

Impact of Occlusal Discrepancies on Periodontal Disease
An examination of data that support an association between certain types of occlusal contacts and progression of pocket probing depths.
An examination of data that support an association between certain types of occlusal contacts and progression of pocket probing depths
PURCHASE COURSE
This course was published in the December 2016 issue and expires December 2019.The author has no commercial conflicts of interest to disclose.This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the controversial history of the relationship between occlusal contacts and their influence on periodontal disease progression.
- Identify which occlusal contacts contribute to the progression of periodontal disease.
- Explain the potential problems and benefits associated with the treatment of occlusal discrepancies as part of periodontal therapy.
The role that occlusion plays in the progression of periodontal disease has long been controversial. Early clinical observations indicated that teeth with heavy occlusal loads seemed to have deeper pockets than teeth with normal occlusal loads.1 In the early 20th century, Stillman2 postulated that abnormal occlusal contacts were responsible for periodontal disease, and that successful periodontal treatment was centered on occlusal adjustment.
In the mid-20th century, many studies of cadaver material attempted to demonstrate, one way or the other, whether occlusion played a role in the progression of periodontal disease. Glickman and Smulow3 believed that heavy occlusal contacts (occlusal trauma) in the presence of gingival inflammation were a codestructive force that resulted in deep pockets and bone loss. In comparison, Waerhaug4 argued that all periodontal destruction was associated solely with the advancing subgingival plaque front. Extensive animal studies also tried to correlate various forms of occlusal trauma to periodontal disease progression.5,6 The anatomical differences between animals and humans, however — and the types of trauma that were applied to the animals — make it difficult to correlate the results of these animal studies to human periodontal disease progression.
The 1996 World Workshop in Periodontics summed up the occlusion research of the 20th century by concluding there was no proof occlusion played a role in the progression of periodontal disease. It also noted that with the exception of the treatment of mobility and presence of parafunctional habits, there was no proof that occlusal treatment was beneficial in the control or treatment of periodontal disease.7 In addition, the workshop recognized that developing an ethical research protocol to determine a definitive answer to the role of occlusion in human periodontal disease progression was impossible. A controlled clinical trial would involve diagnosing periodontal disease and occlusal discrepancies, and withholding treatment from a portion of the study population.
OCCLUSAL INTERFERENCE
Given the unequivocal statement of the World Workshop in Periodontics that a controlled clinical trial evaluating the role of occlusion in periodontal disease progression in humans was unethical, an effort was made to retrospectively determine the effect of occlusion on the progression and treatment of periodontal conditions. Patient records from a private practice were evaluated to determine if occlusal discrepancies were a risk factor for the progression of periodontal disease.8,9 These studies were based on assessments of patients who had received periodontal evaluations, including thorough occlusal assessments. Patients then chose whether they wanted to receive complete periodontal treatment, or only undergo a portion of the recommended therapy. The patients voluntarily returned in 12 months for another periodontal and occlusal examination.

Some patients diagnosed with periodontal disease decided not to complete recommended periodontal treatment. When they returned 12 months later, the progression of periodontal involvement in teeth with occlusal discrepancies was compared with the progression in teeth that did not have occlusal discrepancies. This allowed for the ethical evaluation of the effects of occlusal discrepancies on untreated periodontal disease. In addition, in cases in which patients had some treatment before dropping out of active therapy, the effect of occlusal adjustment on teeth with discrepancies could be evaluated.
Among patients who had no periodontal treatment for 12 months or longer, pocket probing depths continued deepening over time for teeth with or without occlusal discrepancies (Figure 1). This is expected, as it is well established that untreated periodontal disease worsens over time. The rate of increase in pocket probing depths for teeth with occlusal discrepancies, however, was significantly higher than the increase in pocket probing depths of teeth without occlusal discrepancies. This portion of the study offers clear evidence that presence of an occlusal discrepancy resulted in a more rapid increase in pocket probing depth, and that presence of an occlusal discrepancy negatively influenced periodontal health.8,9
In cases in which a portion of the recommended periodontal treatment was performed, patients underwent subgingival root planing with local anesthesia, but did not follow through with surgical recommendations. Some patients had also undergone occlusal adjustment. Others dropped out of treatment before occlusal adjustments were performed. In this partially treated group, all teeth continued to exhibit increasing pocket probing depths (Figure 2), indicating that root planing was inadequate to halt the progression of periodontal disease in this cohort.10 While the rate of disease progression was slowed in all groups receiving treatment (compared to the untreated group), the teeth with untreated occlusal discrepancies experienced a more rapid increase in pocket probing depths compared with teeth without an occlusal discrepancy, or teeth in which discrepancies had been eliminated by occlusal adjustment. The fact that occlusal adjustment significantly slowed the increase in pocket probing depths indicated that removal of an occlusal discrepancy yielded a treatment benefit.

A later study evaluated the effect of occlusal discrepancies on the progression of gingival recession.11 While it is a commonly held belief that heavy occlusal contacts result in the loss of gingiva and exposure of the root surface, no correlation between occlusal discrepancies and recession was detected. While some gingival recession was noted at the initial examination, the study showed no correlation between existing gingival recession and the tooth’s occlusal contact. Additionally, increased recession (noted over time) was not related to an occlusal discrepancy. The study concluded that occlusal discrepancies do not contribute to gingival recession.11
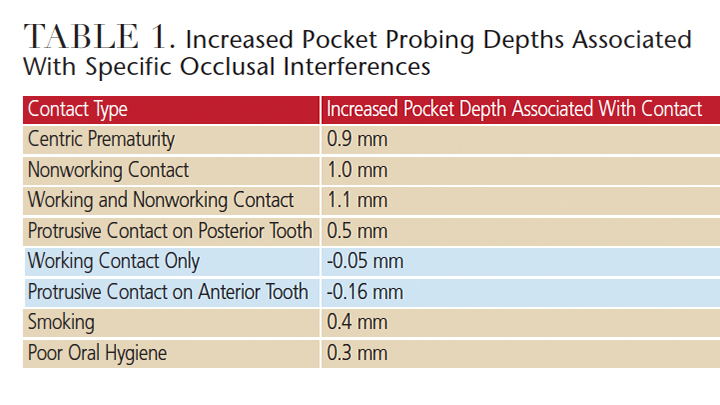
Four studies compared teeth that either had, or did not have, occlusal discrepancies. In these studies, an occlusal discrepancy was defined as a centric prematurity and/or a nonworking interference. This relatively broad definition was used due to the capabilities of the statistical programs available at the time of publication. Due to improvements in statistical programs, it was decided to reevaluate the data that looked at individual occlusal contacts.12 In this study, the effects of premature contacts in centric relation, working contacts, nonworking contacts, combined working and nonworking contacts, and protrusive contacts were evaluated individually (Table 1). Deeper pocket probing depths were noted on teeth that had a centric prematurity, a nonworking contact, a combined working and nonworking contact, or a protrusive contact on a posterior tooth. A working contact without a balancing contact and a protrusive contact on an anterior tooth were not associated with deep pocket probing depths. The pocket probing depths on teeth with a centric prematurity or nonworking contact experienced a mean increase in probing depths of 1 mm or greater compared with a similar tooth that lacked these contacts. The pocket probing depths associated with the damaging contacts were compared to known risk factors for periodontal disease: smoking and poor oral hygiene. In all cases, the mean pocket probing depths associated with the damaging occlusal contacts were statistically deeper than those associated with the known risk factors.
The outcomes of these studies suggest that occlusal discrepancies are a significant risk factor for the progression of periodontal disease. In addition, the studies on the partially treated group indicate that treatment of occlusal discrepancies is associated with slowing the progression of periodontal disease. Although these results are not definitive because the studies were not prospective, controlled clinical trials (which would have been unethical to perform), they provide the best data available to date. The results indicate that occlusal relationships should be evaluated in all patients with periodontal disease, and that occlusal therapy should be an integral portion of definitive periodontal therapy.
CLINICAL IMPLICATIONS
The research referenced in the previous section was based on a study of patients with established periodontal disease. Thus, the trends and results can only be applied to patients with periodontal involvement. These studies do not necessarily demonstrate the need to adjust occlusal discrepancies among patients with mild or no periodontal disease. If a patient’s periodontal condition does not respond to nonsurgical periodontal therapy, however, occlusal therapy and surgery should be considered.
The most definitive form of occlusal therapy is to permanently change the relationship between the teeth in a manner that eliminates the damaging occlusal contact. This may be accomplished through orthodontic therapy or multiple full-coverage restorations. In patients with advanced periodontal disease, however, these therapies are usually contraindicated because the long-term prognosis of the teeth cannot be established until periodontal disease is controlled. During active periodontal therapy, removable devices, such as a biteguard/occlusal stint, can help manage occlusal forces. Clinicians may also elect to perform definitive occlusal adjustment by reshaping the contours of the natural teeth. There are concerns with both approaches, however.
The use of a bite appliance is the least invasive approach to prevent potential damage from occlusal forces — and, because no permanent changes are made to the dentition, it is completely reversible. If there is a problem with patient acceptance, the appliance can be removed and the patient’s occlusal pattern remains the same as pretreatment. The issues surrounding a removable appliance are that most patients will not wear the appliance during the day, and compliance while sleeping varies. If a patient only wears the appliance during sleep, the teeth will undergo potentially damaging loading at least 50% of the time. If a patient bruxes during sleep, a large portion of the damaging loading may be occurring during sleep. In this case, the harm from the occlusal pressures caused by parafunctional habits may be avoided by use of a night guard.
A definitive occlusal adjustment of all teeth is the most predictable approach to relieving damage from occlusal contacts. It permanently removes the occlusal discrepancy and takes pressure off the tooth. In addition, this benefit is not dependent on patient compliance. That said, performing extensive tooth reshaping necessary to effectively eliminate damaging contacts from all teeth is a technically difficult procedure that should be approached with caution. While offering high potential benefit, if the procedure is not performed correctly there is potential for serious harm to the teeth and periodontium. Additionally, permanent reshaping of the occlusal surface cannot be reversed without extensive prosthetic intervention. Permanent occlusal adjustment should be approached cautiously, and specific training in the adjustment technique is necessary. If the treating dentist is not comfortable with performing a complete occlusal adjustment, the patient should be referred to a specialist.
EVALUATE AND DOCUMENT
Due to the evidence suggesting a possible association between occlusal discrepancies and the progression of periodontal disease, it is advisable for clinical teams to evaluate and record evidence of occlusal stress in patients with periodontal disease. Signs of occlusal stress include parafunctional habits, such as grinding/clenching, which may occur as a result of skeletal or positional misalignment of the dentition. A prominent clinical feature of parafunctional habits is the presence of flat spots or wear facets on the teeth. Obvious wear facets with a shiny surface usually indicate the patient is presently bruxing, while those with a dull surface suggest the patient has been a bruxer in the past, but is not currently — or perhaps bruxes intermittently. In either case, the findings should be recorded and the possibility of clenching/grinding discussed with the patient. Many individuals who routinely clench their teeth are not aware of the habit, and the first step in educating these patients is to show them the wear patterns on their teeth.
If patients are unsure or deny they are bruxers, they should be presented with information that will help them self-diagnose possible parafunctional habits. Signs of parafunctional habits include waking in the middle of the night or morning with the teeth clamped together, waking with the muscles of the face and jaws feeling tired, having “tired teeth” in the morning as if the individual has been chewing gum all night, or waking with tenderness or pain in front of the ear. Any of these signs is an indication the patient is grinding/clenching during sleep and that intervention is indicated.
SUMMARY
The role of occlusion in the progression of periodontal disease remains controversial.13,14 While not definitive due to the inability to perform an ethical controlled clinical trial, current data seem to indicate that occlusal discrepancies and certain types of occlusal contacts contribute to the progression of periodontal disease, and that treatment of occlusal discrepancies has a beneficial therapeutic effect. As a result, occlusal evaluation and treatment, if indicated, should be an integral part of periodontal therapy.
REFERENCES
- Karolyi M. Beobachtungen über pyorrhea alveolaris. Öst. Ung. Vierteeljschr Zahnheilk. 1901;17:279.
- Stillman PR. The management of pyorrhea. Dent Cosmos. 1917;59:405–414.
- Glickman I, Smulow J. The combined effects of inflammation and trauma from occlusion in periodontitis. Int Dent J. 1969;39:101–105.
- Waerhaug J. The angular bone defect and its relationship to trauma from occlusion and downgrowth of subgingival plaque. J Clin Periodontol. 1979;6:61–82.
- Polson A, Zander H. Effects of periodontal trauma on intrabony pockets. J Periodontol. 1983;54:586–591.
- Ericsson I, Lindhe J. Effect of longstanding jiggling on experimental marginal periodontitis in the beagle dog. J Clin Periodontol. 1982;9:497–503.
- Gher M. Non-surgical pocket therapy: Dental occlusion. Ann Periodontol. 1996;1:567–580.
- Nunn ME, Harrel SK. The effect of occlusal discrepancies on treated and untreated periodontitis: I. Relationship of initial occlusal discrepancies to initial clinical parameters. J Periodontol. 2001;72:485–494.
- Harrel SK, Nunn ME. The effect of occlusal discrepancies on treated and untreated periodontitis II. Relationship of occlusal treatment to the progression of periodontal disease J Periodontol. 2001;72:495–505.
- Harrel SK, Nunn ME. Longitudinal comparison of the periodontal status of patients with moderate to severe periodontal disease receiving no treatment, non-surgical treatment, and surgical treatment utilizing individual sites for analysis. J Periodontol. 2001;72:1509–1519.
- Harrel SK, Nunn ME. The effect of occlusal discrepancies on gingival width. J Periodontol. 2004;75:98–105.
- Harrel SK, Nunn ME. The association of occlusal contacts with the presence of increased periodontal probing depth. J Clin Periodontol. 2009;36:1035–1042.
- Harrel SK, Nunn ME, Hallmon WW. Is there an association between occlusion and periodontal destruction?: Yes — occlusal forces can contribute to periodontal destruction. J Am Dent Assoc. 2006;137:1380–1384.
- Deas DE, Mealey BL. Is there an association between occlusion and periodontal destruction?: Only in limited circumstances does occlusal force contribute to periodontal disease progression. J Am Dent Assoc. 2006:137:1381–1385.
Feature image courtesy of MKARCO/ISTOCK/ THINKSTOCK
From Decisions in Dentistry. December 2016;2(12):42-45.

