

Pathways for the Management of Early Childhood Caries
By understanding the risk factors, oral health professionals can prescribe appropriate preventive strategies for managing early childhood caries.
By understanding the risk factors, oral health professionals can prescribe appropriate preventive strategies for managing early childhood caries
PURCHASE COURSE
This course was published in the October 2018 issue and expires October 2021. Marion C. Manski, RDH, MS, has no commercial conflicts of interest to disclose. Norman Tinanoff, DDS, MS, is a consultant for the American Dental Association and the American Academy of Pediatric Dentistry. This 2 credit hour self-study activity is electronically mediated.
Early childhood caries is highly prevalent and increasing in poor and near-poor preschool children in the United States.2 In developing countries, the rate of early childhood caries can be as high as 86%.3 Surveys clearly indicate that besides early childhood caries being highly prevalent, it is largely untreated in children younger than 3.4
This course was published in the October 2018 issue and expires October 2021. Marion C. Manski, RDH, MS, has no commercial conflicts of interest to disclose. Norman Tinanoff, DDS, MS, is a consultant for the American Dental Association and the American Academy of Pediatric Dentistry. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Define early childhood caries and risk factors for lesion development in young pediatric patients.
- Describe signs of dental caries in this patient population.
- Explain clinical management strategies for caries prevention.
Consequences of early childhood caries include increased risk of new caries lesions, hospitalizations and emergency department visits, high treatment costs, reports of delays in growth and development, and diminished quality of life.1 Risk factors, such as previous caries, cariogenic bacteria, visible plaque, diet, enamel defects, socioeconomic status and suboptimal dosing of fluoride, are associated with the prevalence of early childhood caries. The purpose of this article is to discuss evidence-based care pathways for oral health professionals to manage this highly prevalent disease.
Early childhood caries was first described in 1962 by Fass,5 who referred to the condition as “milk bottle mouth” because he believed the cause was putting a child to bed with a baby bottle of milk. Prior to a 1998 National Institutes of Health-sponsored Early Childhood Caries Conference, dental caries in preschool children was referred to as “baby bottle syndrome,” “nursing bottle caries,” or “baby bottle tooth decay.”6 Each of these names was associated with rampant caries presumed to be caused by inappropriate use of a baby bottle. A better understanding of early childhood caries emerged during the conference, as well as awareness that early childhood caries was multifactorial, related to frequent sugar consumption in an environment of enamel adherent, acid-producing bacteria, and, in some cases, enamel hypoplasia.6
PREVALENCE AND ETIOLOGY
As noted, early childhood caries has been defined since 1999 as the presence of one or more decayed, missing (due to caries), or filled surfaces in any primary tooth of a child up to age 6.1 Severe early childhood caries (S-ECC) is defined as any sign of smooth-surface caries in children younger than 3. In children ages 3 to 5, one or more decayed, missing, filled (dmf) smooth surfaces in primary maxillary anterior teeth, or a dmf score of ≥ 4 (age 3), ≥ 5 (age 4), or ≥ 6 (age 5) surfaces also constitutes S-ECC.1 Typical early signs of early childhood caries include crescent-shaped white spot lesions or cavities at the gingival margin (Figure 1).

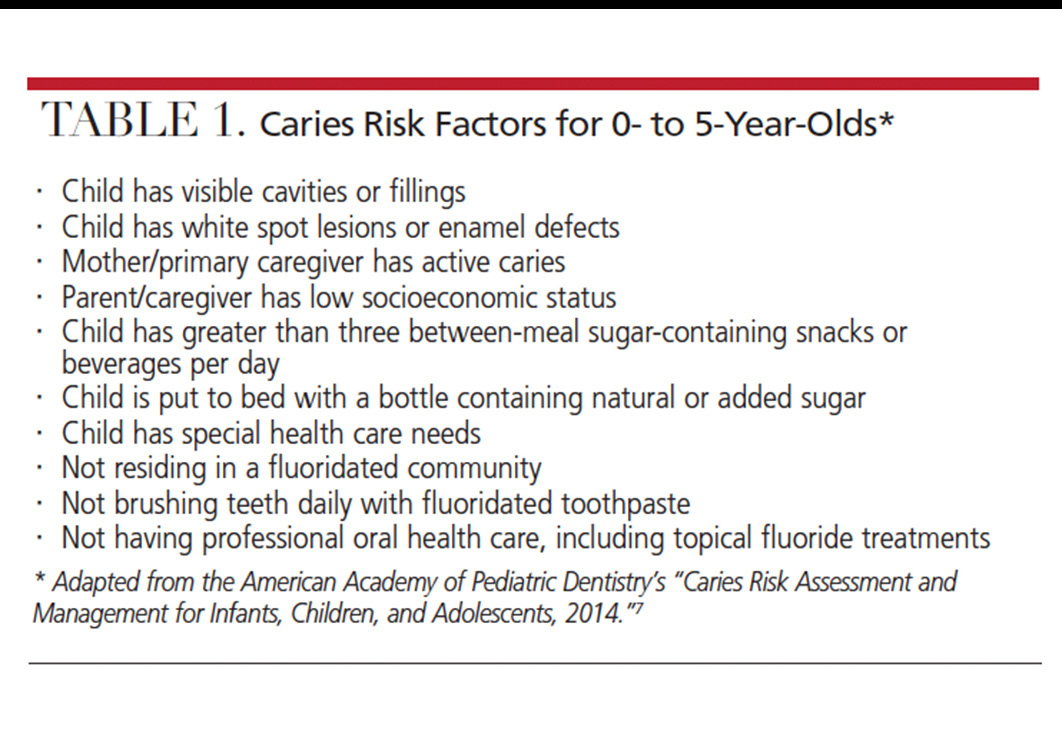
Risk factors for early childhood caries include the presence of white spot lesions or caries at initial examination, the mother/primary caregiver having active caries, a child having more than three between-meal sugar-containing snacks or beverages per day, and a child being put to bed with a bottle containing a liquid with natural or added sugar. The most significant risk factor, however, is a parent/caregiver having low socioeconomic status — that is, lifetime poverty, lack of oral health knowledge, living in food deserts, and deficient preventive behaviors in the community (Table 1).7
The bacteria most often associated with early childhood caries are mutans streptococci, which metabolize sugars to produce acid that lowers the pH of oral plaque. Low pH for an extended period results in a higher rate of enamel demineralization, thus contributing to caries. An early colonization of mutans streptococci is associated with the likelihood of caries formation. Colonization often begins with a vertical transmission to a child from a primary caregiver, usually the mother.8 High levels of mutans streptococci in a caregiver and frequent snacking by the child increases the chance of mutans streptococci colonization and proliferation in children. Horizontal transmission also may occur during encounters with other family members or children in daycare centers or school.
Due to early colonization of mutans streptococci, it is imperative that establishment of a dental home begin no later than 12 months of age. This first assessment will determine risk levels, provide parental/caregiver education, and create individual treatment protocols to decrease the incidence of early childhood caries.1 Beginning these interventions before the child’s first birthday is a critical factor in their effectiveness.
Besides early childhood caries having a major impact on children’s health, it adds significant costs to society. Treatment of early childhood caries often requires extensive restorative treatment, extraction of primary teeth, space maintenance, and there can be substantial costs for sedation or general anesthesia in cases in which the child may be precooperative for treatment in the dental chair. The U.S. Medical Expenditures Survey found that dental expenditures exceeded $1.55 billion in 2010 for children younger than 5.9 Approximately $450 million additional expenditures occurred in 2011 because of hospital operating room costs related to early childhood caries.10
MANAGEMENT STRATEGIES
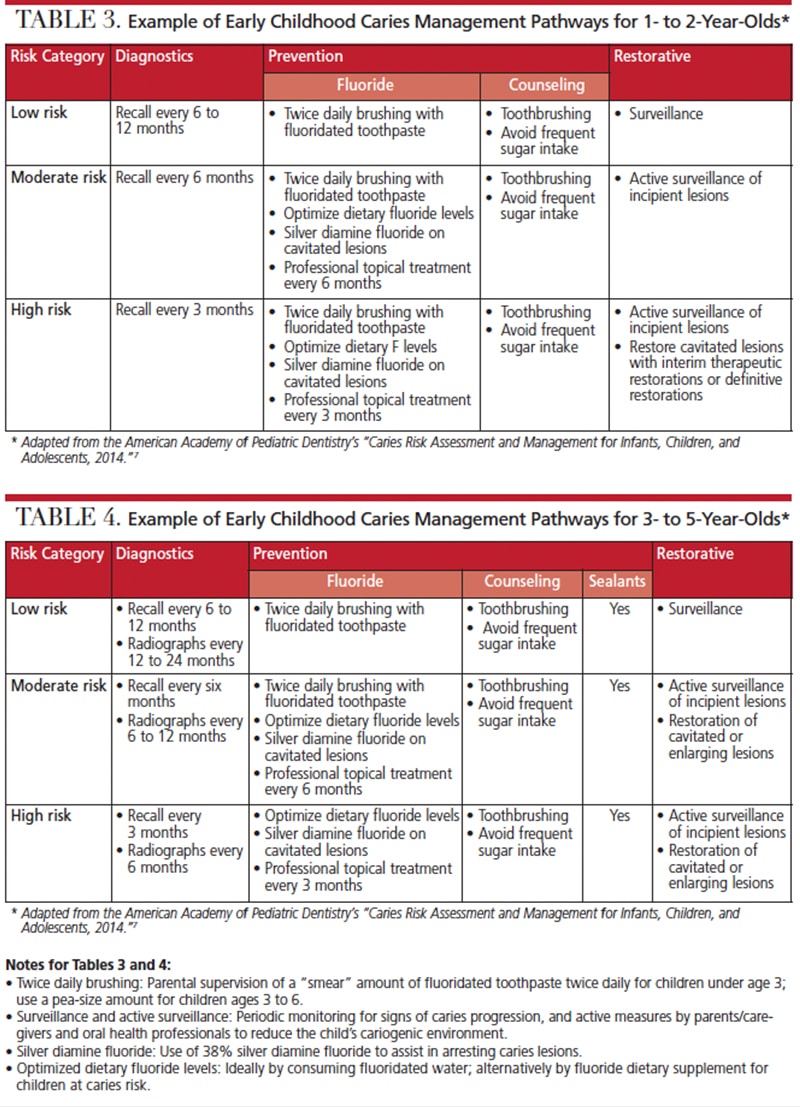
Dental professionals are uniquely positioned to help reduce or prevent early childhood caries by providing parents and caregivers with management strategies, such as instructions regarding toothbrushing and sugar restrictions. Furthermore, the use of risk assessment strategies and care pathways to establish appropriate recall schedules, optimize fluoride treatments, provide sealants on primary teeth, promote surveillance (periodic monitoring for caries progression), and referral, when necessary, will help prevent caries lesions.
Preventive strategies include:
Motivational interviewing techniques were first described in the 1980s as a method of reflective listening, empathy, and provoking self-exploration.11 The goal for this counseling technique for early childhood caries prevention is to optimize parents’/caregivers’ behavior changes with regard to the child’s sugar consumption and oral hygiene. Use of motivational interviewing to improve health behaviors is based on the premise that an individual takes ownership and responsibility for his/her behavior change. When utilizing motivational interviewing for behavior changes, the caregiver’s interest, curiosity and appreciation of the message should be enhanced; therefore this technique aims for individuals to perceive the information as their own, thus more readily adopting behavior changes/strategies.
Relative to comparison groups, motivational interviewing has been associated with significant improvements in health behaviors, such as diet, physical activity, smoking cessation, body mass index and oral health. Results suggest this approach may outperform comparison groups in terms of dental caries.12 Recently, Colvara et al13 assessed the effectiveness of motivational interviewing techniques versus conventional oral health education in the prevention of early childhood caries in 3-year-old Brazilian children. After a 3-year study period, children in the motivational interviewing group had 53% fewer caries than the control group.13
Dietary counseling aims to help parents/caregivers improve their child’s dietary behaviors to favor low- or noncariogenic snacks, drink fluoridated water, and limit sugar-containing foods to mealtimes. Such dietary recommendations must be realistic and based upon the dietary norms of the family. An extensive study using clinical food intake surveys and microbial data of 72 Boston children with severe early childhood caries found the disease was associated with between-meal juice consumption, drinking less milk between meals, eating at bedtime or during the night, and not eating caries-protective foods.14 Examples of low cariogenic foods include cheese, crunchy fruits and vegetables, nuts and nut butters.
Fluoride exposure and fluoride application are effective means of preventing caries. Fluoridation of community drinking water is the most equitable and cost-effective method of delivering fluoride to members of the community.15 Water fluoridation at the level of 0.7 to 1.2 mg fluoride ion/L (ppm F) was introduced in the U.S. in the 1940s. Because fluoride from water supplies is now one of several sources of fluoride, the U.S. Department of Health and Human Services has standardized optimal fluoride levels in water to 0.7 ppm. The rationale is to balance the benefits of preventing dental caries while reducing the chance of fluorosis.16 Dietary fluoride supplements are also effective in reducing prevalence of dental caries and should be considered for children at high caries risk who drink fluoride-deficient (less than 0.6 ppm F) water.17 Infant formulas requiring reconstitution with water have raised concerns regarding an increased risk of fluorosis.18 Standardization of the optimal fluoride levels in drinking water to 0.7 ppm F, however, makes this issue less important.
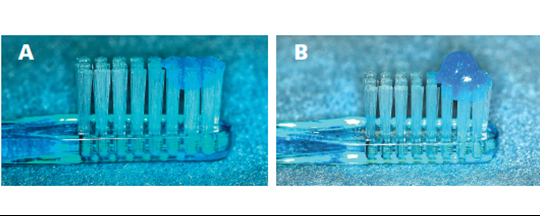
The most widely used method of applying fluoride topically is via toothpaste. Systematic reviews have shown that in 3- to 6-year-olds, daily toothbrushing with fluoridated toothpaste significantly reduces caries incidence.19 To reduce the risk of fluorosis in preschool children, the American Dental Association (ADA) Council on Scientific Affairs recommends children under age 3 have their teeth brushed twice a day using a “smear” of toothpaste, and children ages 3 to 6 have their teeth brushed twice a day using a pea-sized amount of toothpaste20 (Figures 2A and 2B).
The most commonly used agents for professionally applied fluoride treatments are 5% sodium fluoride varnish (NaFV; 2.26% F, 22,600 ppm F) and acidulated phosphate fluoride (1.23% F, 12,300 ppm F). Unit doses of fluoride varnish are the only professional topical fluoride agent that are now recommended for children younger than 6 because the 0.25-ml unit dose contains only 5.5 mg of fluoride.21

Silver diamine fluoride (SDF) is indicated for treating dentinal hypersensitivity, but is also frequently used to arrest caries. This agent arrests caries by the antibacterial effect of silver and remineralization of enamel and dentin.22 The only reported side effect of SDF is that caries lesions will stain black following treatment (Figure 3). Because this discoloration of the teeth may be objectionable to parents/caregivers, it is recommended that consent forms that show pictures of the treatment effect be obtained before application of SDF. See Table 2 for a summary of topical fluoride products for preschool children.
Pit-and-fissure sealants have been used since the early 1970s to prevent and control caries lesions, primarily in permanent teeth. The recent joint ADA and American Academy of Pediatric Dentistry clinical guideline now gives strong recommendation to the use of pit-and-fissure sealants on fissure surfaces of both primary and permanent molars that have clinically sound occlusal surfaces or noncavitated caries lesions.23
ACCESS-TO-CARE PATHWAYS
Pediatricians, nurse practitioners, obstetricians and family physicians generally see the caregiver and child much earlier than oral health professionals. Engaging dental professionals in collaborative care with other health care providers and delegating areas of the care pathway to the interprofessional team can provide better outcomes for preventing early childhood caries. Currently, almost all states reimburse (through Medicaid) primary medical providers for oral health preventive visits. In a study to improve physician participation in oral health programs, Boylston-Herndon et al24 studied the effects of training pediatricians and family physicians in oral health procedures. Results showed in-office training improved physician confidence in conducting dental caries risk assessment, and oral health screening and oral health knowledge. Because fluoride varnish application was not reimbursed at time of the project, this procedure was not studied.24
According to Fried,25 collaboration between medical and dental providers has been shown to have a positive effect on patient outcomes, as this model can facilitate earlier risk assessment and care. For parents and caregivers of preschool children, collaborative practice allows timely referrals and counseling on preventive oral health behaviors; and for children, better access to screenings and topical fluoride application.
CONCLUSION
Early childhood caries is a complex, multifactorial disease that continues to be the most chronic disease of childhood. Consequences include increased risk for more caries lesions, and, in severe cases, hospitalization and emergency department visits, high treatment costs, and reports of delays in growth and development. This condition also diminishes quality of life.
The medical/dental team must carefully assess the risk factors that subsequently lead to evidence-based care pathways to manage the disease process. Dental professionals, utilizing their expertise in prevention, are in a unique position to lead the team in providing care and early interventions for this young population.
REFERENCES
- American Academy of Pediatric Dentistry. Policy on Early Childhood Caries (ECC): Classifications, Consequences, and Preventive Strategies, 2016. Available at: aapd.org/media/Policies_Guidelines/P_ECCClassifications.pdf. Accessed August 6, 2018.
- Dye BA, Tan S, Smith V, et al. Trends in oral health status: United States, 1988–1994 and 1999–2004.Vital Health Stat 11. 2007;248:1–92.
- Anil S, Anand PS. Early childhood caries: Prevalence, risk factors, and prevention. Front Pediatr. 2017;5:157.
- Tinanoff N, Reisine S. Update on early childhood caries since the Surgeon General’s Report. Acad Pediatr. 2009;9:396–403.
- Fass EN. Is bottle-feeding of milk a factor in dental caries? J Dent Child. 1962;24:245–251.
- Tinanoff N. Introduction to the Early Childhood Caries Conference: Initial description and current understanding. Community Dent Oral Epidemiol. 1998;26 (Suppl 1):5–7.
- American Academy of Pediatric Dentistry. Caries Risk Assessment and Management for Infants, Children, and Adolescents, 2014. Available at: aapd.org/media/Policies_Guidelines/BP_CariesRiskAssessment.pdf. Accessed August 6, 2018.
- Douglass JM, Li Y, Tinanoff N. Association of mutans streptococci between caregivers and their children. Pediatr Dent. 2008;30:375–387.
- Agency for Healthcare Research and Quality. Dental Expenditures in the 10 Largest States, 2010 Available at: meps.ahrq.gov/data_files/publications/st415/stat415.pdf. Accessed August 6, 2018.
- Bruen BK, Steinmetz E, Bysshe T, Glassman P, Ku L. Potentially preventable dental care in operating room for children enrolled in Medicaid. J Am Dent Assoc. 2016;147:702–708.
- Moyers TM. History and happenstance: how motivational interviewing got its start. J Cognitive Psychotherapy. 2004:18:291–298.
- Borelli B, Tooley EM, Scott-Shelton LA. Motivational interviewing for parent-child health interventions: a systematic review and meta-analysis. Pediatr Dent. 2015;37:254–265.
- Colvara BC, Faustino-Silva DD, Meyer E, Hugo FN, Hilgert JB, Celeste RK. Motivational interviewing in preventing early childhood caries in primary healthcare: A community–based randomized cluster trial. J Pediatr. 2018;18:30672–30673.
- Palmer CA, Kent R, Loo CY, et al. Diet and caries-associated bacteria in severe early childhood caries. J Dent Res. 2010;89:1224–1229.
- From the Centers for Disease Control and Prevention. Achievements in public health, 1900–1999; fluoridation of drinking water to prevent dental caries. JAMA. 2000;283:1283–1286.
- U.S. Department of Health and Human Services Federal Panel on Community Water Fluoridation. U.S. Public Health Service recommendation for fluoride concentration in drinking water for the prevention of dental caries. Public Health Rep. 2015;130:318–331.
- Rozier RG, Adair S, Graham F, et al. Evidence-based clinical recommendations on the prescription of dietary fluoride supplements for caries prevention: a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2010;141:1480–1489.
- Hujoel PP, Zina LG. Moimas SA, Cunha-Cruz J. Infant formula and enamel fluorosis. A systematic review. J Am Dent Assoc. 2009;140:841–854.
- dos Santos AP, Nadanovsky P, de Oliveira BH. A systematic review and meta-analysis of the effects of fluoridated toothpastes on the prevention of dental caries in the primary dentition of preschool children. Community Dent Oral Epidemiol. 2013;41:1–12.
- Wright JT, Hanson N, Ristic H, et al. Fluoride toothpaste efficacy and safety in children younger that 6 years. J Am Dent Assoc. 2014;145:182–189.
- Weyant RJ, Tracy SL, Anselmo T, et al. Topical fluoride for caries prevention: executive summary of the updated clinical recommendations and supporting systematic review. J Am Dent Assoc. 2013:144:1279–1291.
- Zhao IS, Gao SS, Hiraishi N, et al. Mechanisms of silver diamine fluoride on arresting caries: a literature review. Int Dent J. 2018;68:67–76.
- American Academy of Pediatric Dentistry and American Dental Association. Use of Pit-and-Fissure Sealants, 2016. Available at: aapd.org/media/Policies_Guidelines/G_Sealants.pdf. Accessed August 6, 2018.
- Herndon JB, Tomar SL, Catalanotto FA. Effect of training pediatricians and family physicians in early childhood caries prevention. J Pediatr. 2015;166:1055–1061.
- Fried J. Interprofessional collaboration: if not now, when? J Dent Hyg. 2013;87 (Suppl 1):41–44.
From Decisions in Dentistry. October 2018;4(10):31–34.

