

Principles of Interprofessional Collaboration
An increased emphasis on interdisciplinary cooperation between all members of the health care team can improve oral and systemic health outcomes.
An increased emphasis on interdisciplinary cooperation between all members of the health care team can improve oral and systemic health outcomes
This course was published in the April 2016 issue and expires 04/30/19. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Identify the components of interprofessional education and collaboration.
- Discuss the barriers to implementing interprofessional education.
- Identify the core competencies of interprofessional education.
- Provide examples of academic programs within the dental education system that are implementing interprofessional education.
Increased awareness among medical and dental providers regarding the connection between oral health, systemic disease, and overall health and wellness has given rise to an emphasis on interprofessional collaboration. Interprofessional teamwork, education and collaborative practice are becoming key elements of efforts to promote health and treat patients.1 Defined as cooperation, coordination and collaboration between health professions in delivering patient-centered care,2 its successful implementation requires health professionals from different backgrounds to provide comprehensive and coordinated services by working with patients, families, caregivers and communities to deliver whole-body care.2–5
Interprofessional education occurs when students or members of two or more health or social professions learn about, from, and with each other to enable effective collaboration and improve health outcomes.2–5 Evidence suggests that interprofessional education enables effective collaborative practice, which, in turn, optimizes health care services, strengthens medical systems and improves health outcomes.4 The interprofessional educational approach enables an interdisciplinary sharing of expertise, perspectives and resources.2,3,5
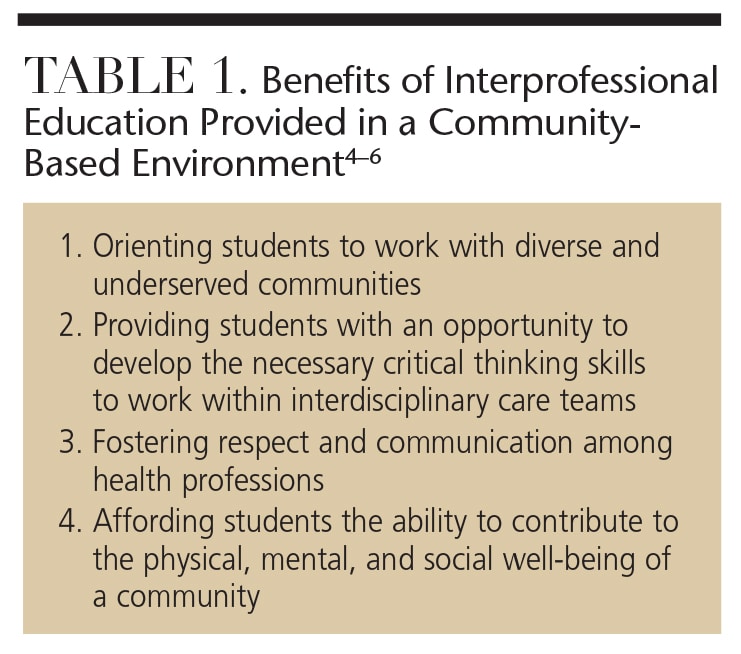
The seminal report, “Dental Education at the Crossroads,” released by the Institute of Medicine in 1995, identified the need for dental professionals to engage with other health professionals for the benefit of patients’ overall health.5 Interprofessional education provided in a community-based environment has many benefits (Table 1).4–6 Medical and dental academic program accreditation standards have further prompted the interprofessional movement, with the goal of graduating students who have an interdisciplinary approach to patient-centered care. The Commission on Dental Accreditation requires preparation of both dental and dental hygiene graduates for interprofessional collaboration.7
Federal health care legislation — including the Affordable Care Act (ACA) and Children’s Health Insurance Program Reauthorization Act — contains drivers for interprofessional collaboration. These seek more efficient health care models that will bridge the medical/dental divide, thus improving patients’ access to care and promoting optimal health outcomes.8 The ACA strives to advance public health and reduce the per capita cost of health care via a “triple aim” approach.9 The triple aim in dentistry focuses on reducing costs, evidence-based care (with an emphasis on risk assessment, management and reduction), and the preservation of hard and soft tissue. All three are facilitated by applying a medical care model to dentistry.10
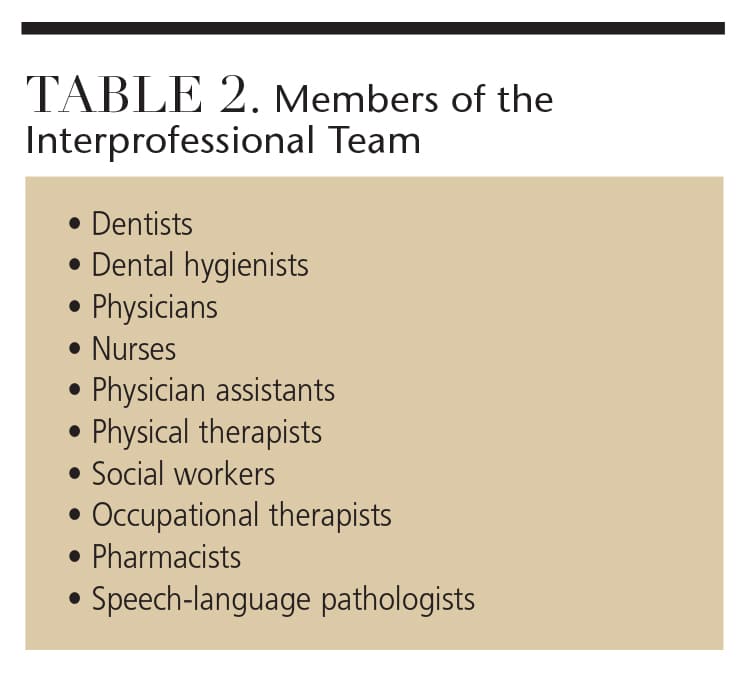
Today’s patients often have complex health care needs, and present with risk factors associated with other diseases that typically require an interdisciplinary approach.3,10 The collaboration of medical and dental teams may increase patient awareness about the connection between oral heath and overall wellness, possibly alleviating secondary medical problems associated with poor oral health. Table 2 lists the participants in interprofessional teams.
BARRIERS TO IMPLEMENTATION
There are many challenges to implementing interprofessional education and collaboration, including separate systems of dental and medical education, patient financing for dental care, crowded curricula, difficulty in training students and faculty, finding a location for training, scheduling conflicts, and lack of faculty development and administrative support.11–13 Because health profession education and training have traditionally been conducted through separate systems, physicians and other primary care practitioners are not trained to examine the oral cavity, screen for oral-systemic health issues, or provide preventive oral health education.11 Most traditional dental schools also do not prepare dental students to participate in the comprehensive health care of patients.11 This separation contributes to oral health inequities across populations. Many patients’ employers provide basic medical insurance, but not dental benefits. Older adults covered by Medicare and economically disadvantaged individuals covered by Medicaid do not receive dental benefits. Private dental insurance operates under a different model than medical health insurance.11
Integrating interprofessional education into existing programs poses logistical issues related to the timing of semesters, curricula and class scheduling.14 Many educational institutions house their medical and dental programs on different campuses.14 It may be taxing for educational institutions to find time for training and a location to house multiple disciplines. Although online training for students and faculty is one alternative, face-to-face training or “hands-on” learning is most valuable in preparing students to interact with other health care professionals.13 Faculty may also require training in interprofessional education if they have had little exposure to the concept. Many clinical sites where faculty members oversee training lack robust or explicit examples of interprofessional, team-based care.13 Faculty training should be experiential and facilitated through interprofessional initiatives that are competency driven and in alignment with student competencies.13 It is also important to ensure the deans and department heads of different disciplines are supportive of interprofessional education.13
CORE COMPETENCIES
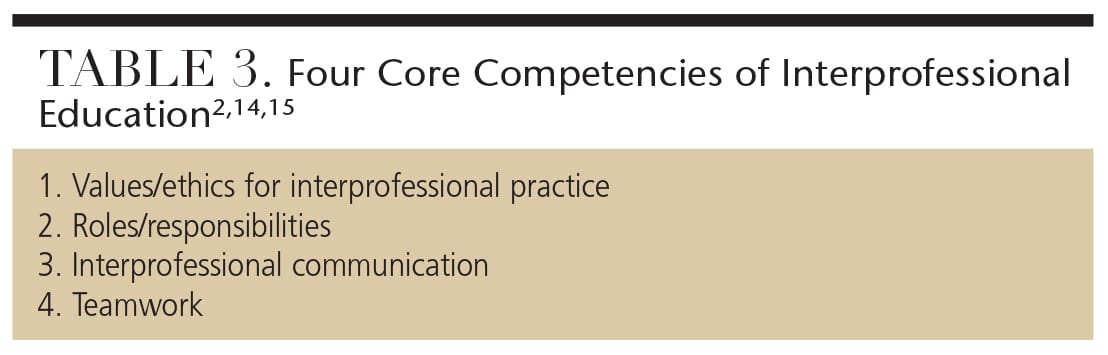
Table 3 lists the four core competencies of interprofessional education.2,14,15 Interprofessional values and ethics should be patient-centered with a community orientation and grounded in a sense of shared purpose to create safe and more effective systems of care. Students and faculty should work with individuals from other professions to maintain a climate of mutual respect and shared values.2,15 Learning interprofessional skills requires an understanding of how professional roles and responsibilities complement each other in patient-centered and community-oriented care. Students and faculty should use the knowledge of their roles and those of other professions to assess and address the health care needs of the patients and populations they serve.2,15 Communication competencies help students and faculty prepare for collaborative practice, and a readiness to work together facilitates effective interprofessional collaboration.2 Presenting information that team members, patients, families and communities can understand contributes to the overall wellness and the treatment of disease.2,15
Teamwork behaviors involve cooperating in patient-centered delivery of care, coordinating care with other health professionals so that gaps, redundancies and errors are avoided, and collaborating with others through shared problem solving and decision making.2 Working in teams involves sharing expertise and relinquishing some professional autonomy in order to work closely with others — including patients and communities — to achieve optimal outcomes.2 Shared accountability, problem solving, and decision making are characteristics of collaborative teamwork. Team members establish a common goal, synthesize their observations and profession-specific expertise, and collaborate and communicate as a team. Joint decision making is valued, and each team member is empowered to assume leadership on patient-care issues appropriate to his or her expertise.2,15,16
APPLICATION IN DENTAL PRACTICE
Health center schools, as well as other health profession programs, are being encouraged to introduce joint learning experiences into their educational programs so that students will graduate with an understanding of the roles and responsibilities of related health professions, and how collaboration can contribute to improved care.15 As learning shifts from the classroom to clinical practice, interprofessional work takes on a greater significance. Learning becomes more relationship-based and involves increasingly more complex interactions with others, including patients, families and communities.1 Interprofessional education may be formal or informal at any point across the education-to-clinical-practice continuum. Organized, formal interprofessional education activities provide the basic foundation of collaborative competence. They generally are didactic or simulated and occur in highly supervised clinical environments.1
The current interprofessional education literature is predominantly centered on dental, nursing, physician assistant and podiatry students. In 2004, Rosalind Franklin University of Medicine and Science in Chicago designed a one-credit, pass/fail course with three components, didactic, service learning and clinical, to facilitate interprofessional education.3 The interdisciplinary family health course at the University of Florida in Gainesville has been providing interprofessional community-based learning experiences for more than 10 years.3 This course is required for all first-year students in the medical, dental, pharmacy, nursing, physical therapy, psychology and nutrition programs. The course is two semesters and is based on four home visits with volunteer families by an interprofessional team of three students.3
In 1997, the University of Washington in Seattle established the Center for Health Sciences Interprofessional Education in an effort to integrate teaching, research and professional activities of the schools of medicine, pharmacy, nursing, social work, public health and dentistry. More than 50 collaborative interprofessional offerings are available.
In 2005, the New York University (NYU) College of Nursing moved into the NYU College of Dentistry. Since then, the College of Nursing has established a nurse faculty practice in the dental school, in which nurse practitioners are available for consultation on the dental clinic floor.17 Twice weekly, nursing faculty work with dental students as they chart medical histories, educating them about conditions that might impact dental treatment.17 Since 2009, students in dentistry, osteopathic medicine, graduate nursing, physical therapy and pharmacy at Western University in Pomona, California, have participated in the university’s interprofessional education curriculum, which is designed to progressively advance knowledge and skills through didactic instruction, simulation and clinical care.16 Students are trained to provide outreach, triage, and patient care to at-risk populations.
A partnership between the University of the Pacific Arthur A. Dugoni School of Dentistry and the University of California, San Francisco (UCSF) School of Medicine was established in 2014.18 The two schools have signed a memorandum of understanding for an interprofessional education program that will provide collaborative learning opportunities between fourth-year UCSF medical students and third-year dental students from the University of the Pacific. The medical students observe oral health care delivery for patients who have moderate to severe medical, developmental and psychosocial conditions.18
The interprofessional education model at the Louisiana State University (LSU) Health Sciences Center School of Dentistry in New Orleans was developed in 2005. Dental hygiene students work with elementary school nurses in a school-based environment and perform noninvasive oral health screenings for children. Based on collaboration between LSU nursing students and dental hygiene students, the School of Dentistry curriculum now requires residents in advanced dentistry and dental hygiene students to work together as teams. These teams coordinate treatment with the directors of nursing in state developmental centers for individuals with neurodevelopmental/intellectual disabilities to increase these clinicians’ competency and experience.19
The oral-systemic connection and interprofessional collaboration are among some of dental education’s key focus areas in the Mesa Community College (MCC) dental hygiene program in Arizona. In 2015, Prendergast et al20 developed the Bedside Oral Exam (BOE) to determine the oral health risks of patients in hospital settings.20 Working in pairs, MCC dental hygiene students perform BOEs under the supervision of hospital staff and faculty. Future plans for this collaboration include dental hygiene students educating other health professionals about the effects of pathogenic oral bacteria on systemic health and the benefits of preventive oral care.20
Northern Arizona University in Flagstaff instituted a family health day in 2015 in which the families of students and faculty were invited to participate in hearing tests, blood pressure screenings, nutritional education, glucose screening and dental hygiene services. Students from different disciplines worked together at the various stations. Students from all disciplines completed a three-question survey after the health fair ended. Most students commented they learned something new from a different discipline, such as how to communicate with students in other programs of study, how to educate families about the importance of health and dental screenings, and how to work in teams.
CONCLUSION
Oral health professionals can play a major role in medical screening and monitoring of chronic diseases, such as diabetes and hypertension. Research has demonstrated that the status of patients’ diabetes and hypertension can affect both their oral and overall health.15,21 The interprofessional education/collaboration model expands the dental professional’s scope of practice to include disease assessment and prevention, chronic disease screening, disease management within an integrated health care system, and managing, communicating and collaborating with other health professionals.21,22
Administrative leadership, funding and support from within the academic setting are critical in order to engage all disciplines. Faculty need to be adequately trained in order to teach students how to ensure high-quality outcomes utilizing an interdisciplinary approach. Tomorrow’s dental clinicians will need to be adequately trained in interprofessional collaboration in order to meet the growing demands of a diverse population and provide cost-effective, high-quality oral health care in a team-based atmosphere.
References
- National Academy of Sciences. Measuring the Impact of Interprofessional Education on Collaborative Practice and Patient Outcomes, 2015. Available at: nap.edu/catalog.php?record_id=21726. Accessed March 1, 2016.
- Interprofessional Collaborative Practice. Core Competencies for Interprofessional Collaborative Practice: Report of an Expert Panel. Available at: http://www.aacn.nche.edu/education-resources/ipecreport.pdf. Accessed March 1, 2016.
- Bridges DR, Davidson RA, Odegard PS, Maki IV, Tomkowiak J. Interprofessional collaboration: three best practice models of interprofessional education. Med Educ Online. 2011;8:16.
- World Health Organization, Department of Human Resources for Health. Framework for Action on Interprofessional Education & Collaborative Practice. Available at: http://apps.who.int/iris/bitstream/10665/70185/1/WHO_HRH_HPN_10.3_eng.pdf. Accessed March 1, 2016.
- Hettinger L, Gwozdek A. Utilizing community-based education as a springboard for interprofessional collaboration. Access. 2015;29(3):11–13.
- Price SS, Funk AD, Shockey AK, et al. Promoting oral health as part of an interprofessional community-based women’s health event. J Dent Ed. 2014;78:1294–1300.
- Commission on Dental Accreditation. Accreditation Standards for Dental Hygiene Programs. Available at: ada.org/~/media/ coda/files/dh.ashx. Accessed March 1, 2016.
- Edelstein BL. The roles of federal legislation and evolving health care systems in promoting medical-dental collaboration. Calif Dent Assoc J. 2014;42(1):19–23.
- Robinson LA, Krol DM. Interprofessional education and practice…moving toward collaborative, patient-centered care: part two. Calif Dent Assoc J. 2014;42(9):616–618.
- Krol DM, Gesko D, Hilton I, Garlan T, McCauley L. Panel proceedings; conference on interprofessional education and practice. California Dental Association and American Dental Education Association. February 2014. Calif Dent Assoc J. 2014;42(9):622–623.
- Mouradian WE, Lewis CW, Berg JH. Integration of dentistry and medicine and the dentist of the future: the need for the health care team. Calif Dent Assoc J. 2014;42(10):687–696.
- Conway SE, Smith WJ, Truong TH, Shadid J. Interprofessional pharmacy observation activity for third-year dental students. J Dent Ed. 2014;78:1313–1318.
- Hall LW, Zierler BK. Interprofessional Education and Practice Guide No. 1: developing faculty to effectively facilitate interprofessional education. J Interprof Care. 2015:29:3–7.
- Valachovic RW. Integrating oral and overall health care — on the road to interprofessional practice: building a foundation for interprofessional education and practice. Calif Dent Assoc J. 2014;42(1):25–27.
- Formicola AJ, Andrieu SC, Buchananan JA, et al. Interprofessional education in U.S. and Canadian dental schools: an ADEA team study group report. J Dent Ed. 2012;76:1250–1268.
- Friedrichsen S, Martinez TS, Hostetler J, Tang JMW. Innovations in interprofessional education: building collaborative practice skills. Calif Dent Assoc J. 2014;42(9):627–635.
- Wilder RS. Dental hygienists and interprofessional collaboration: thoughts from 1927. J Den Hyg. 2013;87:108–109.
- University of Pacific Arthur A. Dugoni School of Dentistry. Pacific Dugoni Partners with UCSF School of Medicine on Interprofessional Education Opportunities. Available at: http://dental.pacific.edu/News_and_Events/News_Archive/Pacific_Dugoni_Partners_with_UCSF_School_of_Medicine_on_Interprofessional_Education_Opportunities.html. Accessed March 1, 2016.
- Mabry CC, Mosca NG. Interprofessional educational partnerships in school health for children with special oral health needs. J Den Ed. 2006;70:844–850.
- Prendergast V, Kleiman C, King M. The Bedside Oral Exam and the Barrow Oral Care Protocol: translating evidence-based oral care into practice. Intensive Crit Care Nurs. 2013;29:282–290.
- Robinson L. Interprofessional education and practice….the dentist of the future: part three. Calif Dent Assoc J. 2014;42(10):685–686.
- Berg JH, Mouradian WE. Integration of dentistry and medicine and the dentist of the future: changes in dental education. Calif Dent Assoc J. 2014;42(10):697–700.

