

Nutritional Assessment and Oral Health
Dietary choices can positively — or negatively — impact oral health. Clinicians can help by identifying and managing risk, and providing appropriate dietary counseling.
Dietary choices can positively — or negatively — impact oral health. Clinicians can help by identifying and managing risk, and providing appropriate dietary counseling
PURCHASE COURSE
This course was published in the August 2016 issue and expires 08/31/19. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Define the impact of diet on oral health.
- Discuss how to perform nutritional assessment and provide
dietary counseling in the dental setting. - Identify strategies to help patients understand how dietary
changes may improve their oral health.
Ideally, all members of the dental team serve as health care educators, and this instruction should include diet and nutrition counseling for the prevention and treatment of oral health conditions. Diet, defined as the combination of foods and beverages consumed, may impact caries risk, soft tissue health, and responses to injury and infection. Nutrients contained within foods are essential for growth, maintaining tissue health, repairing injured tissue, and providing energy for daily activities. Oral health professionals should recognize dietary contributors to disease, and routinely assess and manage nutrition-related risks.
Dental caries is a disease in which the acid produced by oral microorganisms dissolves enamel or dentin in a specific location. Oral pathogens cannot ferment proteins, fats or nonnutritive sweeteners, such as aspartame and sucralose.1 As such, carbohydrates are considered cariogenic, while proteins, fats and nonnutritive sweeteners are considered noncariogenic. Dietary carbohydrates at risk for fermentation include sugars, starches and hydrolyzed starch products.2,3 Common dietary sugars include glucose, fructose, sucrose and lactose. Starches are long saccharide chains that are made from sugars. They are found in grains, vegetables and baked goods. Intermediary carbohydrates produced by the hydrolysis of starches are also fermentable by oral microbes. Hydrolysis — the splitting of large carbohydrates into small carbohydrates through the addition of water — slowly severs the bonds of starch molecules. This results in fewer saccharide units per molecule. On food labels, hydrolyzed sugars are called modified starches, oligosaccharides and maltodextrins.
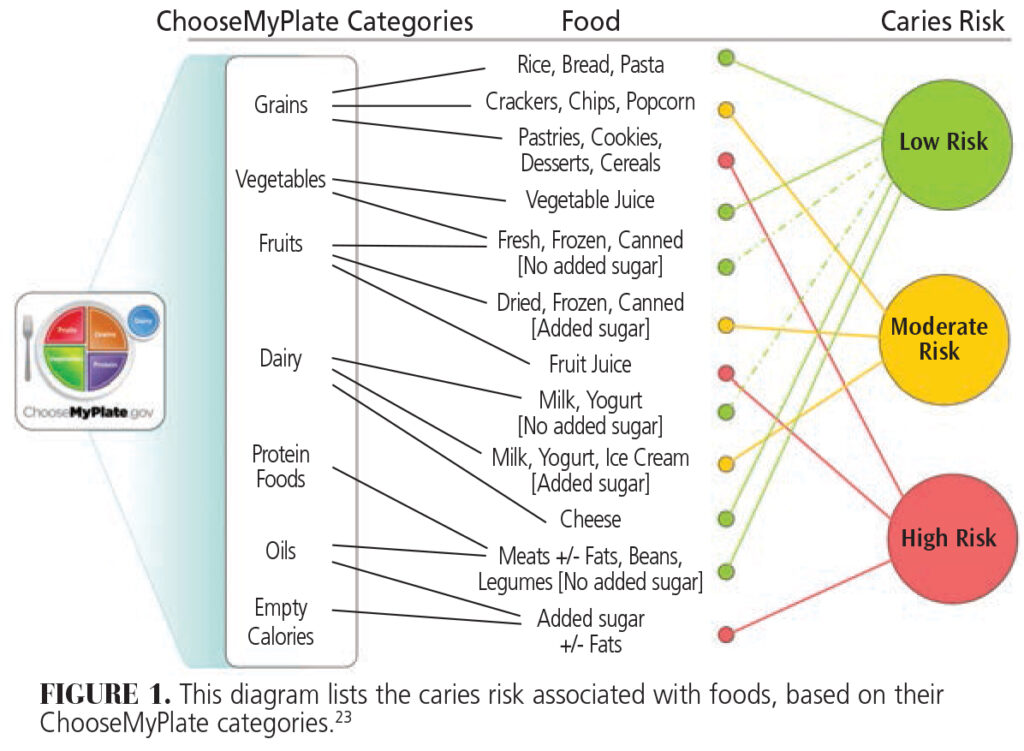
The caries risk associated with foods depends on their carbohydrate composition and manner of consumption (Figure 1). Typically, unsweetened grains, vegetables, fruits and dairy products present low caries risk. Foods containing added sugars and/or hydrolyzed starch products, however, are associated with increased caries risk.3 Although potato chips, crackers and cereals may not contain sugars, they do have oligosaccharides (saccharide polymers composed of three to 10 simple sugars) and maltodextrins (polysaccharides used as food additives). These can, in time, be fermented by the oral microbiota. Beverages made with natural sugars or added sugars are associated with higher caries risk than solid foods containing sugars.4–6
Consumption behaviors can also modify caries risk.5,7 Behaviors that limit exposure to cariogenic foods/beverages decrease caries risk, while behaviors that increase exposure raise caries risk. Structured meals and snacks with no more than five to six eating events per day tend to decrease risk, while unstructured eating events, “grazing” and sipping sugar-sweetened beverages increase caries risk. Certain oral habits, such as swishing beverages, holding foods and beverages in the mouth, and pocketing foods in the cheek, are associated with increased caries risk.
A significant reduction or elimination of foods containing added sugars is a prudent dietary goal. When added sugar is consumed, behaviors that limit oral exposure time —such as brief, structured eating intervals, prompt swallowing of chewed food, and the use of straws — tend to decrease caries risk. In addition, rinsing with water, chewing sugar-free gum, and appropriate oral hygiene practices also reduce caries risk.
The source of acids that cause erosion of enamel and/or dentin can be either exogenous (dietary) or endogenous (gastrointestinal). Soft drinks, 100% fruit juices, juice drinks, wine, herbal teas and sports drinks are all highly acidic.8,9 Foods associated with increased erosion risk include fruits (particularly citrus), sour candies, and foods prepared with vinegar, wine or acidic spices.8,10 To prevent diet-related erosion, exposure to acidic foods or beverages must be limited. In order to allow saliva to neutralize the oral cavity, patients should be advised to wait to brush their teeth for at least 20 minutes following consumption of acidic foods and beverages.
DIET AND PERIODONTAL DISEASE
Although periodontitis is a bacterial plaque-related condition, nutrition can influence susceptibilities to the disease. Conversely, prevention and treatment of periodontal disease depends on a functioning immune system — which, in turn, depends on appropriate nutrition. Nutrition-related conditions, including obesity and poorly controlled diabetes, increase the risk of periodontal disease.
Adequate energy (calories) and protein are necessary for daily activities and metabolic functions. Without adequate energy or protein, individuals become lethargic, growth slows, wound healing is impaired, and susceptibility to infection increases. Many nutrients have essential functions that support the immune system.11,12 Although the consequences of extreme nutrient deficiencies are well known, the implications of subtle nutrient deficiencies in relation to periodontal disease are less clear. In general, periodontal disease is more common and severe in individuals with protein-energy malnutrition compared to properly nourished individuals.11 Vitamin C deficiency has been associated with increased bleeding on probing, while high serum vitamin C levels have been linked to reduced risk of periodontitis in both smokers and nonsmokers.12 Similarly, low calcium and vitamin D intake may be related to periodontitis.11,12
Obesity and poorly controlled diabetes are thought to support a proinflammatory state and increase susceptibilities to infections, such as periodontitis. The size of fat cells correlates with the inflammatory markers tumor necrosis factor-α and interleukin-6 in young children.13 Excess weight and waist circumference are associated with increased risks for periodontitis in late adolescence.14 A high body mass index increases the risk of periodontitis in adults.15 In addition, the relationship between chronic periodontitis and poorly controlled diabetes is well established.11,16
The U.S. Department of Agriculture’s (USDA) Dietary Guidelines for Americans provide general recommendations for healthy diets to reduce the rates and intensity of chronic disease.17,18 At ChooseMyPlate.gov, the USDA offers dietary recommendations based on age, gender and activity level.19 In general, deficient nutrient intakes should be corrected through dietary changes. Nutritional supplements may be appropriate for addressing deficiencies for short intervals, however. For example, individuals who smoke often have low serum vitamin C levels and might benefit from vitamin C supplements. In addition to selecting foods to meet nutrient requirements, dietary recommendations for weight management and glycemic control in patients with obesity and/or diabetes are designed to reduce inflammatory responses and the risk for periodontal disease.
NUTRITIONAL ASSESSMENT
Nutritional assessment is the first step in addressing diet with patients. Subsequent stages include planning and implementing interventions, and evaluating their effectiveness. The depth of this process depends on the goals of the assessment, which can range from helping patients make better food choices to identifying malnourished individuals. Although malnutrition suggests deficient intake of energy or nutrients, it can also stem from excessive intake of energy or nutrients, or an imbalance of nutrient consumption.20,21 Signs and symptoms of malnutrition can be overt or subclinical. Secondary causes are not necessarily associated with dietary intake — but, rather, are problems relating to the absorption, utilization or excretion of nutrients.
A nutritional assessment includes questions regarding the frequency of exposure to fermentable carbohydrates, history of sweetened beverage consumption, level of compliance with ChooseMyPlate recommendations, and history of weight loss or gain of more than 10 pounds during the preceding six months. Patients identified as high risk for malnutrition during the initial screening, or those who have diet-related conditions, should receive a more detailed nutritional assessment that includes an examination of medical, social and medication histories, anthropometrics, physical examination, and diet assessment. This information process provides the foundation for identifying appropriate interventions.
Historical information is typically obtained during patient interviews or from medical records, and identifies patient characteristics that influence food intake and/or nutrient requirements. Assessing medical histories is designed to identify illnesses and treatments or conditions that increase the risk of malnutrition. The assessment of socioeconomic history helps clinicians detect financial and environmental factors that limit a patient’s ability to buy or prepare appropriate foods. By evaluating medication usage, practitioners can consider whether supplements, over-the-counter medications, prescription medications and/or recreational drugs may cause nutrient-medication interactions.
Anthropometrics refer to measures of body size and proportion, which provide an indirect assessment of body composition. Weight and height are the most common measurements taken, but recording waist and hip circumference is increasingly common. Waist circumference or the waist-to-hip ratio can identify the presence of abdominal obesity, which is strongly associated with metabolic disorders, such as type 2 diabetes and cardiovascular disease.21 The relationship between weight and height (body mass index) may help to identify nutrition-related disorders.21
Physical examinations are visual evaluations of the color, shape, texture and symmetry of tissues.20,21 Inspection of body size and shape will reveal the presence of excesses fat tissue and/or loss of muscle or fat tissue. Dry skin, brittle hair, pale eyes and mottled nails are consistent with visible nutrient deficiencies. Changes to oral tissues — including magenta tongue, cracked lips or bleeding gums — also suggest nutrient deficiencies. In the assessment of dietary behaviors, current and past food consumption is recorded and compared to the nutritional guidelines provided by ChooseMyPlate to identify inadequate or excessive food intakes.19
The assessment of past food consumption helps clinicians detect nutrition issues that may have contributed to disease, but have since been corrected. For example, a patient recognized that his or her high intake of sugar-sweetened beverages was causing recurrent caries and took steps to eliminate these beverages from his or her diet. Dietary habits, such as meal patterns, location of consumption, and frequency of intake, are assessed to identify factors that influence the length of carbohydrate exposures. Before offering recommendations, dietary preferences, family and/or cultural dietary restrictions, and feeding skills should also be evaluated.
Dietary intake can be assessed by asking patients to recall what they have eaten over the past 24 hours or what they typically eat in a day, or through the use of food records and food frequency reports. Food records require patients to record their food consumption for three to seven days. While food records do not rely on memory, accuracy can be hindered by the tendency to overstate the consumption of healthy foods or omission of foods that are viewed as “bad.” Food frequency, which is based on patient memory, refers to the frequency and volume of food and beverages consumed. Most dietary assessment tools include questions about behaviors associated with food intake.
DIETARY COUNSELING
Dietary counseling includes the identification of dietary interventions to improve food choices and dietary behaviors.22 The information gathered during the nutrition assessment is used to determine which dietary factors may be contributing to current disease — or raising the risk of future disease. Following identification of risk factors, the patient’s diet and dietary behaviors are evaluated to identify strategies to modify food intakes and/or dietary behaviors to improve nutritional health.
Once strategies for modifying the diet are identified, patient counseling can begin. The patient should be informed of his or her oral health status, risk for oral diseases, and how dietary behaviors influence risk. Clinicians should also evaluate the individual’s general dietary knowledge so that appropriate education can be provided. In order to make informed decisions regarding behavioral changes, the patient needs to understand the relationship between oral health concerns and diet. After sharing the health status and dietary information, clinicians should identify the patient’s perceptions of any suspected dietary problems and how these may influence a willingness to modify the diet.
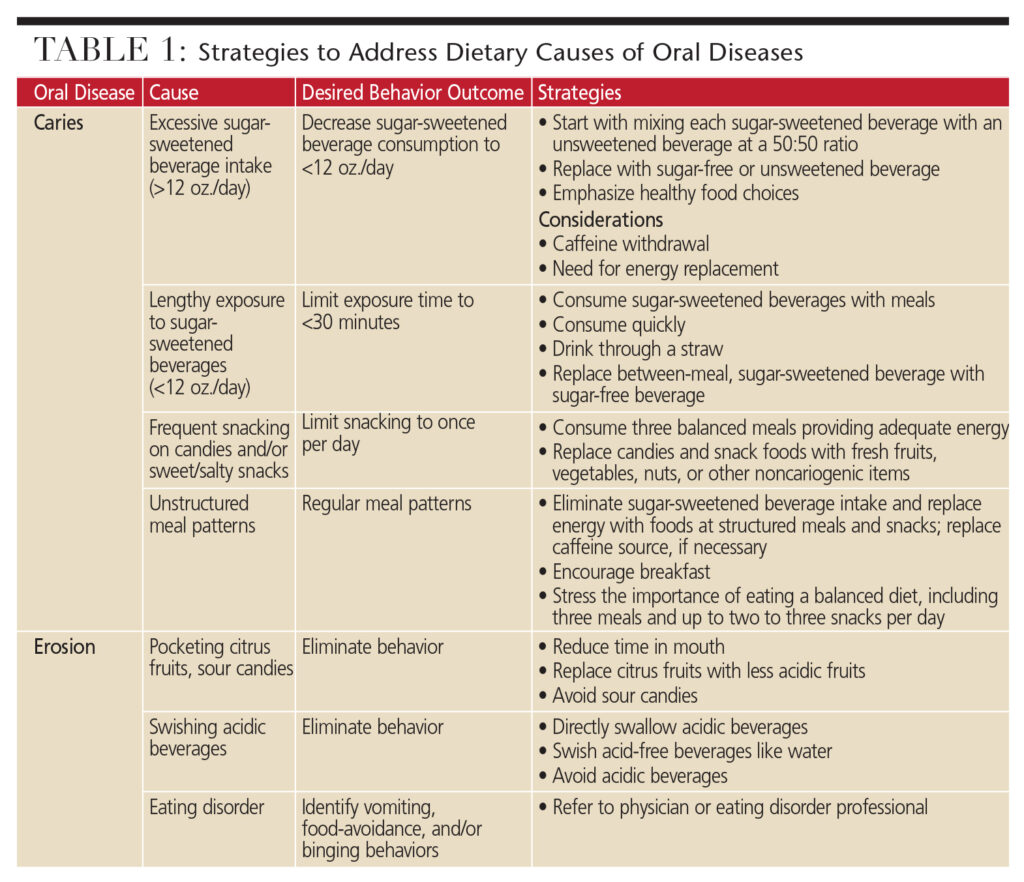
After identifying oral health concerns and dietary contributors, nutritional strategies to address disease and/or reduce risk are presented (Table 1). Change is difficult for most individuals, and multiple modifications are often required before an acceptable diet can be implemented. As such, the recommended strategies should be prioritized based on the most pressing health concerns. Patients should be provided with the desired behavior outcome and multiple strategies for achieving the outcome. Because food is not consumed in isolation, a change in one area of the diet often impacts other areas of dietary consumption. Thus, additional strategies should be presented as anticipatory guidance in advance of expected difficulties.22 In short, changing dietary behaviors is a gradual process and support is essential for success.
 Dietary counseling is not simply telling patients what to do. In order to be effective, it is a negotiation between the clinician and patient. Both the patient’s environment (including financial resources and food availability), and reserve capacity (the ability to take on additional emotional or physical stress and make the required time commitment), will affect his or her ability to comply with dietary changes. The clinician’s responsibility is to identify the problem, educate the patient about the disease-diet relationship, and provide strategies to address the issue. Implementation of the strategies to reduce oral disease, however, is the patient’s responsibility. To assist patients in achieving dietary change, both motivational interviewing and self-determination theory are appropriate counseling approaches.23
Dietary counseling is not simply telling patients what to do. In order to be effective, it is a negotiation between the clinician and patient. Both the patient’s environment (including financial resources and food availability), and reserve capacity (the ability to take on additional emotional or physical stress and make the required time commitment), will affect his or her ability to comply with dietary changes. The clinician’s responsibility is to identify the problem, educate the patient about the disease-diet relationship, and provide strategies to address the issue. Implementation of the strategies to reduce oral disease, however, is the patient’s responsibility. To assist patients in achieving dietary change, both motivational interviewing and self-determination theory are appropriate counseling approaches.23
CONCLUSION
Dental teams are responsible for providing dietary counseling for oral health and oral disease prevention consistent with the ChooseMyPlate recommendations. That said, some patients will present with systemic diseases, or educational or resource limitations that limit the team’s ability to address these issues. In these situations, dental professionals should refer patients to appropriate health care providers, such as registered dietitians, state cooperative extension specialists, or local food/nutrition educators. Patients with resource limitations should be informed of food assistance programs, local food banks, and/or free-meal programs.
Understanding the relationships between oral disease, nutritional intake and dietary behaviors is the foundation for patient education. Performing nutrition assessments to identify diet-related risk factors, and providing counseling or referrals to help patients address these risk factors are necessary to improve patients’ oral and systemic health.
References
- Marshall TA. Preventing dental caries associated with sugar-sweetened beverages. J Am Dent Assoc. 2013;144:1148–1152.
- Marshall TA. Nomenclature, characteristics, and dietary intakes of sugars. J Am Dent Assoc. 2015:146:61–64.
- Al-Khatib GR,Duggal MS, Toumba KJ. An evaluation of the acidogenic potential of maltodextrins in vivo. J Dent. 2001;29:409–414.
- Marshall TA, Levy SM, Broffitt B, et al. Dental caries and beverage consumption in young children. Pediatrics. 2003;112:e184–e191.
- Palmer CA, Kent R Jr., Loo CY, et al. Diet and caries-associated bacteria in severe early childhood caries. J Dent Res. 2010;89:1224–1229.
- Evans EW, Hayes C, Palmer CA, Bermudez OI, Cohen SA, Must A. Dietary intake and severe early childhood caries in low-income, young children. J Acad Nutr Diet. 2013;113:1057–1061.
- Marshall TA, Broffitt B, Eichenberger- Gilmore J, Warren JJ, Cunningham MA, Levy SM. The roles of meal, snack, and daily total food and beverage exposures on caries experience in young children. J Public Health Dent. 2005;65:166–173.
- Mallonee LFH, Boyd LD, Stegeman C. Practice Paper of the Academy of Nutrition and Dietetics. Oral Health and Nutrition. 2014;114:958.
- Ehlen LA, Marshall TA, Qian F, Wefel JS, Warren JJ. Acidic beverages increase the risk of in vitro tooth erosion. Nut Res. 2008;28:299–303.
- Wagoner SN, Marshall TA, Qian F, Wefel JS. In vitro enamel erosion associated with commercially available original-flavor and sour versions of candies. J Am Dent Assoc. 2009;140:906–913.
- Moynihan PJ. Update on nutrition and periodontal disease. Quintessence Int. 2008;39:326–330.
- Kaye EK. Nutrition, dietary guidelines and optimal periodontal health. Periodontol 2000. 2012;58:93–111.
- Maffeis C, Silvagni D, Bonadonna R, Grezzani A, Banzato C, Tato L. Fat cell size, insulin sensitivity, and inflammation in obese children. J Pediatr. 2007;151:647–652.
- Reeves AF, Rees JM, Schiff M, Hujoel P. Total body weight and waist circumference associated with chronic periodontitis among adolescents in the United States. Arch Pediatr Adolesc Med. 2006;160:894–899.
- Morita I, Okamoto Y, Yoshii S, et al. Fiveyear incidence of periodontal disease is related to body mass index. J Dent Res. 2011;90:199–202.
- Position of the Academy of Nutrition and Dietetics: Oral Health and Nutrition. J Acad Nutr Diet. 2013:113:693–701.
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2010. 7th ed. Washington, DC: U.S. Government Printing Office; 2010.
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans 2015–2020. Available at: health.gov/dietaryguidelines/ 2015/guidelines. Accessed July 8, 2016.
- U.S. Department of Agriculture. ChooseMyPlate. Available at: choosemyplate.gov. Accessed July 8, 2016.
- Corkins KG. Nutrition-focused physical examination in pediatric patients. Nutr Clin Pract. 2015;30:203–209.
- Radler DR, Mobley C. Obesity and oral health across the lifespan. In: Touger-Decker R, Mobley C, Epstein JB, eds. Nutrition and Oral Medicine. 2nd ed. New York: Humana Press; 2014.
- Marshall TA. Chairside diet assessment of caries risk. J Am Dent Assoc. 2009;140:670–674.
- Patrick H, Williams GC. Selfdetermination theory: its application to health behavior and complementarity with motivational interviewing. Int J Behav Nutr Phys Act. 2012;2;9–18.
From Decisions in Dentistry. August 2016;2(08):40–43.

