

Oral Complications in Children With Diabetes
The following clinical strategies can help improve the oral and systemic health of this patient population.
The following clinical strategies can help improve the oral and systemic health of this patient population
PURCHASE COURSE
This course was published in the April 2017 issue and expires April 2020. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Describe the epidemiology of diabetes in pediatric patients, and common oral complications in this population.
- Explain the pathophysiology of diabetes, and its potential impact on oral health.
- Discuss research that indicates parents and caregivers of children with diabetes may not be aware of the relationship between diabetes and oral health.
- Provide appropriate clinical care for children with diabetes.
Diabetes mellitus is the third most common chronic disease in children and adolescents.1 In the United States, about 208,000 people younger than 20 years of age have been diagnosed with type 1 or type 2 diabetes; this accounts for 0.25% of all people in this age group.1 During 2008–2009, an estimated 18,436 Americans younger than 20 were newly diagnosed with type 1 diabetes.1 This is the leading form of diabetes in children of all ages, and accounts for almost all diabetes in children younger than 10.2 Although type 2 diabetes is less common in children, the incidence is greater among youth ages 10 to 19 years than in younger children.1
Type 1 diabetes results from the autoimmune destruction of insulin-producing pancreatic b-cells, creating a deficiency of circulating insulin. Consequently, insulin injections are required to maintain normal blood glucose levels and prevent metabolic complications from the excess serum glucose — particularly life-threatening diabetic ketoacidosis. Often, clinical symptoms are sudden onset. Type 2 diabetes results from insulin resistance, in which insulin receptors are not sufficiently sensitive for insulin to bind to the cell and allow glucose uptake. This impairs insulin action and glucose regulation. Although type 2 diabetes is often considered to be an adult-onset disease that evolves over several years, increasing numbers of children are being diagnosed with this disease, a reflection of the increased number of overweight or obese children in recent years.
In both children and adults, obesity increases the risk of developing type 2 diabetes.3 Symptoms of both types of diabetes include fatigue, weight loss, polyuria and polydipsia, resulting from hyperglycemia. Excess blood glucose, in fact, is used as one of the diagnostic criteria. Diabetes is diagnosed by fasting blood glucose levels greater than 126 mg/dl, or a two-hour plasma glucose greater than 200 mg/dl during an oral glucose tolerance test.3 The hemoglobin A1c (HbA1c) test measures the levels of glucose bound to hemoglobin in erythrocytes. Test readings greater than 6.5% indicate hyperglycemia. And because these values provide average blood glucose levels over a two- to three-month period, they are useful for monitoring overall glycemic control. In hemoglobin A1c testing, readings of 6.5% and below indicate good glycemic control, while readings of 7% and above indicate poor control. Blood glucose is regulated by insulin, and one of its functions is to facilitate transport of glucose from the bloodstream into the target tissues, where it provides energy and aids the process of storing excess glucose as glycogen. Impairing insulin secretion and/or action causes chronic hyperglycemia, which affects multiple metabolic processes, including systemic inflammation. These factors are responsible long-term consequences, such as microvascular diseases (e.g., retinopathy, nephropathy and neuropathy), macrovascular diseases (e.g., cardiovascular and cerebrovascular conditions), increased susceptibility to infections, poor wound healing and periodontal disease.
BIDIRECTIONAL RELATIONSHIP
The association between diabetes and periodontal disease has been studied extensively. A meta-analysis of 57 peer-reviewed studies of adults with type 2 diabetes concluded its presence in adults is a risk factor for periodontitis.4 Based on recent systematic and comprehensive reviews of studies of children with diabetes, these children are also at risk for developing periodontal disease.5,6 Compared with nondiabetic children, pediatric patients with diabetes have been reported to exhibit significantly greater gingival inflammation and clinical attachment loss.7,8 This periodontal destruction can begin very early in life and become more prominent as the child enters into adolescence.8
While this evidence indicates diabetes adversely affects periodontal health, other studies have shown that periodontal infections can also affect glycemic control in individuals with diabetes. A systematic review of the evidence led to the conclusion that poor periodontal health adversely affects diabetes outcomes, and that the relationship between diabetes and periodontal disease is bidirectional.9 The link between them may be chronic systemic inflammation.
The chronic hyperglycemia observed in individuals with diabetes triggers the formation of systemic inflammatory mediators that circulate throughout the body, including the periodontium. This stimulates the periodontal cells to produce a local inflammatory response that exaggerates the existing inflammatory response induced by periodontal pathogens. This is especially true in obese individuals with type 2 diabetes, in whom inflammatory mediators produced by abdominal tissue cells trigger systemic and local inflammatory responses.10 Inflamed periodontal tissues have numerous detrimental effects, such as increasing bone resorption and decreasing bone formation, resulting in the net loss of alveolar bone. Hyperglycemia’s role in this process is underscored by evidence that a higher prevalence of periodontal destruction has been observed in adults and children with poorly controlled glucose levels11–13 (as determined by HbA1c levels greater than 9%,11 9.5%12 or 10%13).
As previously noted, periodontal infections can affect glycemic control in individuals with diabetes by serving as a source of chronic systemic inflammation. Periodontal pathogens — especially Gram-negative bacteria — stimulate periodontal tissue cells to synthesize and release local proinflammatory mediators. These mediators, as well as bacteria and their by-products, circulate through the bloodstream and activate a systemic inflammatory response in the liver. This systemic inflammation can reduce tissue response to circulating insulin, thereby reducing glucose uptake by cells and causing hyperglycemia. Several systematic reviews with meta-analyses have shown the effectiveness of periodontal treatment in improving glycemic control. While a recent critical assessment of these reviews found similar results, due to methodological limitations, the authors concluded more research is needed before establishing any conclusions about this relationship.14
ADDITIONAL CONSIDERATIONS
Common oral complications of diabetes include xerostomia, candidiasis and delayed wound healing. Xerostomia is the most common oral complication of the disease in children, with dry mouth symptoms experienced by 53% of adolescents with diabetes.15 Salivary dysfunction has been associated with poor glucose control in diabetic patients. The presence of hyperglycemia affects the biochemical composition of saliva, which contributes to considerably lower salivary flow rate, reduced pH (and, thus, buffering capacity), and yeast growth.16 In addition, hyperglycemic episodes increase salivary concentrations of glucose, causing the oral environment to become more favorable to cariogenic bacteria, such as lactobacilli and mutans streptococci.17 Thus, hyperglycemia appears to be a factor in the development of caries. A higher prevalence of caries has been reported in children with poorly controlled diabetes (HbA1c values greater than 8%,18 9%,16 or 10%13) than in children with moderate-to-good levels of control.13,16,18 Yet recent reviews comparing caries experience indicate contradictory results; that is, children with diabetes have been reported to have higher, lower or the same prevalence of caries as their peers without diabetes.5,6
One possible explanation for a lower prevalence of caries in children with diabetes may be their sucrose-restricted diet. Dietary recommendations for children with type 1 diabetes include avoiding refined sugar, and consuming an even distribution of complex carbohydrates throughout the day.19 In addition to increased exercise to promote weight loss, a healthy diet consisting of low-sugar content, complex carbohydrates — and small portions — is also recommended for children with type 2 diabetes.
ORAL HEALTH EDUCATION
Due to their increased risk for periodontal disease and impaired salivary function, children with diabetes should undergo extensive preventive measures at an early age. These risks have not always been recognized by their parents and caregivers,20 which is a concern because parents/caregivers play a significant role in children’s oral health. Findings from a recent study demonstrate that parents/caregivers of children with diabetes were not aware of the relationship between diabetes/glycemic control and periodontal disease.20 Adolescents with diabetes also have been reported to lack knowledge of the effects of diabetes on oral health.21–23 In addition, oral health care may be less of a priority for this population due to the focus on the medical aspects of the disease. Even though parents/caregivers of children with diabetes did not recognize the condition might compromise their child’s oral health, they considered this information to be important.20 Thus, oral health education is critical to provide the knowledge to properly care for their child’s (and their own) oral health, and prevent the oral complications of the disease.
Periodontal disease and caries are largely preventable, and interventions are least invasive and tend to be most successful when these conditions are recognized in their early stages. Therefore, it is critical for children with diabetes to establish good oral hygiene habits at an early age. Type 1 diabetes can be diagnosed at any age (e.g., as early as infancy), and the duration of diabetes has been associated with the prevalence of periodontal disease12,22 and caries.22 Although meticulous oral hygiene is crucial, adolescents with type 1 diabetes have been reported to have suboptimal oral hygiene behaviors,21,23 which is concerning because regular toothbrushing and use of mouthrinse have been related to glycemic control.21 Oral health education should stress the importance of frequent brushing and interdental cleaning, the use of fluoride toothpaste and mouthrinse, and the need for supervision of oral hygiene for children younger than 6. In older children, the use of xylitol gums or lozenges may be beneficial to increase salivary flow and reduce acidogenic bacteria. Professionally applied sealants and fluoride varnish are also recommended to further reduce caries risk.
Regular professional care is important for prevention, early detection and treatment of oral complications in children with diabetes. Because these children are at risk for periodontitis, their gingival tissue should be closely monitored. Oral health professionals should emphasize the importance of regular dental visits by focusing on the fact that children with diabetes are more likely than nondiabetic children to experience periodontal disease.
PATIENT MANAGEMENT
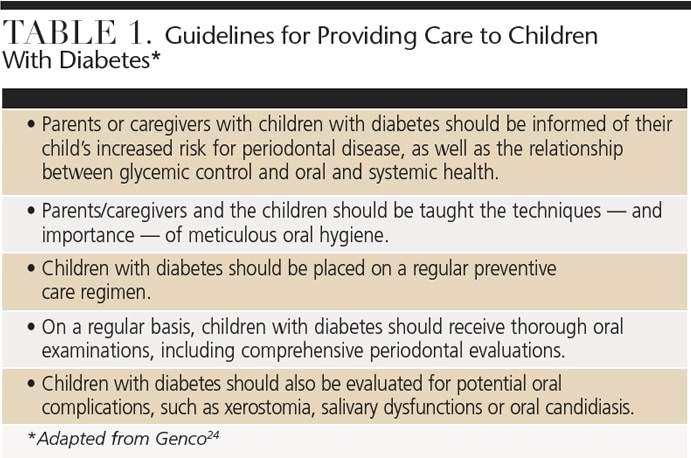
Table 1 provides guidelines for oral health professionals who care for children with diabetes. To avoid a diabetic emergency, appointments should be scheduled so they neither concur with peak insulin levels, nor interfere with the patient’s medication and eating schedules. In general, morning appointments approximately 60 to 90 minutes after breakfast are ideal. At the beginning of the appointment, a thorough health history should be obtained, including the type of diabetes, date of diagnosis, methods used to control diabetes, current medications and dosages, last visit with a physician, the frequency of hypoglycemic episodes, and recent glycemic control (as indicated by the level of glycated hemoglobin.24
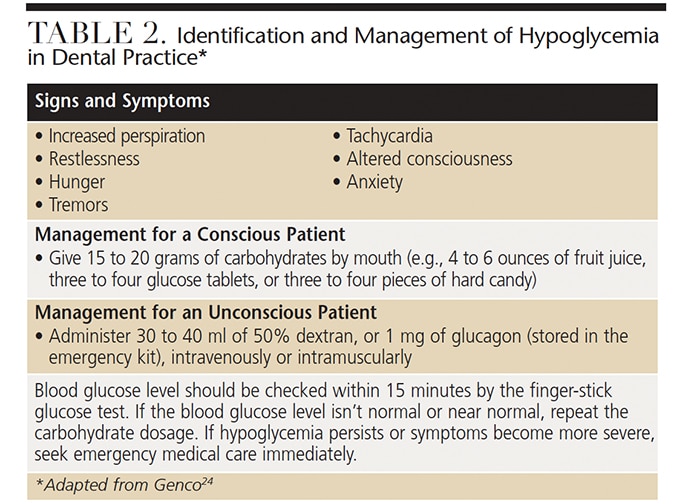
Because the HbA1c test averages blood glucose over the preceding two- to three-month period, the readings do not necessarily indicate the patient’s blood glucose level at the time of the appointment. Levels fluctuate throughout the day, so it is important for clinicians to know these levels prior to the start of treatment. Measuring blood glucose levels with a finger-stick glucose test or glucometer is a quick and standard way to determine whether the patient may be likely to experience a diabetic emergency. Hypoglycemia is a common medical emergency for individuals with type 1 diabetes. Symptoms generally present when the patient has skipped or delayed meals, resulting in readings below the normal lower blood glucose limit of 70 mg/dl. Clinicians should be prepared to identify and manage a hypoglycemic episode in the dental office, as described in Table 2. Hyperglycemia is a less common — but more serious complication — which is generally seen in those who are insulin dependent. Without intervention, hyperglycemia can progress to diabetic ketoacidosis, which can be life threatening. Thus, if the patient’s blood glucose levels are chronically elevated (> 126 mg/dl), professional oral care should be postponed and the patient referred to a physician.24
CONCLUSION
Diabetes, especially poorly controlled blood glucose levels, is detrimental to oral health. Children with diabetes are at elevated risk for periodontal disease, and any periodontal infections may adversely affect glycemic control. Poorly controlled diabetes also increases the risk of caries, possibly due to impaired salivary function and an increased numbers of cariogenic pathogens. Dental professionals can provide the extensive preventive and therapeutic care needed to maintain the health of oral tissues in this patient population. At the same time, parents/caregivers of children with diabetes need to be informed of the significant contribution of oral health to their children’s long-term systemic health.
References
- U.S. Centers for Disease Control and Prevention. 2014 National Diabetes Statistics Report. Available at: cdc.gov/diabetes/data/statistics/2014statisticsreport.html. Accessed March 1, 2017.
- National Diabetes Education Program. Overview of Diabetes in Children and Adolescents; 2014. Available at: niddk.nih.gov/health-information/health-communication-programs/ndep/living-with-diabetes/youth-teens/diabetes-children-adolescents/Documents/overview- of-diabetes-children_508_2016.pdf. Accessed March 1, 2017.
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2012;35:S64–S71.
- Chavarry NG, Vettore MV, Sansone C, Sheiham A. The relationship between diabetes mellitus and destructive periodontal disease: A meta-analysis. Oral Health Prev Dent. 2009;7:107–127.
- Ismail AF, McGrath CP, Yiu CK. Oral health of children with type 1 diabetes mellitus: a systematic review. Diabetes Res Clin Pract. 2015;108:369–381.
- Novotna M, Podzimek S, Broukal Z, Lencova E, Duskova J. Periodontal diseases and dental caries in children with type 1 diabetes mellitus. Mediators Inflamm. 2015;2015:379626.
- Lalla E, Cheng B, Lal S, et al. Diabetes mellitus promotes periodontal destruction in children. J Clin Periodontol. 2007;34:294–298.
- Lalla E, Cheng B, Lal S, et al. Periodontal changes in children and adolescents with diabetes: A case-control study. Diabetes Care. 2006;29:295–299.
- Borgnakke WS, Ylostalo PV, Taylor GW, Genco RJ. Effect of periodontal disease on diabetes: systematic review of epidemiologic observational evidence. J Periodontol. 2013;84:S135–S152.
- Mealey BL, Oates TW, American Academy of Periodontology. Diabetes mellitus and periodontal diseases. J Periodontol. 2006;77:1289–1303.
- Tsai C, Hayes C, Taylor GW. Glycemic control of type 2 diabetes and severe periodontal disease in the U.S. adult population. Community Dent Oral Epidemiol. 2002;30:182–192.
- Lalla E, Cheng B, Lal S, et al. Diabetes-related parameters and periodontal conditions in children. J Periodontal Res. 2007;42:345–349.
- Carneiro VL, Fraiz FC, Ferreira Fde M, Pintarelli TP, Oliveira AC, Boguszewski MC. The influence of glycemic control on the oral health of children and adolescents with diabetes mellitus type 1. Arch Endocrinol Metab. 2015;59:535–540.
- Faggion CM Jr, Cullinan MP, Atieh M. An overview of systematic reviews on the effectiveness of periodontal treatment to improve glycaemic control. J Periodontal Res. 2016;51:716–725.
- Busato IM, Ignacio SA, Brancher JA, Moyses ST, Azevedo-Alanis LR. Impact of clinical status and salivary conditions on xerostomia and oral health-related quality of life of adolescents with type 1 diabetes mellitus. Community Dent Oral Epidemiol. 2012;40:62–69.
- Siudikiene J, Machiulskiene V, Nyvad B, Tenovuo J, Nedzelskiene I. Dental caries and salivary status in children with type 1 diabetes mellitus, related to the metabolic control of the disease. Eur J Oral Sci. 2006;114:8–14.
- Siudikiene J, Machiulskiene V, Nyvad B, Tenovuo J, Nedzelskiene I. Dental caries increments and related factors in children with type 1 diabetes mellitus. Caries Res. 2008;42:354–362.
- Twetman S, Johansson I, Birkhed D, Nederfors T. Caries incidence in young type 1 diabetes mellitus patients in relation to metabolic control and caries-associated risk factors. Caries Res. 2002;36:31–35.
- Gilbertson HR, Brand-Miller JC, Thorburn AW, Evans S, Chondros P, Werther GA. The effect of flexible low glycemic index dietary advice versus measured carbohydrate exchange diets on glycemic control in children with type 1 diabetes. Diabetes Care. 2001;24:1137–1143.
- Sohn HA, Rowe DJ. Oral health knowledge, attitudes and behaviors of parents of children with diabetes compared to those of parents of children without diabetes. J Dent Hyg. 2015;89:170–179.
- Merchant AT, Oranbandid S, Jethwani M, et al. Oral care practices and A1c among youth with type 1 and type 2 diabetes. J Periodontol. 2012;83:856–863.
- Rafatjou R, Razavi Z, Tayebi S, Khalili M, Farhadian M. Dental health status and hygiene in children and adolescents with type 1 diabetes mellitus. J Res Health Sci. 2016;16:122–126.
- Orlando VA, Johnson LR, Wilson AR, et al. Oral health knowledge and behaviors among adolescents with type 1 diabetes. Int J Dent. 2010;2010:942124.
- Genco RJ. Oral health and Diabetes. In: Glick M, ed. The Oral-Systemic Health Connection. Hanover Park, IL: Quintessence Publishing Co Inc; 2014:120–137.
Featured photo by AMR Image / istock / Getty Images Plus
From Decisions in Dentistry. April 2017; 3(4):46–49.

