
Managing Subcutaneous Emphysema Following Dental Procedures
While uncommon, dental providers need to be able to diagnose and treat this potentially fatal complication.
While uncommon, dental providers need to be able to diagnose and treat this potentially fatal complication
PURCHASE COURSE
This course was published in the September 2017 issue and expires September 2020. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
Subcutaneous emphysemas result when air is forcefully introduced underneath soft tissues, which can lead to dissection of the fascial planes in the affected area. In medicine, this is often associated with blunt force trauma, such as motor vehicle accidents, abuse, infections with gas-forming bacteria, or iatrogenic causes, including laparoscopic procedures.1,2 In dentistry, subcutaneous emphysemas are uncommon, but typically result from restorative treatment, a head and neck infection with clostridium bacteria, or surgical procedures in which a high-speed air-driven handpiece is used and air, bacteria, oil or debris become embedded in the surrounding soft tissues.3 For patients having general anesthesia, endotracheal intubation carries a small and rare risk of a mucosal tear; mechanical ventilation or bag mask valve ventilation that follows can lead to the introduction of air in the pleural or mediastinal spaces, causing an airway obstruction.4
This course was published in the September 2017 issue and expires September 2020. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- List the types of dental procedures that can produce a subcutaneous emphysema.
- Identify clinical signs and risk factors that can lead to a diagnosis of a subcutaneous emphysema.
- Describe advanced imaging technologies that will aid diagnosis of this complication, and a typical time period for resolution without treatment.
According to a number of case reports in the literature, endodontic treatment, surgical extractions, restorative therapy, crown preparations and the use of air abrasion have caused subcutaneous emphysemas.5–10 Patients seem to be more at risk if there is preexisting periodontal disease.10 In addition to iatrogenic causes, subcutaneous emphysemas can also be patient-induced. This typically occurs after an extraction in situations in which the patient begins to smoke, cough, exhale forcefully or vomit before any healing has taken place.11 In the case of endodontic treatment, sodium hypochlorite accidents, the use of air-driven syringes, and misuse of rubber dams — or not using a rubber dam — have been documented as causing subcutaneous emphysemas.12–14
Dentists need to be aware of this rare, but potentially life-threatening, complication and able to differentiate subcutaneous emphysemas from more common disease processes that have similar clinical presentations.
DIFFERENTIAL DIAGNOSES
The first sign of subcutaneous emphysema is the swelling of the overlying soft tissues, which could take place immediately or several hours after the event has occurred. In cases in which the subcutaneous emphysema has spread to the paratracheal, mediastinal or thoracic spaces, there may be alterations in breathing. However, myriad conditions are associated with rapid swelling, including (but not limited to) soft tissue infections, angioedema, allergic reactions and hematomas.
There are signs and symptoms that can guide dental professionals to the correct diagnosis. Taking a thorough history, as well as a complete physical exam, are a good beginning. A subcutaneous emphysema typically does not have an associated erythema and warmness upon palpation, as seen with odontogenic or skin infections. Patients may complain of swelling and that the affected area feels like they have been eating fizzy candy (e.g., Pop Rocks). A complete blood count, as well as blood panels, will reveal normal C4 levels and white blood cell counts. This is in contrast to angioedema, where one would expect to see depressed levels of C4.15
However, there is a chance that besides the emphysema, bacteria could also be introduced during the traumatic event, leading to the patient presenting with a concomitant soft tissue infection. Thus, the patient may exhibit the cardinal signs of inflammation (e.g., erythema, redness, swelling or pain) and infection.
When arriving at a differential diagnosis, it is important for clinicians to take into account the patient’s entire medical history. Allergic reactions may also occur and can easily be avoided by reviewing the patient’s medical history. Likewise, it is possible that the patient could have an undocumented allergy. In both cases, an acute, localized swelling may occur and mimic a subcutaneous emphysema. The most efficient way to differentiate an allergic reaction from a subcutaneous emphysema is to note any responsiveness to antihistamines or steroids. The medical history can also be checked for any conditions that might cause the patient to be immunocompromised and, thus, prone to infections, such as individuals with uncontrolled diabetes or human immunodeficiency virus.
Ultimately, the pathognomonic sign of subcutaneous emphysema is crepitus upon palpation of the affected area. However, it has been noted this sign may take several hours to emerge.16
RADIOGRAPHIC PRESENTATION AND SEQUELAE
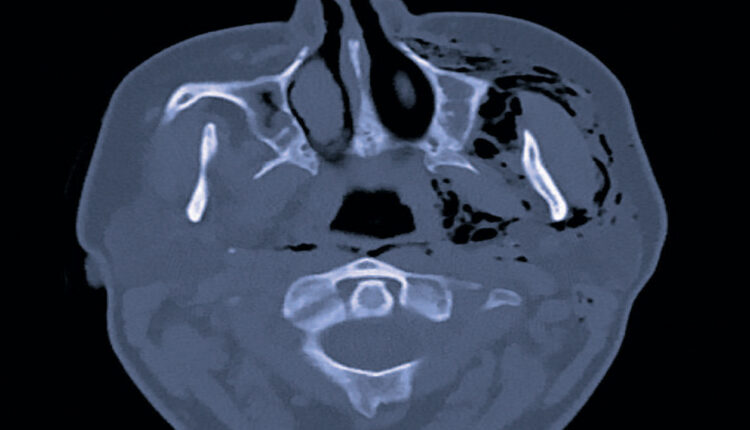
Unfortunately, little evidence of this complication can be seen on the imaging modalities commonly available to dental practitioners. Intraoral radiographs and panoramic radiography are likely to be inconclusive (as shown in Figure 1). Even cone beam computed tomography (CBCT) will yield inconclusive findings. Although pockets of air can be detected much easier when using CBCT rather than two-dimensional radiography, a number of conditions can produce this finding. Infections — such as clostridial myonecrosis, space abscesses or cellulitis — are capable of producing gas and will alter the surrounding soft tissues. Again, this is where a review of the medical history is important, as certain conditions, such as uncontrolled diabetes or acatalesemia, can make a patient prone to clostridial-type infections.17

remnants of teeth #2 and #3.
Due to the lack of soft tissue detail on a CBCT, a hospital referral for multidetector computed tomography (MDCT) of the head and neck should be made to determine the extent and location of the subcutaneous emphysema. Depending on the extent, patients should be monitored closely prior to discharge for any respiratory or cardiac distress. If left untreated, there have been instances secondary to dental treatment in which a subcutaneous emphysema spread to the mediastinum and thoracic regions, causing pneuomediastinum, pneumothorax and pleural effusion.18 In addition, if it spreads to the pericardial space, there have been reports of arrhythmias and electrocardiogram alterations.19 There have also been reports secondary to an extraction in which the emphysema spread to the orbital and periorbital regions, leading to blindness due to nerve compression.20 There are even rare instances in which air emboli from the soft tissues entered the bloodstream, causing seizures and ischemic brain lesions, leading to short-term memory impairment.21 Thus, it is critical that early recognition and proper management be implemented to prevent such progressions.
MANAGEMENT AND TREATMENT
If a subcutaneous emphysema is suspected, the initial clinical step is to immediately stop the procedure to determine its extent and location. This can be achieved by palpation of the skin over the affected area, which may indicate the spread and extent of entrapped air.
Fortunately, space emphysema is usually self-limited and resolves in three to 10 days, as the gas is resorbed into the bloodstream for eventual excretion via the lungs.22–25 Although imaging may not be recommended in the absence of severe clinical findings — and even if there are no signs of compromises in vision, airway, cardiac or brain function — the patient should be observed until the clinician is satisfied the path of the air has been tracked and is no longer advancing. At this point, the patient can be successfully managed on an outpatient basis with close follow-up.
The administration of prophylactic antibiotics for potential infections and/or corticosteroids to reduce swelling have been reported in the literature; however, there is no consensus on their use. The authors recommend careful consideration of such pharmaceuticals, taking the patient’s clinical signs and symptoms into account, including any bacterial infection or inflammation present before the administration of antibiotics.
PREVENTIVE STRATEGIES
Considering that use of high-speed air-driven handpieces is a chief cause of subcutaneous emphysema in dental settings, clinicians are advised to closely follow manufacturers’ recommendations as to proper use and maintenance, as this will help prevent complications. Additionally, patients should be advised about the consequences of not following postoperative instructions after an extraction. For example, coughing, smoking, nose blowing, using straws, vomiting or other activities that increase pressure in the oral cavity may increase the risk of a subcutaneous emphysema. When endotracheal intubation during general anesthesia is required, excessive inspiratory pressures and volumes should be avoided, and special care should be taken to minimize injury to the tracheal mucosa.
Clinical choices that further reduce the risk of subcutaneous emphysemas include utilizing high-speed electric handpieces, the proper use of rubber dams during restorative and endodontic procedures, and the judicious use of paper points during endodontic treatment.24–28 In addition, when sectioning a tooth or mucoperiosteal flap elevation is required during surgery, strategic decisions — such as sectioning the tooth before flap elevation, and elevating a smaller flap to avoid directly injecting air into it — may also reduce the risk.
Another step toward preventing subcutaneous emphysemas is to ensure the patient’s periodontal condition is optimal. With chronic inflammation, deep periodontal pockets form and the junctional epithelium starts to loosen from the gingival sulcus. This can easily create channels for air to spread to adjacent soft tissues when a high-speed air driven handpiece is used in the affected area. When the treatment plan allows, proper phasing and sequencing should be followed in order to ensure that periodontal conditions are managed before any restorative or definitive treatment is completed.
CASE STUDY
A 36-year-old female with a noncontributory medical history presented to the emergency department with a chief complaint of right facial swelling and pain two days after extraction of the right maxillary first and second molars at a local community clinic. The management of the patient included a one-week course of 500 mg penicillin VK as a prophylactic measure to prevent a bacterial infection, as well as an opioid for pain, as needed. Symptoms arose the morning after the extractions, and, at the time of her emergency department visit, were increasing in severity adjacent to the right ear and along the mandible. Upon clinical examination, pain was noted upon palpation and jaw movement, but the patient reported no symptoms of fever, chills, nausea or headaches. Subsequently, a panoramic radiograph, basic metabolic panel, and an MDCT with IV contrast were ordered to investigate further. The panoramic radiograph (Figure 1) and basic metabolic panel were inconclusive as to the source of the patient’s chief complaint.
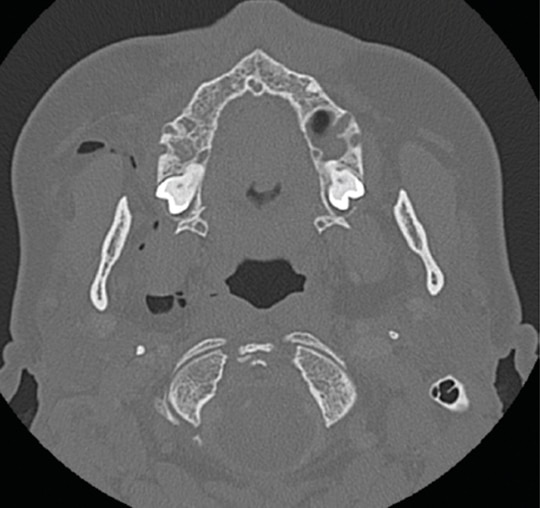
The MDCT revealed a collection of air pockets adjacent to the right masticator and parapharyngeal space (Figure 2), as well as fat stranding anterior to the masticator space (Figure 3). There were no obvious signs of fluid collection in the area that would have represented an abscess.

Although no documentation is readily available about the extraction techniques that could have resulted in a subcutaneous emphysema, the following assumptions seem plausible. There is radiographic evidence the extracted teeth were periodontally compromised, along with being grossly carious and/or fractured (Figure 1). These conditions may have prolonged the surgical procedure, creating a more vulnerable condition for the introduction of air into the adjacent soft tissues. In the extraction of retained root fragments, mucoperiosteal flaps are often utilized to improve access and visualization; this also could have made the tissue susceptible to a subcutaneous emphysema. The air could have been introduced to the subcutaneous tissue via an air-driven handpiece or air-water syringe. Air-driven handpieces are frequently used to facilitate the removal of retained roots and clean and smooth postextraction surface irregularities to improve healing. Similarly, air-water syringes are used by some dentists instead of gauze to clear away blood and debris during extractions.
SUMMARY
In conclusion, subcutaneous emphysemas secondary to dental procedures are rare, but can be a potentially life-threatening complication if not diagnosed and treated quickly and properly. Entrapped air can advance deeper in the soft tissue and cause a fatal air embolism and/or dangerous infections through dissemination of bacteria. In addition, patients can have minimal signs and symptoms, which potentially presents a diagnostic and management challenge. A diagnosis of a subcutaneous emphysema is best established radiographically, in conjunction with a comprehensive review of the patient’s medical history and clinical examination.
REFERENCES
- Cassada DC, Munyikwa MP, Moniz MP, Dieter RA Jr, Schuchmann GF, Enderson BL. Acute injuries of the trachea and major bronchi: importance of early diagnosis. Ann Thorac Surg. 2000;69:1563–1567.
- Bansal BC, Abramo TJ. Subcutaneous emphysema as an uncommon presentation of child abuse. Am J Emerg Med. 1997;15:573–575.
- McKenzie WS, Rosenberg M. Latrogenic subcutaneous emphysema of dental and surgical origin: a literature review. J Oral Maxillofac Surg. 2009;67:1265–1268.
- Balaji SM. Subcutaneous emphysema. J Maxillofac Oral Surg. 2015;14:515–517.
- Safar JA. Subcutaneous emphysema during removal of an overhang. Gen Dent. 1995;43:424.
- An GK, Zats B, Kunin M. Orbital, mediastinal, and cervicofacial subcutaneous emphysema after endodontic retreatment of a mandibular premolar: a case report. J Endod. 2014;40:880–883.
- Buchbender M, Musazada S, Kreißel S, Schmitt CM. Extensive cervicofacial and mediastinal subcutaneous emphysema after endodontic retreatment of a maxillary canine: a case report. J Oral Maxillofac Radiol. 2017;5:14–18.
- Haitz KA, Patel AJ, Baughman RD. Periorbital subcutaneous emphysema mistaken for unilateral angioedema during dental crown preparation. JAMA Dermatol. 2014;150:907–909.
- Toniollo MB, Terada AS, Yamaji MA. Subcutaneous emphysema after treatment using air-abrasive device: case report. Braz Dent Sci. 2016;19:106–110.
- Lee SW, Huh YH, Cha MS. Latrogenic subcutaneous cervicofacial emphysema with pneumomediastinum after class V restoration. J Korean Assoc Oral Maxillofac Surg. 2017;43:49–52.
- Ali A, Cunliffe DR, Watt–Smith SR. Surgical emphysema and pneumomediastinum complicating dental extraction. Br Dent J. 2000;188:589–590.
- de Sermeño RF, da Silva LA, Herrera H, Herrera H, Silva RA, Leonardo MR. Tissue damage after sodium hypochlorite extrusion during root canal treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:e46–e49.
- Kim Y, Kim MR, Kim SJ. Iatrogenic pneumomediastinum with extensive subcutaneous emphysema after endodontic treatment: report of 2 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109:e114–e119.
- Uehara M, Okumura T, Asahina I. Subcutaneous cervical emphysema induced by a dental air syringe: a case report. Int Dent J. 2007;57:286–288.
- Bas M, Hoffmann TK, Kojda G. Evaluation and management of angioedema of the head and neck. Curr Opin Otolaryngol Head Neck Surg. 2006;14:170–175.
- McGrannahan WW. Tissue space emphysema from an air turbine handpiece. J Am Dent Assoc. 1965;71:884–885.
- Góth L, Nagy T. Acatalasemia and diabetes mellitus. Arch Biochem Biophys. 2012;525:195–200.
- Gulati A, Baldwin A, Intosh IM, Krishnan A. Pneumomediastinum, bilateral pneumothorax, pleural effusion, and surgical emphysema after routine apicoectomy caused by vomiting. Br J Oral Maxillofac Surg. 2008;46:136–137.
- Reiche-Fischel O, Helfrick JF: Intraoperative life-threatening emphysema associated with endotracheal intubation and air insufflation devices: report of two cases. J Oral Maxillofac Surg 1995;53:1103–1107.
- Buckley MJ, Turvey TA, Schumann SP, Grimson BS. Orbital emphysema causing vision loss after a dental extraction. J Am Dent Assoc. 1990;120:421–422.
- Magni G, Imperiale C, Rosa G, Favaro R. Nonfatal cerebral air embolism after dental surgery. Anesth Analg 2008;106:249–251.
- Salib RJ, Valentine P, Akhtar S. Surgical emphysema following dental treatment. J Laryngol Otol. 1999;113:756–758.
- Schuman NJ, Edwards BC, Walker W, Chitwood W. Subcutaneous emphysema during operative dentistry: report of a case with 30 month follow-up. J Oral Med. 1983;38:168–169.
- Heyman SN, Babayof I. Emphysematous complications in dentistry, 1960–1993: an illustrative case and review of the literature. Quintessence Int. 1995;26:535–543.
- Yadav RK, Chandra A, Tikku AP, Wadhwani KK, Verma P. Air emphysema — an in office emergency: a case report. Endodontology. 2011;23:74–78.
- Uyanık LO, Aydın M, Buhara O, Ayalı A, Kalender A. Periorbital emphysema during dental treatment: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;112:e94–e96.
- Chan DC, Myers T, Sharaway M. A case for rubber dam application —subcutaneous emphysema after class V procedure. Oper Dent. 2007; 32:193–196.
- Fleischman D, Davis RM, Lee LB. Subcutaneous and periorbital emphysema following dental procedure. Ophthal Plast Reconstr Surg. 2014;30:e43–e45.
Featured Image by HELLERHOFF/WIKIMEDIA.ORG
From Decisions in Dentistry. September 2017;3(9):36,39–41.

