
Prosthetic Retention Options for Dental Implants
When placing implant restorations, clinicians must choose between cement- or screw-retained techniques.
When placing implant restorations, clinicians must choose between cement- or screw-retained techniques
The advent of dental implants has brought new solutions for tooth loss, which for many patients has provided quality-of-life improvements that were never before possible.1–3 At the same time, the use of these devices has also brought new challenges, including technical and biological complications — such as screw loosening, component fractures,4–7 and new diseases, such as peri-implantitis8–11 While dental implant procedures continue to evolve, we should look at the past and evaluate how success relates to the treatment options chosen.
Initially, implants were restricted to the mandible, with functional-based prostheses connected solely by screw joints to the implant body, and implant placement predicated by the available bone. Prior to the concept of restoration-driven implant placement, planning was predominantly based on the surgical site.12–14 With this development, now implant location, angulation and depth were codirected by considerations related to the restoration, as well as bone anatomy. As implant placement progressed to include single missing teeth, esthetics became a growing concern. With this, the restorative options evolved to include cemented restorations. Now, esthetics, control of the occlusion, and techniques more familiar to traditional dentistry became available.15,16
The era of cemented implant restorations presented both advantages and disadvantages. Early issues included the predictable removal of the restoration in case clinicians needed to access the implant abutment screw — something that was never an issue with screw-retained restorations. This resulted in polarization of cementation principles, such as choosing between permanent or provisional cement. It also led to the development of implant-specific cements.17 Several years after the introduction of the cemented restoration, clinicians began to report concerns over residual, excess cement and peri-implant disease.18,19 Initially, these were restricted to case reports, but then a positive link was established between peri-implant disease and residual cement.20 Not only did Wilson prove an association between excess cement and diseased implants, the discovery that removing this foreign material brought resolution in many cases added further support to the study. Systematic reviews cite an increase in biological problems with cement-retained restorations, and several studies have now indicated likely etiological factors. Many of the problems related to residual cement around implants stem from the transfer of materials and techniques dentistry has been using on the natural dentition for close to 100 years. This must be considered an error, as teeth and implants are very different.21
The biological attachment of a dental implant (both soft and hard tissue) is considerably different from the natural tooth. The soft tissues around the implant attach by a weak hemi-desmosomal attachment — considered more of an adhesion than a true connection. The lack of fiber bundle insertion into the implant (due to the lack of cementum for these fibers to anchor), as well as the sulcus of the implant having low reparative capabilities, high permeability and not being keratinized (the converse is true for the healthy tooth), all make this a vulnerable site. Trauma to this site can effectively disrupt the fragile connection, and has been seen to occur with techniques such as packing retraction cord — something that is routinely done around natural teeth with little damage (assuming the correct technique is used).





Dental luting cements also play a major role in the peri-implant disease process. If it is understood that cement extrusion into the peri-implant soft tissues can, and does, occur, it would seem prudent to use cements that are easily identified and removed.22 Unfortunately, many cements have low radiopacity, and are colored to reflect the soft tissue esthetics; they’re also highly adhesive, which increases the likelihood of cement retention. Cements not only attach to the implant and restoration, they have also been seen incorporated within the soft tissues. Cement particles have been identified in several studies that evaluated soft tissue human biopsies. Although it may seem difficult to understand how cements can inoculate the soft tissues, dentistry is familiar with this concept when one sees an amalgam tattoo — a condition resulting in metal fragments within the tissues.23,24
Other problems with cements include technique, as there is little, if any, information regarding cement placement techniques to optimize cement flow.
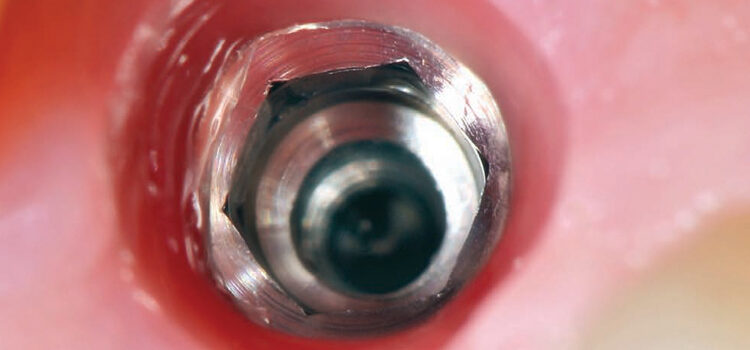
In addition, some dentists may not understand how much cement is required, and this, coupled with a variety of available abutment designs, has led to multiple reports of excess cement being an issue. Newer implant abutment designs will likely fuel the issue, as narrower, deeper implant placement increases in popularity. These cases will make access to cement extrusion and removal of excess material even more challenging. (Figures 1A and 1B, and Figures 2A through 2C).
key takeaways
- There is no single solution to the restoration of the dental implant. Cementation and screw-retention methods both have merit.
- With cemented implant restorations, clinicians need to carefully remove excess cement in order to minimize the risk of peri-implant disease.
- Placing the crown margin as superficially as possible, even supragingivally, also helps limit excess cement extrusion, and allows easier access for removal.27
- Screw-retained implant restorations can be readily made esthetic, and clinicians can control the occlusion equally as well as in cemented restorations.
SCREW-RETAINED TECHNIQUE
Screw retention of implant prosthetics is also not without issues. Dealing with closure of the screw access channel is a concern, especially in highly esthetic sites, or when the patient has high demands. Adequate support for the crown material, and how this relates to the screw hole, contact point issues with adjacent teeth, or restorations not aligning with the anti-rotation features of the implant, all require considerable planning in order not to compromise the site. Many of these issues can be overcome, however, with modern dental laboratory techniques and skilled surgical planning and implant placement.25
Screw-retained implant restorations can be readily made esthetic, and clinicians can control the occlusion equally as well as in cemented restorations (Figures 3A and 3B).


crown. Once seated in the patient’s mouth,
this plug is bonded using porcelain bonding
techniques to cover the screw access
channel.
a lubricant to hold the polytetrafluoroethylene
(PTFE or plumber’s tape) material.
Likewise, cemented restorations can be made to perform well and limit the risk of cement extrusion. Abutment design can be easily altered, and, if desired, the cement margin site controlled.26
Abutment modifications include the use of internal venting, which means that instead of the screw access channel being obliterated prior to cementation, a space is maintained to allow excess cement to flow internally. Retaining as much cement as possible within the system not only reduces excess extrusion, it also alters the crown’s retentive capabilities — in other words, it takes more force to remove the crown. This allows for softer, more manageable cements to be used, but boosts their performance.
Placing the crown margin as superficially as possible, even supragingivally, also helps limit excess cement extrusion, and allows easier access for removal.27 Studies have indicated that cement margins as shallow as 1 mm will result in there being at least some residual cement.28
When cement margins are placed supragingivally in nonesthetic sites, these are generally well accepted — provided the patient is informed prior to receiving the final restoration. If the patient’s demands are such that a more esthetic restoration is required, a custom abutment that incorporates a porcelain supragingival margin can be fabricated. Many pressed porcelain systems are available, and these allow restorations to be wax invested; next, using the lost-wax technique, porcelain is heated and injected within the invested mold.
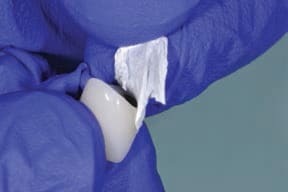
Another means of reducing the risk of cement extrusion is to protect the soft tissues. While rubber dams can seldom be used (due to the thickness of the material), polytetrafluoroethylene (PTFE or plumber’s tape) can be easily sterilized and placed around the abutment to form a bib. Care must be taken with this procedure not to allow this material to get caught in the connection between the implant and abutment.
COPY ABUTMENT TECHNIQUE
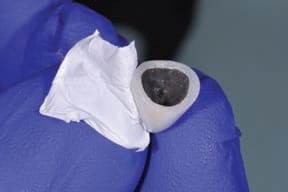
Techniques can also be employed to control the amount of cement used. One documented method is to fabricate a disposable “copy abutment” (Figure 4A through 4H).29 This technique uses a polyvinyl siloxane impression or bite material in conjunction with a spacer. The spacer the author uses is PTFE, as it has a thickness of approximately 50 microns (a dimension that’s similar to that allowed for cement during crown fabrication); this is generally known as relief space or a die spacer. A layer of petroleum jelly or water-soluble lubricant is first painted into the intaglio of the crown, as this helps the PTFE to adapt and stick to the walls of the restoration. In this technique, PTFE is placed in the form of a single layer against the walls of the crown or bridge.


until a handle is produced.
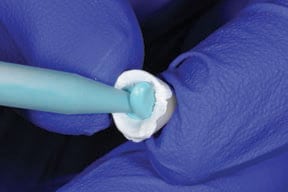
The fast-setting bite or impression material is then injected into the restoration and beyond the margins, so as to produce a handle — this will become the copy abutment. Once set, the copy abutment is removed and the PTFE is discarded; next, the intaglio of the crown is thoroughly washed and cleaned to remove all traces of the lubricant. The copy abutment is inspected and should conform to the crown — yet, compared to the intaglio of the crown, it is 50 microns smaller in all dimensions. The crown (or bridge) is then loaded with cement. The copy abutment is pushed into the cement and seated. Excess cement is thus extruded extraorally, while the restoration has a layer of cement approximately 50 microns thick within the crown (or bridge). Any excess cement on the external surface of the restoration can be quickly removed. The crown (or bridge) is seated with minimal extrusion of cement, as this has already essentially occurred. This expedites cleanup and minimizes the extrusion of excess cement.



CONCLUSION
Overall, there is no single solution to the restoration of the dental implant. Both cementation and screw-retention methods have merit. The conscientious clinician will have a good understanding of the advantages and disadvantages of each method, and make decisions based on what is best for the patient.
In the author’s opinion, most, if not all, posterior maxillary and mandibular implants can be placed by a well-trained surgeon in an ideal position to allow for screw-retained restorations. In the anterior, this is far more challenging. The premaxilla angulation and anatomy of the anterior mandible often preclude screw-retained restorations, so, here, the likely best option is a cement-retained solution.
References
- George LK, Bearon LB. Quality of life in older persons: Meaning and measurement. New York: Human Science Press, 1980.
- Awad MA, Locker D, Korner-Bitensky N, Feine JS. Measuring the effect of intra-oral implant rehabilitation on health-related quality of life in a randomized controlled clinical trial. J Dent Res. 2000 Sep;79(9):1659–1663.
- Feine JS, Carlsson GE, Awad MA, Chehade A, Duncan WJ, Gizani S. The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. Gerodontology. 2002 Jul;19(1):3–4.
- Shim HW, Yang BE. Long-term cumulative survival and mechanical complications of single-tooth Ankylos Implants: focus on the abutment neck fractures. J Adv Prosthodont. 2015 Dec;7(6):423–430.
- Bacchi A, Regalin A, Bhering CL, Alessandretti R, Spazzin AO. Loosening torque of Universal Abutment screws after cyclic loading: influence of tightening technique and screw coating. J Adv Prosthodont. 2015 Oct;7(5):375–379.
- Katsuta Y, Watanabe F. Abutment screw loosening of endosseous dental implant body/abutment joint by cyclic torsional loading test at the initial stage. Dent Mater J. 2015;34(6):896–902.
- Theoharidou A, Petridis HP, Tzannas K, Garefis P. Abutment screw loosening in single-implant restorations: a systematic review. Int J Oral Maxillofac Implants. 2008 Jul-Aug;23(4):681–690.
- Pesce P, Canullo L, Grusovin MG, de Bruyn H, Cosyn J, Pera P. Systematic review of some prosthetic risk factors for periimplantitis. J Prosthet Dent. 2015 Sep;114(3):346–350.
- Hsu YT, Mason SA, Wang HL. Biological implant complications and their management. J Int Acad Periodontol. 2014 Jan;16(1):9–18.
- Esposito M, Hirsch JM, Lekholm U, Thomsen P. Biological factors contributing to failures of osseointegrated oral implants. (II). Etiopathogenesis. Eur J Oral Sci. 1998 Jun;106(3):721–764.
- Mombelli A, Lang NP. The diagnosis and treatment of peri-implantitis. Periodontol 2000. 1998 Jun;17:63–76.
- Brånemark PI. Osseointegration and its experimental background. J Prosthet Dent. 1983 Sep;50(3):399–410.
- Beumer J, Hamada MO, Lewis S. A prosthodontic overview. Int J Prosthodont. 1993 Mar-Apr;6(2):126–130.
- Garber DA, Belser UC. Restoration-driven implant placement with restoration-generated site development. Compend Contin Educ Dent. 1995 Aug;16(8):796,798–802.
- Hebel KS, Gajjar RC. Cement-retained versus screw-retained implant restorations: achieving optimal occlusion and esthetics in implant dentistry. J Prosthet Dent. 1997 Jan;77(1):28–35.
- Taylor TD, Agar JR. Twenty years of progress in implant prosthodontics. J Prosthet Dent. 2002 Jul;88(1):89–95.
- Mansour A, Ercoli C, Graser G, Tallents R, Moss M. Comparative evaluation of casting retention using the ITI solid abutment with six cements. Clin Oral Implants Res. 2002 Aug;13(4):343–348.
- Pauletto N, Lahiffe BJ, Walton JN. Complications associated with excess cement around crowns on osseointegrated implants: a clinical report. Int J Oral Maxillofac Implants. 1999 Nov-Dec;14(6):865–868.
- Gapski R, Neugeboren N, Pomeranz AZ, Reissner MW. Endosseous implant failure influenced by crown cementation: a clinical case report. Int J Oral Maxillofac Implants. 2008 Sep-Oct;23(5):943–946.
- Wilson TG Jr. The positive relationship between excess cement and peri-implant disease: a prospective clinical endoscopic study. J Periodontol. 2009 Sep;80(9):1388–1392.
- Wadhwani CP. Peri-implant disease and cemented implant restorations: a multifactorial etiology. Compend Contin Educ Dent. 2013 Oct;34 Spec No 7:32–37.
- Wadhwani C, Rapoport D, La Rosa S, Hess T, Kretschmar S. Radiographic detection and characteristic patterns of residual excess cement associated with cement-retained implant restorations: a clinical report. J Prosthet Dent. 2012 Mar;107(3):151–157.
- Ramer N, Wadhwani C, Kim A, Hershman D. Histologic findings within peri-implant soft tissue in failed implants secondary to excess cement: report of two cases and review of literature. NY State Dent J. 2014 Mar;80(2):43–46.
- Burbano M, Wilson TG Jr, Valderrama P, Blansett J, Wadhwani CP, Choudhary PK, Rodriguez LC, Rodrigues DC. Characterization of Cement Particles Found in Peri-implantitis-Affected Human Biopsy Specimens. Int J Oral Maxillofac Implants. 2015 Sep-Oct;30(5):1168–1173.
- Wadhwani C, Piñeyro A, Avots J. An esthetic solution to the screw-retained implant restoration: introduction to the implant crown adhesive plug: clinical report. J Esthet Restor Dent. 2011 Jun;23(3):138–143.
- Wadhwani CP, Schwedhelm ER. The role of cements in dental implant success, Part I. Dent Today. 2013 Apr;32(4):74–78;quiz78–79.
- Wadhwani CP, Piñeyro A, Akimoto K. An introduction to the implant crown with an esthetic adhesive margin (ICEAM). J Esthet Restor Dent. 2012 Aug;24(4):246–254.
- Linkevicius T, Vindasiute E, Puisys A, Linkeviciene L, Maslova N, Puriene A. The influence of the cementation margin position on the amount of undetected cement. A prospective clinical study. Clin Oral Implants Res. 2013 Jan;24(1):71–76.
- Wadhwani C. Ed. Cementation in Dental Implantology: An evidence based guide. Heidelberg. Springer and Medical and business media; p.139–145.
