
Impact of Septa During Bone Augmentation in the Maxillary Sinus
An exploration of various treatment scenarios for managing septa during surgical procedures.
An exploration of various treatment scenarios for managing septa during surgical procedures
PURCHASE COURSE
This course was published in the May 2017 issue and expires May 2020. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Describe the morphology and orientation of maxillary sinus septa.
- Discuss the identification and classification of these structures in the sinus.
- Explain the prevalence, management and surgical treatment of septa.
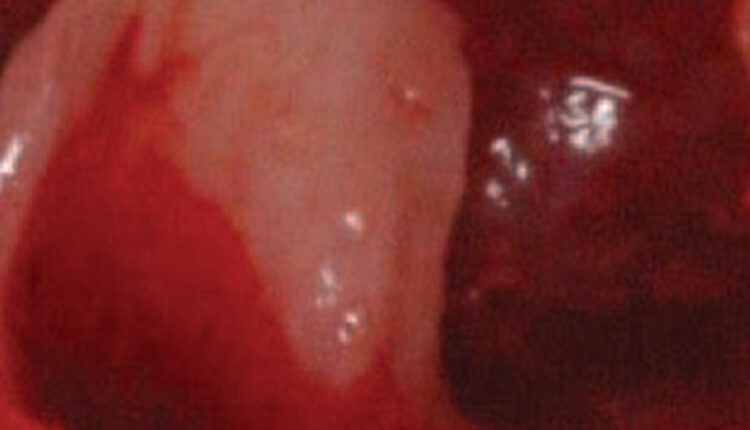
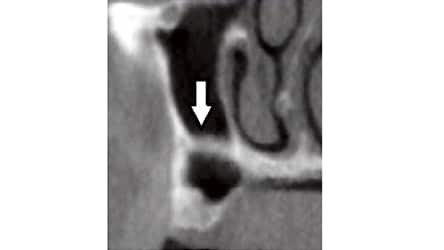
In the maxillary sinus, fin-like, sharp bony anatomical structures often protrude from sinus walls and are referred to as septa (Figure 1).1 The term septum means a dividing partition between two tissues or cavities2 The plural of septum is septa or septums. In the maxillary sinus, septa can be complete (e.g., extending from the sinus wall to an opposing wall) or incomplete (e.g., protruding from a bony wall, but not compartmentalizing the sinus cavity).3,4 Typically, they do not traverse the entire sinus cavity vertically or horizontally.3 Septa appear as white lines on periapical and panoramic films, and are more defined in cross-sectional, sagittal and axial views of a computed tomography (CT) or cone beam computed tomography (CBCT) scan.3,5–8 It is beneficial to be aware of septa prior to attempting a lateral wall sinus lift or transcrestal sinus floor elevation because these structures can complicate maxillary sinus bone augmentation procedures.
This article addresses a variety of issues related to the prevalence, morphology, orientation and management of maxillary sinus septa. In developing this paper, the literature was searched with PubMed using the following terms: maxillary sinus septa, maxillary septum, sinus floor elevation, sinus anatomy, sinus surgery, lateral wall sinus lift, and the bibliographies of article references were searched for pertinent studies.
BACKGROUND AND TERMINOLOGY
In 1910, the anatomist Arthur Underwood described septa in the maxillary sinus.9 Subsequently, these structures are often referred to as Underwood’s septa. The maxillary sinus is also called the antrum of Highmore.9 An antrum is a natural space or a cavity in bone10 and it was English physician Nathan Highmore who first described this maxillary structure in 1642.9
Two sinus procedures routinely used to augment bone in an atrophied posterior maxilla are a lateral window sinus lift and transcrestal sinus floor elevation. A sinus lift procedure was first reported in the literature by Boyne and James in 1980;11 however, Tatum developed this procedure in the 1970s. Subsequently, Summers12 described a transcrestal sinus floor elevation in which an osteotome is used to up-fracture the sinus floor to facilitate bone grafting into the sinus via an osteotomy. Both methods can be affected by septa; thus, it is helpful to note their presence when planning treatment.
When addressing the percentage of sinuses that have septa, it should be referred to as the prevalence, not the incidence, of septa. The term incidence refers to the number of findings per population in a given time period, whereas prevalence denotes the total number of disease cases or structures in a population.13 The term recess refers to an empty space or a cavity.14 Underwood9 denoted different regions in the maxillary sinus, including alveolar, zygomatic and infraorbital recesses. The alveolar recess points toward the alveolar bone; the zygomatic cavity is directed laterally and is bounded by the zygomatic arch; and the infraorbital recess aims superiorly to the inferior orbital surface of the maxilla. In addition, the alveolar region has compartments referred to as anterior, middle and posterior recesses. These correspond, respectively, to areas apical to the second premolar, first molar and second molar sites. Researchers often report the occurrence of sinus floor septa with respect to various alveolar recesses.4,7,15
ALVEOLAR VERSUS BASAL BONE
Basal bone is the osseous tissue of the mandible or maxilla except for the alveolar processes. Teeth are encased in alveolar bone, which rests upon basal bone — the native bone that is present before alveolar bone forms.16 Histologically, basal and alveolar bone cannot be differentiated. However, Park et al16 conducted a study of bone density and found that basal bone is denser than alveolar bone (835 to 1113 versus 810 to 940 Hounsfield units, respectively). Congenital septa consist of basal bone, whereas septa that form due to resorption of alveolar bone can consist of basal and/or alveolar bone.
IDENTIFYING SEPTA
Different criteria have been used to define the sizes of bony protuberances before they are characterized as septa: 2 mm,17 > 2 mm,18 > 2.5 mm,6,19–22 3 mm15,23 and 4 mm.24 These criteria were proposed to differentiate septa from bone irregularities that are caused by uneven bone resorption. When Pommer et al3 compared septa prevalence using the criteria < 2.5 mm versus > 2.5 mm, they reported no statistically significant difference in the prevalence of sinus septa (27.9% versus 27.1% of sinuses). In addition, it should be noted that an investigation might report a high prevalence of septa if more than a typical amount of septa are present in a small study population.25
Septa can be identified using various methodologies, such as an orthopantomograph (panoramic),5,6 three-dimensional (3D) CBCT,4,17,26 during surgery,27 and in cadaveric dissection.15,28,29 Studies have consistently demonstrated that 3D CBCT is more accurate than panoramic films in detecting septa. In general, panoramic films have a higher false positive and false negative finding than 3D CBCT scans.3,5–8
Septa also need to be differentiated from an antrolith, which are rare, calcified masses in the sinus that form around a foreign body.30 These masses may not be attached to a wall of the sinus; in addition, their shape is usually irregular and they have a homogeneous density. Antroliths may be solitary or multiple and require no therapy unless they are symptomatic.
FUNCTION AND FORMATION OF SEPTA
Neivert31 suggested the origin of septa is due to fingerlike projections produced by the embryological outpouching of the ethmoid infundibulum where the contiguous walls do not resorb. Septa function as force-carrying struts, according to van den Bergh et al.32 Septa are divided into two types, depending on their origin. Congenital or primary septa arise during development of the maxilla, whereas secondary or acquired septa develop after tooth loss and bone resorption8,33 or sinus pneumatization.8 Several authors indicated that more secondary septa are seen in edentate than dentate individuals.3,8,22,26 Sharan and Majdar34 observed that when a single posterior tooth is removed, patients may experience 0.54 mm of pneumatization (internal bone loss) within six months. Furthermore, if multiple teeth are extracted, a mean bone loss of 2.22 mm occurs due to sinus pneumatization. This uneven bone resorption can result in formation of secondary septa.8
While it is not possible to denote a septum as primary or secondary without a radiographic history, it can be deduced that septa situated apical to the dentate regions are primary (developmental), and those found apical to the edentulous maxilla are either primary or secondary.35
SEPTA SHAPE
Septa typically manifest several contour characteristics. They are usually thin, but can be wide.9 Their height is usually greater than their width, and septa are often found against the medial wall.3,7,8 Furthermore, they are often larger as they course latero-medially and manifest a shape similar to an inverted Gothic arch.7,8 Septa are usually composed of cortical bone,25 however, if there is a wide septum, cancellous bone may be present.9
ORIENTATION, PREVALENCE, LOCATION and size of septa
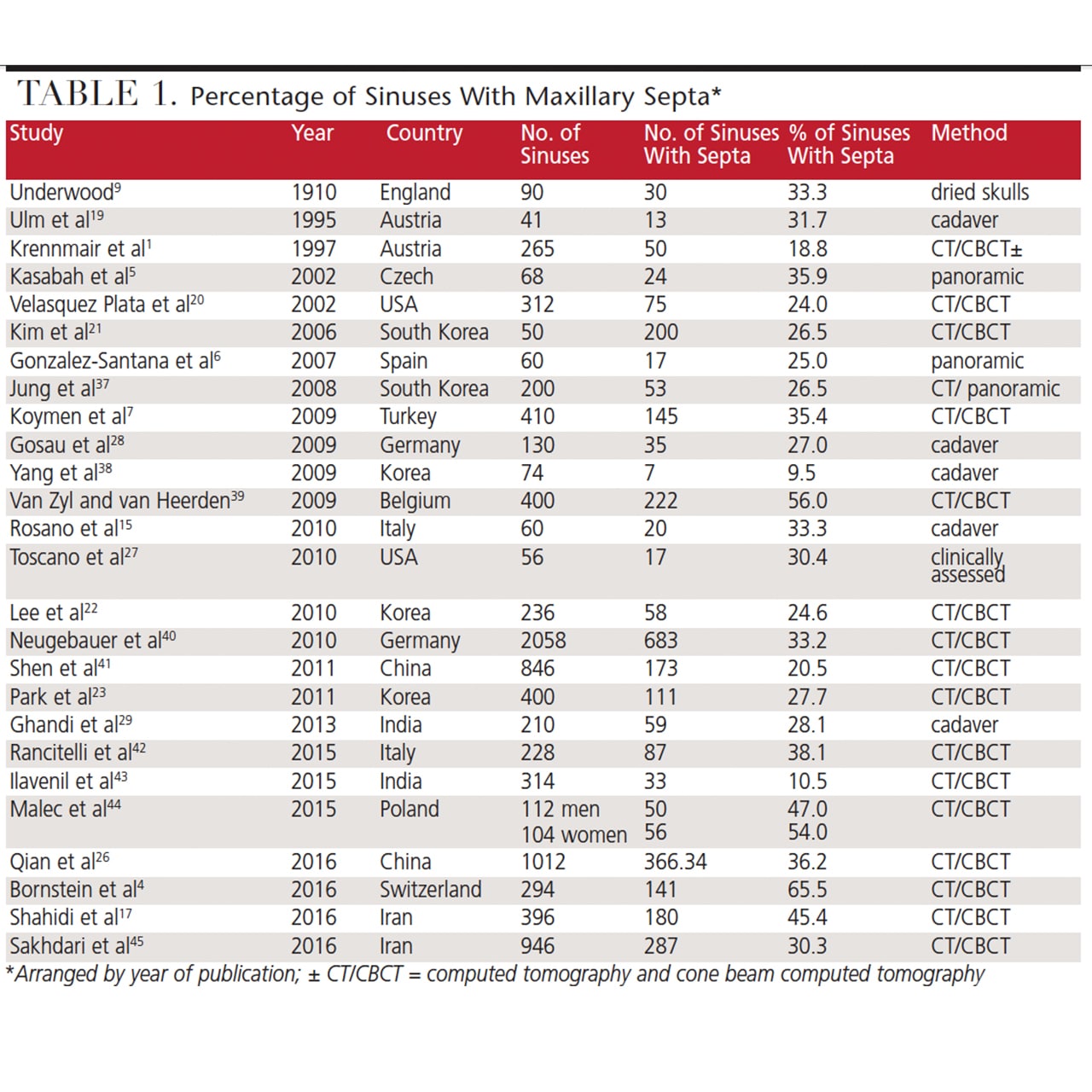
While the prevalence of septa in the maxillary sinus varies in different studies, it ranges from 9.5% to 65.5% (Table 1).1,4–7,9,15,17,19–23,26–29,37–45 Sometimes, data is reported as the percentage of patients who have septa, not the percentage of sinuses affected. In this regard, the percentage of patients manifesting septa may be higher than the percentage of sinuses with septa (because patients may not have septa in both sinuses). For example, Qian et al26 reported the percentage of patients versus the percentage of sinuses with septa was 48.2% and 32.6%, respectively.
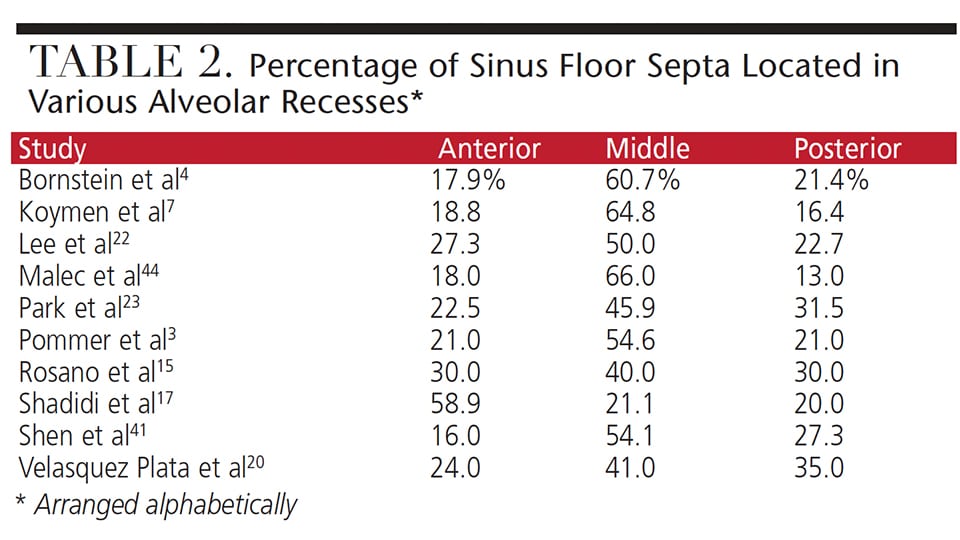
 In a systematic review, Pommer et al3 reported the following findings. Septa were present in 28.4% of sinuses (8923 sinuses assessed) and the range between studies was 9.5% to 55.5%. The 95% confidence limit ranged from 24.3% to 32.5%. One quarter of the patients manifested septa in one sinus and 17.2% had them bilaterally, therefore, 42.2% of patients had a septum. There were more septa in edentate than dentate maxillae due to formation of secondary septa.21,46 Pommer et al3 also noted the following distribution of septa with respect to orientation: buccopalatal 87.6%, mesiodistal 11.1%, and horizontal (parallel to the sinus floor) 1.3%. Complete septa dividing the sinus into compartments occurred in 0.3% of the sinuses, and multiple septa occurred in 4.2%. While septa can be found on the floor or walls of the sinus, they most often arise from the floor (58.6% of septa).4 Table 2 delineates the percentage of sinus floor septa found in the anterior, middle or posterior recesses, with most sinus floor septa arising in the middle recess.3,4,7,15,17,20,22,23,41,44
In a systematic review, Pommer et al3 reported the following findings. Septa were present in 28.4% of sinuses (8923 sinuses assessed) and the range between studies was 9.5% to 55.5%. The 95% confidence limit ranged from 24.3% to 32.5%. One quarter of the patients manifested septa in one sinus and 17.2% had them bilaterally, therefore, 42.2% of patients had a septum. There were more septa in edentate than dentate maxillae due to formation of secondary septa.21,46 Pommer et al3 also noted the following distribution of septa with respect to orientation: buccopalatal 87.6%, mesiodistal 11.1%, and horizontal (parallel to the sinus floor) 1.3%. Complete septa dividing the sinus into compartments occurred in 0.3% of the sinuses, and multiple septa occurred in 4.2%. While septa can be found on the floor or walls of the sinus, they most often arise from the floor (58.6% of septa).4 Table 2 delineates the percentage of sinus floor septa found in the anterior, middle or posterior recesses, with most sinus floor septa arising in the middle recess.3,4,7,15,17,20,22,23,41,44
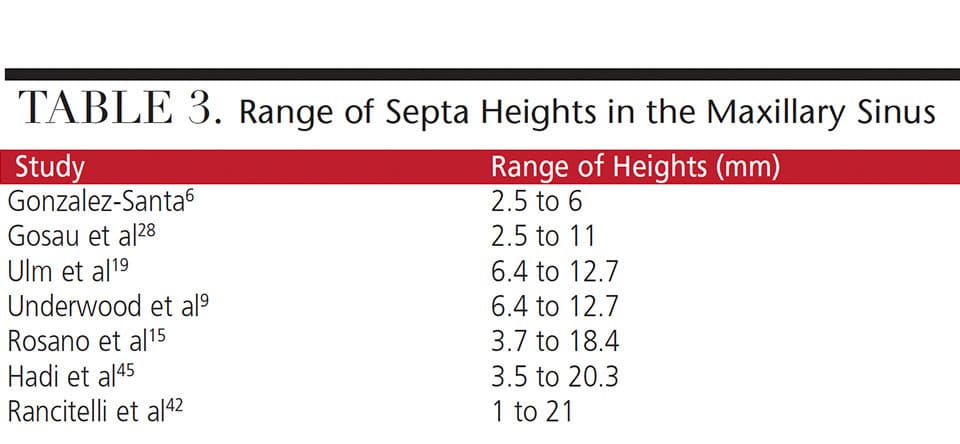
The systematic review by Pommer et al3 reported a mean septal height of 7.5 mm, but the range varies extensively in different studies (Table 3).6,9,15,19,28,42,45 Thus, a mean statistic provides limited information with regard to clinical management of septa.
SCHNEIDERIAN MEMBRANE thickness
Although the thickness of the Schneiderian membrane is normally approximately 1 mm, it varies in different regions of the sinus.47 Rancitelli et al42 found that the mean Schneiderian membrane thickness close to a septum was 1.8 mm, and far from it, the membrane was 0.85-mm thick. In contrast, Cakur et al48 reported a negative correlation between septa proximity and membrane thickness (r = -0.168). In other words, the membrane was thinnest in the vicinity of the septum. It was suggested that septa may be a causation for membrane thinness. These latter data underscore the concept that elevation of the Schneiderian membrane over septa should be performed with caution. However, there is too little data at this time to reach a definitive conclusion regarding the impact of septa on membrane thickness.
ISSUES ASSOCIATED WITH SEPTA
There are several potential problems associated with septa during lateral window sinus augmentation or transcrestal sinus floor elevation procedures. Besides increasing the likelihood of membrane perforation,49–51 the presence of septa can impede moving the lateral window medially32 or prevent the up-fracturing of the sinus floor.52 Furthermore, vertical or horizontal septa may divide the sinus into multiple compartments that require different treatment approaches.4,36,53,54 Therefore, clinicians must be prepared to modify the treatment method to accommodate and manage septa.
Schneiderian Membrane Tears: Anatomic variations in the sinus, such as septa, increase the risk of membrane perforation during elevation procedures.8,21,32,35,53 For example, Schwarz et al55 reported a perforation rate of 8.6% upon membrane elevation when septa were absent, and 45.5% when septa were present. Other researchers noted the Schneiderian membrane tear rate is inversely related to its thickness,56 with perforations occurring more often when the membrane is < 1 mm57 or < 1.5mm56 thick. With respect to membrane elevation over partial septa, the Schneiderian membrane should be released latero-medially, because its elevation antero-posteriorly over a sharp ledge leaves it prone to perforation.58
Lateral Window Sinus Augmentation Modifications Due to Maxillary Septa: Wen et al54 classified septa management into easy, moderate or difficult categories, based on the location, number, orientation and size of septa.
Easy septa are located anterior to the zygomatic arch and course mediolaterally. When a septum is ≤ 6 mm in height, Wen et al54 suggested removal of the lateral bony window to complete a lateral sinus lift. However, if a septum is > 6 mm, their recommendation was to create two buccal windows — one on each side of the septum.
Moderate septa are found posterior to the zygomatic arch and oriented mediolaterally. If a septum is ≤ 6 mm, Wen et al54 advised removing the bony window to facilitate performing a sinus lift. But if a septum is > 6 mm, they suggested removing the bony window and septum through a single window.
Difficult septa include situations in which they occur anterior or posterior to the zygomatic process; in this case, treatment scenarios are subclassified as A, B and C, based on orientation and number of septa. For these subclassifications, Wen et al54 recommended the following treatments:
- Subclass A: If there is one anterior-posterior septum measuring ≤ 6 mm, use a single window and a lateral approach
- Subclass B: In the presence of one anterior-posterior septum that is > 6 mm, use a single window with a crestal approach and remove the bony window
- Subclass C: If there are two or more mediolateral septa, use multiple windows, combined with removing the bony window
With respect to septa removal, Boyne and James11 had another point of view. They recommended that septa be routinely removed with a chisel and mallet so a bone graft can be placed over the entire floor without interruption. However, the authors of this article do not think this is routinely necessary, unless the septa impede visualization of the sinus or inhibit membrane elevation.
When a lateral window sinus lift is performed, the osteotomy is often created so it facilitates horizontal rotation of a trap door (buccal plate) into the sinus cavity; subsequently, this island of bone becomes part of the roof of a sinus lift. However, a small septum situated medial to the trap door could impede rotation of the lateral bony window into the sinus. Thus, when there is a small septum on the sinus floor (seen on a CBCT scan), clinicians are advised to create a W-shaped lateral window (with the center of the window more apical) so it will pass over the septum when the trap door is rotated32 — alternately, it may be easier to remove the entire lateral bony window.
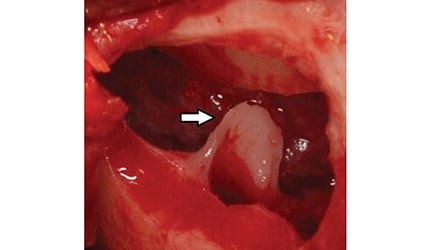
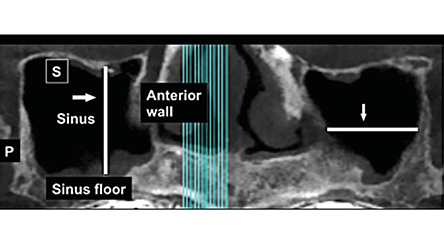
If a vertical septum (lateral view) divides the sinuses into anterior and posterior compartments (Figure 2 and Figure 3), clinicians can manage this in two ways: Separate windows can be created (one on each side of the septum),53,54,59,60 or one large window can be developed and the entire bony window over the two sections removed. In this case, each side of the septum (i.e., the anterior and posterior compartments) is treated independently. The need to do the posterior compartment is dictated by the amount of bone (mesio-distally) required to accommodate future implants.
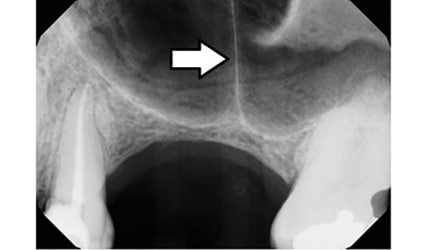
An uncommon finding is a horizontal septum that compartmentalizes the sinus into superior and inferior cavities (Figure 2 and Figure 4).36 In this case, clinicians must determine how much bone is needed to accommodate implants. It may only be necessary to treat the inferior cavity adjacent to the alveolar ridge to encompass the length of the planned implants. Otherwise, dual compartments must be managed with either two separate windows or one large window with the buccal bony plate removed.
Another septal variation that is rarely encountered is a vertical septum that divides the sinus into lateral and medial compartments (Figure 5).4 In this scenario, the location of the sections (with respect to the ridge) needs to be assessed. If the lateral compartment is under the ridge, only that section needs to be managed with a sinus lift. However, if both compartments require treatment, clinicians must gain access to the lateral section to elevate the membrane, and proceed through the vertical septum to treat the medial compartment.
Mailleux et al61 reported a rare occurrence of the inferior orbital nerve within a horizontal septum in the superior aspect of the maxillary sinus. They cautioned that disruption of these septa could result in paresthesia of the maxillary region and noted these unusual anatomic findings need to be detected during a preoperative CT work-up.
Transcrestal Sinus Lift Modification Due to Septa: Prior to performing a transcrestal sinus floor elevation, it is prudent to verify that a septum is not superior to a site where the sinus floor will be up-fractured.52 When a septum is present, it will impede elevating the sinus floor; moreover, if significant force is used during up-fracturing, it is possible to splinter the maxillary bone in an uncontrolled manner. Thus, if a septum is present over a site to be up-fractured, clinicians should choose a different location or perform a lateral wall sinus lift.
IMPLANT PLACEMENT INTO A SEPTUM
Placing an implant into a maxillary septum is conceptually possible (Figure 6). Although this idea was initially addressed by Fortin et al,62 Dragan et al63 subsequently suggested that if a septum was thick enough, an implant could be inserted into it. However, this is usually impractical because septa are infrequently wide enough to encase an implant. Furthermore, the study by Dragan et al63 was not performed on live patients; rather, it was a simulation investigation using 3D reconstructions.

CONCLUSION
Septa in the maxillary sinus are a common finding and their presence may require modification of a sinus augmentation procedure. With respect to identifying septa, the data indicate that CT or CBCT scans provide less false positive and false negative findings than panoramic imaging.3,5–8 Thus, prior to performing a sinus bone grafting procedure, it is strongly recommended that a CBCT scan be obtained to facilitate and enhance treatment planning.
REFERENCES
- Krennmair G, Ulm C, Lugmayr H. Maxillary sinus septa: incidence, morphology and clinical implications. J Craniomaxillofac Surg. 1997;25:261–265.
- Antum [Def. 1]. Dorland’s Medicial Dictionary. Accessed August 4, 2016 from dorlands.com/wsearch.jsp.
- Pommer B, Ulm C, Lorenzoni M, Palmer R, Watzek G, Zechner W. Prevalence, location and morphology of maxillary sinus septa: systematic review and meta-analysis. J Clin Periodontol. 2012;39:769–773.
- Bornstein MM, Seiffert C, Maestre-Ferrín L, et al. An analysis of frequency, morphology, and locations of maxillary sinus septa using cone beam computed tomography. Int J Oral Maxillofac Implants. 2016;31:280–287.
- Kasabah S, Slezák R, Simu°nek A, Krug J, Lecaro MC. Evaluation of the accuracy of panoramic radiograph in the definition of maxillary sinus septa. Acta Medica (Hradec Kralove). 2002;45:173–175.
- González-Santana H, Peñarrocha-Diago M, Guarinos-Carbó J, Sorní-Bröker M. A study of the septa in the maxillary sinuses and the subantral alveolar process in 30 patients. J Oral Implantol. 2007;33:340–343.
- Koymen R, Gocmen-Mas N, Karacayli U, Ortakoglu K, Ozen T, Yazici AC. Anatomic evaluation of maxillary sinus septa: surgery and radiology. Clin Anat. 2009;22:563–570.
- Krennmair G, Ulm CW, Lugmayr H, Solar P. The incidence, location, and height of maxillary sinus septa in the edentulous and dentate maxilla. J Oral Maxillofac Surg. 1999;57:667–671.
- Underwood AS. An inquiry into the anatomy and pathology of the maxillary sinus. J Anat Physiol. 1910;44:354–369.
- Septum. Dorland’s Medicial Dictionary. Accessed August 4, 2016 from dorlands.com/wsearch.jsp
- Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and bone. J Oral Surg. 1980;38:613–616.
- Summers RB. A new concept in maxillary implant surgery: the osteotome technique. Compendium. 1994;15:152,154–158.
- Greenstein G, Lamster I. Understanding diagnostic testing for periodontal diseases. J Periodontol. 1995;66:659–666.
- Recess [Def. 3]. Dorland’s Medicial Dictionary. Accessed August 4, 2016 from dorlands.com/wsearch.jsp.
- Rosano G, Gaudy JF, Chaumanet G, Del Fabbro M, Taschieri S. Maxillary sinus septa. Prevalence and anatomy. Rev Stomatol Chir Maxillofac. 2012;113:32–35.
- Park HS, Lee YJ, Jeong SH, Kwon TG. Density of the alveolar and basal bones of the maxilla and the mandible. Am J Orthod Dentofacial Orthop. 2008;133:30–37.
- Shahidi S, Zamiri B, Momeni Danaei S, Hamedani S. Evaluation of anatomic variations in maxillary sinus with the aid of cone beam computed tomography (CBCT) in a population in south of Iran. J Dent (Shiraz). 2016;17:7–15.
- Naitoh M, Suenaga Y, Kondo S, Gotoh K, Ariji E. Assessment of maxillary sinus septa using cone-beam computed tomography: etiological consideration. Clin Implant Dent Relat Res. 2009;11 (Suppl 1):e52–e58.
- Ulm CW, Solar P, Krennmair G, Matejka M, Watzek G. Incidence and suggested surgical management of septa in sinus-lift procedures. Int J Oral Maxillofac Implants. 1995;10:462–465.
- Velasquez-Plata D, Hovey LR, Peach CC, Adler ME. Maxillary sinus septa: a 3–dimensional computerized tomograhic scan analysis. J Periodontol. 2002;17:854–860.
- Kim MJ, Jung UW, Kim CS, et al. Maxillary sinus septa: prevalence, height, location and morphology. A reformatted computed scan analysis. J Periodontol. 2006;77:903–908.
- Lee WJ, Lee SJ, Kim HS. Analysis of location and prevalence of maxillary sinus septa. J Periodontal Implant Sci. 2010;40:56–60.
- Park YB, Jeon HS, Shim JS, Kee KW, Moon HS. Analysis of the anatomy of the maxillary sinus septum using 3-dimensional computed tomography. J Oral Maxillofac Surg. 2011;69:1070–1078.
- Ella B, Noble Rda C, Lauverjat Y, et al. Septa within the sinus: effect on elevation of the sinus floor. Br J Oral Maxillofac Surg. 2008;46:464–467.
- Maestre-Ferrín L, Galán-Gil S, Rubio-Serrano M, Peñarrocha-Diago M, Peñarrocha-Oltra D. Maxillary sinus septa: a systematic review. Med Oral Patol Oral Cir Bucal. 2010;15:e383–e386.
- Qian L, Tian XM, Zeng L, Gong Y, Wei B. Analysis of the morphology of maxillary sinus septa on reconstructed cone-beam computed tomography images. J Oral Maxillofac Surg. 2016;74:729–737.
- Toscano NJ, Holtzclaw D, Rosen PS. The effect of piezoelectric use on open sinus lift perforation: a retrospective evaluation of 56 consecutively treatedcases from private practices. J Periodontol. 2010;81:167–171.
- Gosau M, Rink D, Driemel O, Draenert FG. Maxillary sinus anatomy: a cadaveric study with clinical implications. Anat Rec (Hoboken). 2009;292:352–354.
- Gandhi KR, Wabale RN, Siddiqui AU, Farooqui MS. The incidence and morphology of maxillary sinus septa in dentate and edentulous maxillae: a cadaveric study with a brief review of the literature. J Korean Assoc Oral Maxillofac Surg. 2015;41:30–36.
- Blaschke DD, Brady FA. The maxillary antrolith. Oral Surg Oral Med Oral Pathol. 1979;48:187–189.
- Neivert H. Surgical anatomy of the maxillary sinus. Laryngoscope. 1930;40:1–4.
- van den Bergh JP, ten Bruggenkate CM, Disch FJ, Tuinzing DB. Anatomical aspects of sinus floor elevations. Clin Oral Implants Res. 2000;11:256–265.
- Vinter I, Krmpotić-Nemanić J, Hat J, Jalsovec D. Does the alveolar process of the maxilla always disappear after loss of teeth? Laryngorhinootologie. 1993;72:605–607.
- Sharan A, Madjar D. Maxillary sinus pneumatization following extractions: a radiographic study. Int J Oral Maxillofac Implants. 2008;23:48–56.
- Chanavaz M. Maxillary sinus: anatomy, physiology, surgery, and bone grafting related to implantology — eleven years of surgical experience (1979–1990). J Oral Implantol. 1990;16:199–209.
- Güls¸en U, Mehdiyev I˙, Üngör C, S¸entürk MF, Ulas¸an AD. Horizontal maxillary sinus septa: An uncommon entity. Int J Surg Case Rep. 2015;12:67–70.
- Jung JW, Song KH, Lee SK, et al. The clinical study of maxillary sinus septa used in panorama, CT. J Korean Oral Maxillofac Surg. 2008;34:319–324.
- Yang HM, Bae HE, Won SY, et al. The buccofacial wall of maxillary sinus: an anatomical consideration for sinus augmentation. Clin Implant Dent Relat Res. 2009;11 (Suppl 1):e2–e6.
- van Zyl AW, van Heerden WF. A retrospective analysis of maxillary sinus septa on reformatted computerised tomography scans. Clin Oral Implants Res. 2009;20:1398–1401.
- Neugebauer J, Ritter L, Mischkowski RA, et al. Evaluation of maxillary sinus anatomy by cone-beam CT prior to sinus floor elevation. Int J Oral Maxillofac Implants. 2010;25:258–265.
- Shen EC, Fu E, Chiu TJ, Chang V, Chiang CY, Tu HP. Prevalence and location of maxillary sinus septa in the Taiwanese population and relationship to the absence of molars. Clin Oral Implants Res. 2012;23:741–745.
- Rancitelli D, Borgonovo AE, Cicciù M, et al. Maxillary sinus septa and anatomic correlation with the Schneiderian membrane. J Craniofac Surg. 2015;26:1394–1398.
- Ilavenil K, Guru AT, Gugapriya TS, Nalinakumari, SD. Maxillary sinus septation: A radiological study. Int J Sci Stud. 2015;3:101–104.
- Malec M, Smektala T, Tutak M, Trybek G, Sporniak–Tutak K. Maxillary sinus septa prevalence and morphology — computed tomography based analysis. Int J Morphol. 2015;33:144–148.
- Sakhdari S, Panjnoush M, Eyvazlou A, Niktash A. Determination of the prevalence, height, and location of the maxillary sinus septa using cone beam computed tomography. Implant Dent. 2016;25:335–340.
- Hadi FA, Najm A, Kadhum MA. Evaluation of maxillary sinus septal type and height in partially edentulous maxilla using spiral computed tomography. J Bagh Coll Dentistry. 2014;26:116–119.
- Janner SF, Caversaccio MD, Dubach P, Sendi P, Buser D, Bornstein MM. Characteristics and dimensions of the Schneiderian membrane: a radiographic analysis using cone beam computed tomography in patients referred for dental implant surgery in the posterior maxilla. Clin Oral Implants Res. 2011;22:1446–1453.
- Cakur B, Sümbüllü MA, Durna D. Relationship among Schneiderian membrane, Underwood’s septa, and the maxillary sinus inferior border. Clin Implant Dent Relat Res. 2013;15:83–87.
- Ardekian L, Oved-Peleg E, Mactei EE, Peled M. The clinical significance of sinus membrane perforation during augmentation of the maxillary sinus. J Oral Maxillofac Surg. 2006;64:277–282.
- Becker ST, Terheyden H, Steinriede A, Behrens E, Springer I, Wiltfang J. Prospective observation of 41 perforations of the Schneiderian membrane during sinus floor elevation. Clin Oral Implants Res. 2008;19:1285–1289.
- Hernández-Alfaro F, Torradeflot MM, Marti C. Prevalence and management of Schneiderian membrane perforations during sinus-lift procedures. Clin Oral Implants Res. 2008;19:19–98.
- Greenstein G, Cavallaro J. Transcrestal sinus floor elevation with osteotomes: simplified technique and management of various scenarios. Compend Contin Educ Dent. 2011;32:12–20.
- Betts NJ, Miloro M. Modification of the sinus lift procedure for septa in the maxillary antrum. J Oral Maxillofac Surg. 1994;52:332–333.
- Wen SC, Chan HL, Wang HL. Classification and management of antral septa for maxillary sinus augmentation. Int J Periodontics Restorative Dent. 2013;33:509–517.
- Schwarz L, Schiebel V, Hof M, Ulm C, Watzek G, Pommer B. Risk factors of membrane perforation and postoperative complications in sinus floor elevation surgery: Review of 407 augmentation procedures. J Oral Maxillofac Surg. 2015;73:1275–1282.
- Cho SC, Yoo SK, Moon DH, Elian N, Froum S, Tarnow D. Schneiderian membrane thickness and membrane perforation. AO Poster Presentation 2002.
- Yilmaz HG, Tözüm TF. Are gingival phenotype, residual ridge height, and membrane thickness critical for the perforation of maxillary sinus? J Periodontol. 2012;83:420–425.
- Cavallaro JS Jr, Greenstein G, Tarnow DP. Clinical pearls for surgical implant dentistry: Part 3. Dent Today. 2010;29:134–139.
- Smiler DG. The sinus lift graft: basic technique and variations. Pract Periodontics Aesthet Dent. 1997;9:885–893.
- Beretta M, Cicciù M, Bramanti E, Maiorana C. Schneider membrane elevation in presence of sinus septa: anatomic features and surgical management. Int J Dent. 2012;261905.
- Mailleux P, Desgain O, Ingabire MI. Ectopic infraorbital nerve in a maxillary sinus septum: another potentially dangerous variant for sinus surgery. JBR-BTR. 2010;93:308–309.
- Fortin T, Isidori M, Bouchet H. Placement of posterior maxillary implants in partially edentulous patients with severe bone deficiency using CAD/CAM guidance to avoid sinus grafting: a clinical report of procedure. Int J Oral Maxillofac Implants. 2009;24:96–102.
- Dragan E, Guillaume OA, Haba D, Olszewski R. Three-dimensional evaluation of implant positioning in the maxillary sinus septum: A retrospective study. Med Sci Monit. 2015;8:2666–2671.
From Decisions in Dentistry. May 2017;3(5):46—51.

