns have become available in various sizes to fit every primary tooth. Some brands also offer a narrower version of canines and first primary molars for patients with space loss or crowding. These monolithic crowns are made of solid zirconia, so there is virtually no possibility of facial veneer fracture.28,29 Concerns over zirconia crowns include an inability to manipulate the margin to create an ideal seal, and the need for additional tooth reduction (leading to possible pulpal exposure) while still leaving enough tooth structure for retention. Other considerations include cost and the learning curve in placing zirconia. Currently, there is little information on their long-term clinical performance. Yet these crowns show high parental satisfaction19 and are likely to become more popular.30–32 The single prospective study available has a six-month follow-up period. In this short trial, zirconia crowns demonstrated a 100% success rate, while 22% of CSCs experienced either fracture or complete loss, and 5% of the PVSSCs lost a portion of the veneer.29 In evaluations of gingival health, zirconia crowns showed improved health, while the other crowns showed increased gingival inflammation.29 This may possibly be attributed to the highly polished surfaces and biocompatibility of zirconia crowns.32 Opposing tooth wear was noted in four out of 38 zirconia crowns studied.29
FUTURE DIRECTIONS
While many options exist for esthetic restorations in primary anterior teeth (Figures 6A through 6C), to date, very little controlled clinical data are available to suggest that one type is superior to the others. Clinical decisions regarding the choice of restoration and the ultimate outcome are dictated by the extent of decay, moisture and hemorrhage control, and the child’s level of cooperation, as well as caries risk, parental desires, and the clinician’s experience and preferences.32,33
Many new materials and techniques are available to dentists who treat children. Ultimately, clinicians can ensure the optimal combination of function, long-term performance and esthetics by selecting the right material for the right situation. Doing so will help set pediatric patients on a lifetime course of improved oral and systemic health.
References
- Dhar V, Hsu KL, Coll JA, et al. Evidence-based update of pediatric dental restorative procedures: Dental materials. J Clin Pediatr Dent. 2015;39:303–310.
- Uribe S. Which filling material is best in the primary dentition? Evid Based Dent. 2010;11:4–5.
- Rodrigues E, Delbem AC, Pedrini D, Cavassan L. Enamel remineralization by fluoride-releasing materials: proposal of a pH-cycling model. Braz Dent J. 2010;21:446–451.
- Donly KJ, Henson T. Glass ionomer cement restorations for contemporary pediatric dentistry. Alpha Omegan. 2005;98(4):21–25.
- Aykut-Yetkiner A, Simşek D, Eronat C, Ciftçioğlu M. Comparison of the remineralisation effect of a glass ionomer cement versus a resin composite on dentin of primary teeth. Eur J Paediatr Dent. 2014;15:119–121.
- American Academy of Pediatric Dentistry. Guideline on Restorative Dentistry, revised 2014. Available at: aapd.org/media/Policies_Guidelines/ G_Restorative.pdf. Accessed August 15, 2016.
- Waggoner WF. Restoring primary anterior teeth: Updated for 2014. Pediatr Dent. 2015;37:163–170.
- Woo D, Sheller B, Williams B, Mancl L, Grembowski D. Dentists’ and parents’ perceptions of health, esthetics, and treatment of maxillary primary incisors. Pediatr Dent. 2005;27:19–23.
- Committee O. Guideline on restorative dentistry. Pediatr Dent. 2015;37:232–243.
- Piyapinyo S, White G. Class III cavity preparation in primary anterior teeth: In vitro retention comparison of conventional and modified forms. J Clin Pediatr Dent. 1998;22:107–112.
- Trairatvorakul C, Piwat S. Comparative clinical evaluation of slot versus dovetail Class III composite restorations in primary anterior teeth. J Clin Pediatr Dent. 2004;28:125–129.
- Rathnam A, Nidhi M, Shigli AL, Indushekar K. Comparative evaluation of slot versus dovetail design in class III composite restoations in primary anterior teeth. Contemp Clin Dent. 2010;1:6–9.
- Oueis H, Atwan S, Pajtas B, Casamassimo PS. Use of anterior veneered stainless steel crowns by pediatric dentists. Pediatr Dent. 2010;32:413–416.
- Kupietzky A, Waggoner WF, Galea J. The clinical and radiographic success of bonded resin composite strip crowns for primary incisors. Pediatr Dent. 2003;25:577–581.
- Kupietzky A, Waggoner WF, Galea J. Long-term photographic and radiographic assessment of bonded resin composite strip crowns for primary incisors: results after 3 years. Pediatr Dent. 2005;27:221–225.
- Ram D, Fuks AB. Clinical performance of resin-bonded composite strip crowns in primary incisors: A retrospective study. Int J Paediatr Dent. 2006;16:49–54.
- Tate AR, Ng MW, Needleman HL, Acs G. Failure rates of restorative procedures following dental rehabilitation under general anesthesia. Pediatr Dent. 2002;24:69–71.
- Kupietzky A, Waggoner WF. Parentral satisfaction with bonded resin composite strip crowns for primary incisors. Pediatr Dent. 2004;26:337–340.
- Salami A, Walia T, Bashiri R. Comparison of parental satisfaction with three tooth-colored full-coronal restorations in primary maxillary incisors. J Clin Pediatr Dent. 2015;39:423–428.
- Nelson T. An improved interim therapeutic restoration technique for management of anterior early childhood caries: report of two cases. Pediatr Dent. 2013;35:124–128.
- Wiedenfeld KR, Draughn RA, Welford JB. An esthetic technique for veneering anterior stainless steel crowns with composite resin. ASDC J Dent Child. 1994;61:321–326.
- Shah PV, Lee JY, Wright JT. Clinical success and parental satisfaction with anterior preveneered primary stainless steel crowns. Pediatr Dent. 2004;26:391–395.
- Roberts C, Lee JY, Wright JT. Clinical evaluation of and parental satisfaction with resin-faced stainless steel crowns. Pediatr Dent. 2001;23:28–31.
- Champagne C, Waggoner W, Ditmyer M, Casamassimo PS, MacLean J. Parental satisfaction with preveneered stainless steel crowns for primary anterior teeth. Pediatr Dent. 2007;29:465–469.
- Gupta M, Chen J-W, Ontiveros JC. Veneer retention of preveneered primary stainless steel crowns after crimping. J Dent Child (Chic). 2008;75:44–47.
- MacLean JK, Champagne CE, Waggoner WF, Ditmyer MM, Casamassimo P. Clinical outcomes for primary anterior teeth treated with preveneered stainless steel crowns. Pediatr Dent. 2007;29:377–381.
- Lopez-Loverich A, Garcia M, Donly KJ. Retrospective study of retention of stainless steel crowns and preveneered crowns on primary anterior teeth. Pediatr Dent. 2015;37:530–534.
- Manicone PF, Rossi Iommetti P, Raffaelli L. An overview of zirconia ceramics: basic properties and clinical applications. J Dent. 2007;35:819–826.
- Walia T, Salami AA, Bashiri R, Hamoodi OM, Rashid F. A randomised controlled trial of three aesthetic full-coronal restorations in primary maxillary teeth. Eur J Paediatr Dent. 2014;15:113–118.
- Planells del Pozo P, Fuks AB. Zirconia crowns — an esthetic and resistant restorative alternative for ECC affected primary teeth. J Clin Pediatr Dent. 2014;38:193–195.
- Croll T, Donly KJ. Contralateral/Opposite-arch zirconia crown restoration of two mandibular primary first molars. Insid Dent. 2015;11:78–81.
- Ashima G, Sarabjot KB, Gauba K, Mittal HC. Zirconia crowns for rehabilitation of decayed primary incisors: an esthetic alternative. J Clin Pediatr Dent. 2014;39:18–22.
- Waggoner WF. Anterior crowns for primary anterior teeth: an evidence based assessment of the literature. Eur Arch Paediatr Dent. 2006;7:53–57.
The authors have no commercial conflicts of interest to disclose.
From Decisions in Dentistry. September 2016;2(09):28–32.
