

Primary Prevention for Pediatric Patients
Establishing good oral health in this population requires the use of evidence-based guidelines for caries risk assessment and management.
Establishing good oral health in this population requires the use of evidence-based guidelines for caries risk assessment and management.
PURCHASE COURSE
This course was published in the October 2017 issue and expires October 2020. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the October 2017 issue and expires October 2020. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
- Explain the concept of the age 1 dental visit and establishing a dental home, as well as key components of the pediatric visit.
- Describe methods to engage patients and parent/caregivers to establish oral health goals.
- List preventive and caries management approaches that are appropriate to this patient population.
The American Academy of Pediatric Dentistry (AAPD) recommends that children establish a dental home by age 1 or within six months of their first tooth erupting.1 A dental home is the ongoing relationship between the dentist and patient, inclusive of all aspects of oral health care.2 Parents and caregivers may be unaware of this recommendation or feel that a dental visit in the first year of life is “too early,” despite numerous studies that show early and regular visits are cost-effective.3 The purpose of the age 1 dental visit is to perform a comprehensive examination and caries risk assessment, identify early signs of pathology (including caries), apply fluoride, and educate parents/caregivers.
Given their frequent interaction with infants and young children, pediatricians and other health professionals also play an important role in promoting oral health; as such, oral health screenings, fluoride application and caries risk assessment are standard protocol in well-child visits.4 Because caries and early loss of primary teeth can affect learning, communication, nutrition, overall well-being, and other activities necessary for growth and development, every health professional should be prepared to answer questions about why it is important to invest time, energy and resources into “baby teeth.”
In light of the expansion of pediatric dental coverage under the Affordable Care Act (ACA), it was anticipated that the number of pediatric patients seeking dental care would increase. However, there is limited and mixed data about whether the ACA has improved access to care for pediatric patients.5 Nevertheless, dentists and auxiliary staff should be prepared to provide age-specific oral health care instructions and preventive education for children from infancy through adolescence.
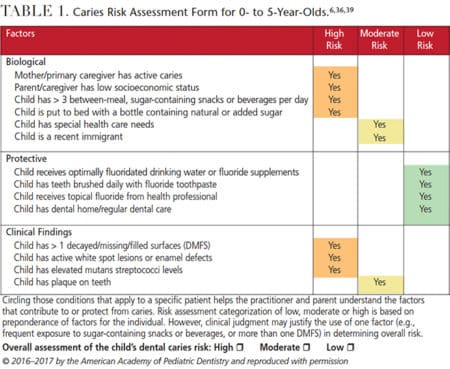
Pediatric dental visits should include a thorough parent/caregiver interview, followed by a caries risk assessment, prophylaxis, examination, fluoride application, and age-appropriate anticipatory guidance. (Examples of pediatric-appropriate caries risk assessment forms can be found in Table 1 and Table 2.) Additional procedures, such as radiographs, are completed when deemed appropriate, but must be used with caution, as recommended by the Image Gently (ImageGently.org) and Image Wisely (ImageWisely.org) campaigns.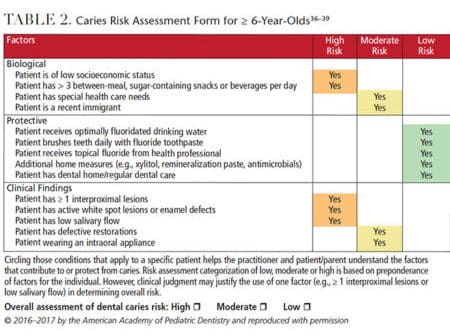
The parent/caregiver interview should address the following items:6
- Medical and dental histories
- Diet intake patterns and frequency
- Oral hygiene practices
- Fluoride use
- Nutritive and nonnutritive habits
- Previous trauma
- Other elements in the caries risk assessment protocol (see Table 3 for a list of caries risk assessment resources)
Information from the interview is used in conjunction with clinical findings to determine a child’s caries risk. The caries risk assessment and caries assessment tools (CAT) are used to determine the likelihood of a child developing future caries by evaluating the balance — or imbalance — between risk factors and protective factors.6,7 Although the positive predictive value of the CAT is low, it allows dentists to create a patient-tailored approach to caries prevention.6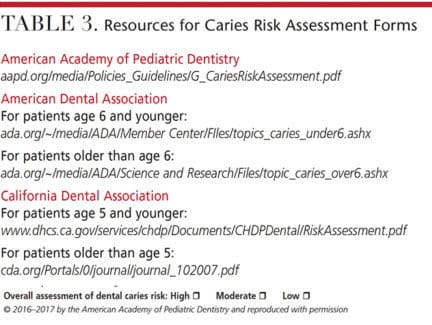
The infant exam is typically performed in the knee-to-knee position, and a toothbrush is often used to perform the prophylaxis.6 Some parents/caregivers may not perceive the value of a toothbrush prophylaxis, so it is important that they understand that teeth must be clean so that they can be examined thoroughly, a toothbrush prophylaxis helps demonstrate appropriate brushing technique, and that use of a rubber cup or scaling is generally unnecessary in young children since most do not have calculus or extrinsic stains.8 Once the child’s level of cooperation permits, he or she can be seen in the dental chair, and a rubber cup can be introduced.
ORAL HEALTH EDUCATION
For young children, the parents/caregivers are primarily responsible for influencing diet and hygiene practices, and should consequently be the focus of oral health education. Dentists and auxiliaries should engage and allow parents/caregivers to observe proper hygiene techniques, identify teeth with significant plaque accumulation, pinpoint teeth with early or advanced caries, and discuss other conditions of concern during the prophylaxis and exam. Plaque disclosing solutions and hand mirrors can play an important role in the education process. Based on evaluation of oral hygiene and caries risk assessment, as well as the overall diagnosis, the dental team will summarize the findings, develop a preventive/treatment plan, and determine which recommendations to suggest.
The dentist and auxiliaries can use motivational interviewing and self-management goals to elicit behavior change and increase compliance with recommendations.9,10 This approach engages the parent/caregiver to connect with self-identified goals to strengthen the intrinsic motivation for positive and realistic changes.11 Providing an extensive list of recommendations can be overwhelming for first-time parents or children having their first dental exam. Studies indicate that oral health instructions should identify one or two key goals through the motivational interviewing process described above.6 At subsequent appointments, progress toward meetings these goals can be revisited. When they are achieved, new goals can be established.
Examples of common goals that the dentist and parent/caregiver can mutually agree upon include:
- Keeping regular dental visits for the child
- Providing healthy snacks
- Brushing with fluoride toothpaste at least twice daily
- Consuming less or no soda and juice
- Weaning from a bottle
- Only drinking water in a sippy cup
- Drinking (fluoridated) tap water
- Consuming less or no junk food and candy
CARIES MANAGEMENT STRATEGIES
Just as the clinical presentation of caries varies widely, so do approaches to treatment. Many factors influence the timing and type of treatment, such as the rate and extent of decay, as well as the child’s psychosocial development.
One important reason for early and regular dental visits is to identify incipient lesions so clinicians can attempt to arrest or recalcify them with fluoride varnish and favorable home care.12 Adjuncts to fluoride therapy include the use of chlorhexidine gluconate and povidone iodine.13 While these are effective for reducing the bacterial load, there is mixed evidence supporting their use as anticaries strategies.14–17 A child with an active caries process is considered high risk and should be seen on a three- to six-month schedule.6 Children who are low risk require less frequent recall appointments.
When a lesion has become cavitated, clinicians must decide whether treatment is necessary or if restorative therapy can be delayed. This decision is based on the rate and extent of decay, and the likelihood the child will cooperate during treatment18 (particularly in the case of very young children who may not predictably cooperate for restorative care). Such patients may require interim restorations with the use of a spoon or slow speed handpiece for caries excavation, followed by placement of a restorative material, such as glass ionomer.19 The goal is to remove the most active part of the lesion,20 avoid the use of anesthetic agents, and buy time for the patient to reach an age where he or she can cooperate for a definitive restoration. If a child has advanced treatment needs and/or does not have the means to cooperate for restorative care, advanced behavior guidance — such as protective stabilization, moderate sedation or general anesthesia — may be necessary.21 Due to recent media attention and studies of safety concerns with moderate sedation and general anesthesia in children — particularly repeat exposures and exposure early in life — dentists must exercise extreme caution and be aware of public perceptions about these approaches.22
The U.S. Food and Drug Administration (FDA) has granted a “breakthrough therapy” designation to silver diamine fluoride (SDF) 38% for use in arresting caries in children and adults. This agent was previously cleared by the FDA for treating dentinal hypersensitivity. Although silver-based products have a long history of use in medicine and dentistry, SDF was not given FDA clearance for dental use in the United States until 2014. Initial research into its capacity to inhibit caries progression is promising. It can be used by dental and nondental providers in the secondary and tertiary treatment of caries. Most protocols for SDF use are empirical in nature,23 and evidence-based guidelines will be developed from the results of trials that are currently under way. At this time, SDF appears to be a cost-effective and easy-to-use option for caries management.24
Again, the purpose of early dental care is to prevent the onset of disease. If primary prevention is not successful, the hope is that early and regular dental visits will slow caries progression and allow for early detection.12
Up to 90% of caries in school-aged children occurs in pits and fissures. In 2016, the American Dental Association and AAPD concluded that: (1) sealants are effective in preventing and arresting pit-and-fissure lesions of primary and permanent molars in children and adolescents; (2) they can minimize the progression of noncavitated occlusal caries lesions; and (3) there is insufficient evidence to support one type of sealant material over others.25 Sealants on at-risk molars provide a cost-effective way to reduce the risk of caries in these teeth. Subsequent recalls should include verifying the sealant is still present and replacing or repairing sealants when appropriate. Though sealants provide a means of reducing caries in pits and fissures, it is important to remind parents/caregivers that sealants do not prevent gingival disease or reduce the risk of caries to smooth surfaces.
This discussion reflects the spectrum of caries management, with the least invasive approach being watchful observation of early lesions, along with the application of fluoride (or other medicaments, such as SDF), and the most invasive being treatment under moderate sedation or general anesthesia.18,19 Sealants may be a means of primary and secondary prevention in at-risk pits and fissures.
DEVELOP A PREVENTIVE PLAN
Focus on Toothbrushing: Many patients know that brushing with fluoridated toothpaste should occur twice daily and flossing should occur daily, yet, based on limited data, compliance is low.26 Parents/caregivers may offer many reasons for nonadherence,27 such as uncooperative children, busy schedules, the belief that caries are inevitable, and lack of oral health knowledge, among others.28 The AAPD recommends the use of fluoride-containing toothpaste for dentate children of any age.29 Recent changes in the recommendation stating that fluoride toothpaste is universally indicated for all children, regardless of caries risk, is a common point of confusion for parents/caregivers, medical professionals and even some dental providers. This is particularly important as fewer people drink municipally available, optimally fluoridated water due to concerns about water safety.
A simple means of monitoring the amount of fluoride that a child may potentially ingest is by controlling the amount of toothpaste placed on a toothbrush. Children younger than age 2 should have only a smear of toothpaste (0.125 gram), while children ages 2 to 5 should receive a pea-sized amount (0.25 gram).27 Dental professionals should demonstrate appropriate, age-specific quantities because parents/caregivers may have difficulty applying the correct amount.30 The fluoride content in most nonprescription pediatric and adult toothpaste is the same; the only difference is flavoring that may be more palatable to children. While fluoride-free “training toothpastes” are available, they are of little benefit and send the message that fluoridated toothpastes are not safe for young children.29
Communication Principles: Although dental terminology and an understanding of caries and periodontal disease are fundamental to oral health care providers, parents/caregivers and pediatric patients are not likely to have a full understanding of the mechanisms by which individuals develop caries and periodontal disease. Oral health literacy is a key factor; this is the degree to which individuals have the capacity to obtain, process and understand basic health information and services needed to make appropriate oral health decisions.31 Compared to those with higher health literacy, individuals with low oral health literacy are less likely to utilize preventive services and maintain a regular recall schedule. In addition, they are more likely to utilize emergency services for dental care, and may be at higher risk of developing caries.32 Consequently, dental teams must assess parents’/caregivers’ and pediatric patients’ oral health literacy, provide simple, direct messages (avoiding dental jargon) and seek feedback using open-ended questions.
When communicating oral health information, it is important to offer parents/caregivers visual aids; this can be done using dental models, graphics and images. When possible, parents/caregivers should engage in “teach back,” in which they demonstrate their ability to perform a task — such as their ability to floss a model or brush their child’s teeth using proper technique. The process of explaining, demonstrating and engaging parents/caregivers in hands-on participation should achieve the most favorable outcome for all learning styles.
Kid-Friendly Dental Products: The tendency for many dental teams is to hand a patient or parent/caregiver a goodie bag containing a toothbrush, toothpaste, floss, mouthrinse and other kid-friendly products. This can be overwhelming and send mixed messages. While mouthrinses and novelty products might be fun to use, brushing with the proper frequency, duration and technique — and using fluoridated toothpaste — is the best preventive measure.
Parents/caregivers may have mixed understanding about whether dental floss should be used in children. The AAPD recommends flossing once the interproximal spaces between primary teeth are closed because they are no longer cleansable with a toothbrush.33 A barrier to compliance with this recommendation may be lack of knowledge and reported difficulty flossing a child’s teeth. Many manufacturers produce flossing aids, which may be easier for children or parents/caregivers to use.
Mouthrinse or fluoride rinse should never be a substitute for proper brushing and flossing; rather, they should only be used as adjuncts to an appropriate home-care regimen. Manual and electric toothbrushes can both be effective in plaque removal when used with the proper technique, duration and frequency.34 For this reason, one of the best giveaways in a goodie bag is a 2-minute timer. A caveat is that some parents/caregivers report their children enjoy using electric toothbrushes more than manual toothbrushes. If electric toothbrushes bear a certain level of novelty, have built-in timers, and make the process fun for the children — thereby increasing compliance — clinicians may wish to recommend these products.
Toothbrushing with a soft-bristled, appropriately sized toothbrush should begin when the first teeth begin to erupt.34 A wet cloth can be used as needed to clean infants’ teeth, such as between breastfeeding. Initially, toothbrushing is performed solely by the parent/caregiver. Toddlers may enjoy chewing on toothbrushes, but it is important for parents/caregivers to continue to brush for the child, playing an active role until the child has developed sufficient manual dexterity. This normally occurs around age 8, but, even at this age, parents/caregivers need to reinforce brushing frequency and technique. One strategy that is mutually beneficial for children and parents/caregivers is to encourage brushing together. This not only reinforces brushing habits, it allows for direct supervision and for the adult to model appropriate technique.
Although infant products with rubber bristles may serve as gum stimulators and teething toys, they are not particularly effective for plaque removal, consequently, they should not be used as substitutes for toothbrushes. Cold teething rings and other soft teething products stimulate the gums and may alleviate discomfort when primary teeth are erupting.35 Topical benzocaine products should not be used in children younger than 2 years of age, however, due to risk of methemoglobinemia.35
CONCLUSION
Dentists and auxiliaries must be familiar with the steps necessary to provide effective dental care to children from infancy through adolescence. To decrease the burden of disease, the emphasis should be on primary prevention. When needed, treatment modalities and caries control measures will vary, depending on the rate and extent of decay, as well as the child’s behavior. Awareness of oral health literacy and parent/caregiver engagement through motivational interviewing are essential to elicit behavior change. To increase the likelihood of compliance, the dental team can recommend various kid-friendly products, but emphasize that brushing with fluoridated toothpaste and using floss regularly are the most effective anticaries hygiene practices.
REFERENCES
- American Academy of Pediatric Dentistry. Policy on the dental home. Pediatr Dent. 2016;38:12.
- Nowak AJ, Casamassimo PS. The dental home: a primary care oral health concept. J Am Dent Assoc. 2002;133:93–98.
- Lee JY, Bouwens TJ, Savage MF, Vann WF Jr. Examining the cost-effectiveness of early dental visits. Pediatr Dent. 2006;28:102–105.
- Segura A, Boulter S, Clark M, et al. Maintaining and improving the oral health of young children. Pediatrics. 2014;134:1224–1229.
- Nasseh K, Vujicic M, O’Dell A. Affordable Care Act expands dental benefits for children but does not address critical access to dental care issues. Available at: ada.org/~/media/ADA/Science%20and%20Research/HPI/Files/HPIBrief_0413_3.pdf. Accessed September 11, 2017.
- Ramos-Gomez FJ, Crall J, Gansky SA, Slayton RL, Featherstone JD. Caries risk assessment appropriate for age 1 dental visit (infants and toddlers). J Calif Dent Assoc. 2007;35:687–702.
- Featherstone JD. The caries balance: the basis for caries management by risk assessment. Oral Health Prev Dent. 2004;2 (Suppl 1):259–264.
- American Academy of Pediatric Dentistry. Policy on the role of dental prophylaxis in pediatric dentistry. Pediatr Dent. 2016;38:43–44.
- Weinstein P, Harrison R, Benton T. Motivating parents to prevent caries in their young children: one-year findings. J Am Dent Assoc. 2004;135:731–738.
- Kay EJ, Logam HL, Jakobsen J. Is dental health education effective? Systematic review of current evidence. Community Dent Oral Epidemiol. 1996;24:231–235.
- Rollnick S, Miller WR. What is motivational interviewing? Behav Cogn Psychother. 1995;23:325–334.
- Featherstone JD. Caries prevention and reversal based on the caries balance. Pediatr Dent. 2006;26:128–132.
- Milgrom P, Chi DL. Prevention-centered caries management strategies during critical periods in early childhood. J Calif Dent Assoc. 2011;39:735–741.
- Autio-Gold J. The role of chlorhexidine in caries prevention. Oper Dent. 2008;33:710–716.
- van Rijkom HM, Truin GJ, van’t Hof MA. A meta-analysis of clinical studies on the caries-inhibiting effect of chlorhexidine treatment. J Dent Res. 1996;75:79–795.
- Nowak A, Casamassimo PS. Using anticipatory guidance to provide early dental intervention. J Am Dent Assoc. 1995;126:1156–1163.
- Lopez L, Berkowitz R, Spiekerman C, Weinstein P. Topical antimicrobial therapy in the prevention of early childhood caries: a follow-up report. Pediatr Dent. 2002;24:204–206.
- Nelson T. The continuum of behavior guidance. Dent Clin North Am. 2013;57:129–143.
- American Academy of Pediatric Dentistry. Policy on early childhood caries: unique challenges and treatment options. Pediatr Dent. 2016;38:55–56.
- American Academy of Pediatric Dentistry . Policy on interim therapeutic restorations (ITR). Pediatr Dent. 2016;38:50–51.
- American Academy of Pediatric Dentistry. Guideline on behavior guidance for the pediatric dental patient. Pediatr Dent. 2011;33:161–173.
- Sun LS, Li G, Miller TL, et al. Association between a single general anesthesia exposure before age 36 months and neurocognitive outcomes in later childhood. J Am Dent Assoc. 2016;315:2312–2320.
- Horst JA, Ellenikiotis H, UCSF Silver Caries Arrest Committee, Milgrom PM. UCSF protocol for caries arrest using silver diamine fluoride: rationale, indications, and consent. J Calif Dent Assoc. 2016;44:16–28.
- Cheng LL. Limited evidence suggesting silver diamine fluoride may arrest dental caries in children. J Am Dent Assoc. 2017;148:120–122.
- Wright JT, James JC, Fontana M, et al. Evidence-based clinical practice guideline for the use of pit-and-fissure sealants: a report of the American Dental Association and the American Academy of Pediatric Dentistry. J Am Dent Assoc. 2016;147:672–682.
- Inglehart M, Tedesco LA. Behavioral research related to oral hygiene practices: a new century model of oral health promotion. Periodontol 2000. 1995;8:15–23.
- Collett BR, Huebner CE, Seminario AL, Wallace, E, Gray KE, Speltz ML. Observed child and parent toothbrushing behaviors and child oral health. Int J Paediatr Dent. 2016;26:184–192.
- Bakdash B. Current patterns of oral hygiene product use and practices. Periodontol 2000. 1995;8:11–14.
- American Academy of Pediatric Dentistry. Guideline on fluoride therapy. Pediatr Dent. 2016;38:181–184.
- Thomas AS. Graduate thesis: Parents’ interpretation of instructions to control fluoride toothpaste application. Available at: depts.washington.edu/mchprog/docs/abstracts/2011/ThomasAbstract.pdf. Accessed September 11, 2017.
- American Dental Association. Oral Health Literacy in Dentistry. Available at: ada.org/en/public-programs/health-literacy-in-dentistry. Accessed September 11, 2017.
- Horowitz AM, Kleinman DV. Oral health literacy: the new imperative to better oral health. Dent Clin North Am. 2008;52:333–344.
- American Academy of Pediatric Dentistry. Guideline on periodicity of examination, preventive dental services, anticipatory guidance/counseling, and oral treatment for infants, children, and adolescents. Pediatr Dent. 2016;38:133–141.
- Robinson PG, Deacon SA, Deery C, et al. Manual versus powered toothbrushing for oral health. Cochrane Database Syst Rev. 2005;18:CD002281.
- U.S. Food and Drug Administration. Benzocaine Topical Products: Sprays, Gels and Liquids — Risk of methemoglobinemia. 2011. Available at: nwcemss.org/assets/1/clinical_practice_alerts/Benzocaine_Topical_Products_4-11.pdf. Accessed September 11, 2017.
- American Dental Association Councils on Scientific Affairs and Dental Practice. Caries Risk Assessment Form (Ages 0–6). Available at: ada.org/~/media/ADA/Member Center/FIles/topics_caries_under6.ashx. Accessed September 11, 2017.
- American Dental Association Councils on Scientific Affairs and Dental Practice. Caries Risk Assessment Form (Age >6). Available at: ada.org/~/media/ADA/Science and Research/Files/topic_caries_over6.ashx. Accessed September 11, 2017.
- Featherstone JD, Domejean-Orliaguet S, Jenson L, Wolff M, Young DA. Caries risk assessement in practice for age 6 through adult. J Calif Dent Assoc. 2007;35:703–713.
- American Academy of Pediatric Dentistry. Guideline on Caries Risk Assessment and Management for Infants, Children, and Adolescents. Available at: aapd.org/media/policies_guidelines/g_cariesriskassessment.pdf. Accessed September 11, 2017.
Featured image by SPYDERSKIDOO/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. October 2017;3(10):32–36.

