

Handling Medical Emergencies In Dental Settings
Preparation and practice, along with reviewing patients’ medical histories and vital signs, will help dental teams assess risk and appropriately respond to medical emergencies.
Preparation and practice, along with reviewing patients’ medical histories and vital signs, will help dental teams assess risk and appropriately respond to medical emergencies
PURCHASE COURSE
This course was published in the February 2019 issue and expires February 2022. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
Medical emergencies in dental settings occur for a variety of reasons. A survey revealed that among 2704 dentists polled over a 10-year period, more than 13,000 medical emergencies took place.1 The chief reason is an increase in the number of older adults seeking dental services. In addition, many of these patients utilize polypharmacy, which, in turn, can increase medical complications.2,3 Another factor stems from medical advances that are allowing patients who are medically compromised to live a higher quality life, which includes seeking dental services.2,3 In clinical practice, these varied conditions and prescriptions must be considered when selecting dental anesthetics, as they may inhibit a patient’s ability to adapt to stressful situations.4
This course was published in the February 2019 issue and expires February 2022. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the scope of medical emergencies in dental practice, and how teams can prepare to manage these events.
- List common types of medical emergencies encountered in dental settings.
- Explain ways to assess risk and appropriately respond to emergencies.
For these reasons, dental professionals are advised to work toward preventing medical emergencies.5 One way to do this is by collecting a detailed medical history for every patient and updating the history at each visit (with a new medical history document at least once every five years).5,6 A detailed and thorough medical history includes all over-the-counter and prescription medications, with the date started, drug name, dosage, directions, and the reason for taking each medication. When updating the history, patients should have an opportunity to review the documentation and sign to confirm the information is accurate.
An important part of the medical history is documenting the patient’s vital signs, which include respiration, pulse, blood pressure, height, weight and temperature.7 By taking blood pressure at each visit, dental teams can review and discuss the blood pressure readings and make referrals for further evaluation when indicated.8 Hypertension is indicative of risk for an emergency in the dental setting. In addition, patients may not be monitored by a primary care provider and therefore may be unaware of potentially dangerous blood pressure levels. With the publication of updated blood pressure guidelines in 2017,9 dental personnel are advised to follow the updated guidelines, refer patients to medical providers when appropriate, and educate patients on the effects of hypertension.7,9
By reviewing medical histories and vital signs, oral health professionals are able to more accurately assess risk for an emergency in the dental office. Clinicians should use a risk classification system, such as the American Society of Anesthesiologists Physical Status Classification System, to document the patient’s risk of experiencing a medical emergency (Table 1).6,7
PREPARATION IS KEY
While preventing medical emergencies should be the primary goal, it is nearly impossible to predict and prevent every emergency scenario. As such, being prepared for dental emergencies is paramount to successful management. The first thing a dental team should do when preparing is select, review and understand the contents of the emergency kit.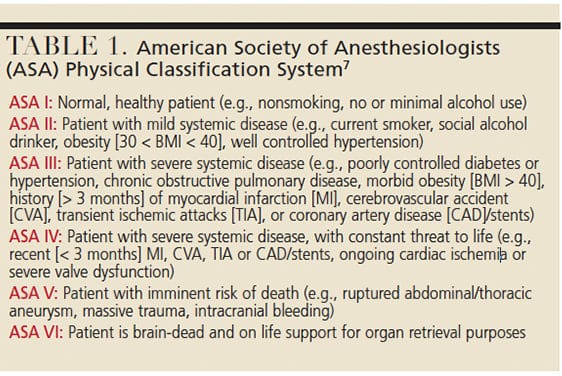
The scope of the dental setting will determine the level of equipment, supplies and medications in the emergency kit.10 A practice that offers conscious sedation, for example, should be prepared with advanced cardiac life support equipment, supplies and medications,10 while an office that does not offer more invasive treatment may carry a more basic kit. Regardless of the kit, all team members should be familiar with its equipment and contents.
Every dental setting should have at least a basic emergency kit that contains oxygen, an automated external defibrillator (AED), albuterol (rescue inhaler), aspirin, diphenhydramine (antihistamine), and auto-injectors of epinephrine, nitroglycerin and glucose.10 The kit should be evaluated (and logged) monthly to confirm that no items have expired.11
Effective emergency management requires a team approach, and for all staffers to play a key role during an emergency.7,11,12 All dental offices should hold at least annual drills. These should include a review of who will be the leader in charge of managing the response (Team Member 1), who will secure the emergency equipment, supplies and medications (Team Member 2), and who will call 911 (Team Member 3).12 Usually, the dentist is Team Member 1, but an alternate should be designated in case the dentist is not in the office.
Team Member 1 manages the emergency and makes decisions on appropriate steps. In the dental setting, the team is responsible for the patient’s safety and well-being. Therefore, Team Member 1 stays with the patient at all times until help arrives (and sometimes accompanies the patient to the emergency department).13 After 911 is called, Team Member 3 waits outside of the building to escort the first responders to the setting.13 Team Member 3 can then assist with preparing procedural notes (which are often incomplete and should be labeled as such) and the emergency documentation form.12,13 Team Member 2 monitors vital signs and prepares any medication(s) to be administered.7,12
All dental practices should have an emergency plan in place.12 It should include emergency drill scheduling, identification of who will fulfill specific roles during the emergency, and who will make copies of emergency documentation forms. The plan should also iterate that all emergencies will be handled with the position, airway, breathing and circulation (or PABC) approach.12
Under the team concept, effective communication is crucial to medical emergency management. Participants should practice communication during annual or biannual drills. A best practice includes repeating what is stated to check for clarity and reiterate for the individual who is documenting the events that unfold.12 It is also good practice to invite local emergency medical technicians/paramedics to participate in drills.13 This interdisciplinary interaction will assist in the transfer of the patient who is experiencing a medical emergency.
COMMON EMERGENCIES IN DENTISTRY
Syncope: The most common medical emergency in dentistry is syncope,7,14 and the most accepted reason is because dental settings can be perceived as a stressful environment. The stressors can be physical and/or psychological.7 Physical stressors can include discomfort from a procedure or pain due to an infection. Psychological stressors include anything that can be perceived as unpleasant. This may include visualizing needles, blood or tissue, smelling dental aromas, and hearing a dental handpiece or another patient reporting pain or discomfort.
The body’s response to stress can result in blood pooling in the extremities, a physiological process known as the fight-or-flight response.7 However, the pooling blood is not helpful, especially when the individual is in the dental chair. Due to positioning and lack of mobility in the chair, a lack of oxygenated blood is pumped to the brain, which leads to syncope.7
No matter the cause, a dental professional who suspects a patient is in presyncope should immediately and calmly place the patient in the Trendelenburg position (head below the heart and feet elevated 10 to 15 degrees).6 If the patient experiences syncope, identifying the cause will aid appropriate situation management. Once a patient recovers, the provider and patient will determine if treatment should be discontinued. Monitoring the patient before dismissal is recommended. In many cases, it is prudent to have a friend or relative take the patient home and monitor the individual until he or she regains normalcy.
Anaphylaxis: Patients who experience a severe allergic reaction, or anaphylaxis, should be assisted with administration of an auto-injector of epinephrine.15 These auto-injectors are packaged with a trainer so dental professionals can use the trainer during emergency drills to learn how to administer the medication and familiarize themselves with how the delivery system works.13 The adult dosage is 0.3 mg epinephrine and the child dosage is 0.15 mg epinephrine. All dental settings should have at least two auto-injectors available in case the first dose insufficient. It is prudent to call 911 in the case of a severe allergic reaction and ensure follow-up testing to identify the cause of the episode.
Asthmatic Attack: Asthma is a common respiratory ailment, and dental professionals are encouraged to ask these patients to bring their bronchodilators (albuterol) to appointments in case the need arises. Dental settings should also stock a rescue inhaler in the emergency kit in the event a patient does not have a bronchodilator available. For the conscious patient who is experiencing an asthmatic attack (bronchospasm), clinicians can assist the patient in administering his or her medication and deliver supplemental oxygen.15 If the bronchospasm persists despite use of a bronchodilator, the team may suspect the patient is experiencing status asthmaticus.7,14 This is the most severe form of asthma and does not respond to normal drug therapy.7,14 It is essential to call 911 because these patients require immediate medical attention to prevent death.
Diabetes: Diabetes is a complex and chronic condition that can lead to medical emergencies in the dental office.7 Oral health professionals are advised to ask patients with diabetes when the last time they ate, if they test their blood glucose on a regular basis, and if they take their medication(s) as prescribed. Dental offices should have a blood glucose testing kit with strips available to monitor current readings. Inquiring about the most current HbA1c reading provides additional information regarding the level of disease control. It is becoming more common for patients to use a continuous glucose-monitoring device, and these individuals are usually very knowledgeable about their blood glucose levels.
Although hypoglycemia can occur in nondiabetic patients, it is more important to ask patients with diabetes the last time they ate to discern their risk of hypoglycemia. Patients who are more likely to experience hypoglycemia often skip meals, do not eat enough, or experience higher than normal levels of stress. If a patient exhibits sweating, increased anxiety and nervousness, the clinician should position the patient upright and deliver an oral carbohydrate.15 Therefore, oral carbohydrates — such as crackers, candy bars, juices, or a glucose paste or tablet — should be included in the emergency kit.10 After the patient has something to eat, the individual’s blood glucose should be tested to determine if it is safe to proceed with the appointment.
If a patient with hypoglycemia becomes unconscious, the individual should be placed in a supine position, with the legs elevated.7 An unconscious patient exhibiting hypoglycemia should be administered glucagon to reverse the emergency and 911 should be called.
Seizures: Accounting for 90% of the seizures that occur in dental settings,14 grand mal seizures are what most people envision when they think of seizures. Also known as clonic/tonic seizures, grand mal seizures are characterized by three phases.7
Phase I is the period before the patient begins to seize. Patients in Phase I may experience an aura. A flash of light may trigger a seizure, which is why it is important to control the dental unit light and any lighting worn on loupes. When the patient enters Phase II, or the convulsive phase, the individual exhibits an epileptic cry, which is the sound of air rushing from the lungs as the patient loses consciousness.15 The body becomes rigid for 20 to 30 seconds, and may move violently for two to five minutes.7 During this period, the dental team should discontinue treatment, remove anything from the mouth, and strive to protect the patient from injury. After the tonic and clonic movements have ceased, the patient enters Phase III, or the postictal phase, and regains consciousness. At this point, the patient may be confused, tired and embarrassed. Due to the loss of control over the smooth muscles during a seizure, the patient may have urinated or have excess frothy saliva.15 The dental professional should be prepared to suction and reassure the patient. This individual faces increased risk of entering into Phase II again, so stressful stimuli should be minimized. The patient should be escorted home, closely monitored, and advised to follow up with a medical provider in timely fashion.
Hyperventilation: Hyperventilation is nearly always caused by anxiety. High levels of anxiety in the dental setting can result in rapid breathing, which reduces the amount of carbon dioxide in the blood.7 The clinician may notice the patient seems nervous, has increased respirations, and reports a tightness in the chest and tingling in the fingers and toes.14 A patient who is hyperventilating should be placed in an upright position,14 and clinical teams are advised to help the patient take slow, deep breaths from the lower diaphragm. If necessary, the patient can be instructed to cup the hands over the nose and mouth and breathe slowly.14 These patients have too much oxygen due to increased respirations, so supplemental oxygen is contraindicated.7,14,15 If the emergency continues, call 911. Continued care may be necessary and emergency medical services may deliver antianxiety medication.
Partial or Complete Airway Obstruction: When it comes to medical emergencies, today’s practitioner has a number of resources to prevent airway obstructions. Many clinicians have an assistant, newer technology and equipment that can be helpful in suctioning. In addition, retraction devices and dental dams are available. As with any medical emergency, despite the team’s best efforts to prevent it, the emergency may happen and the team must be trained and ready to manage a situation related to an airway obstruction.
There are two types of airway obstruction a patient may present with. A partial airway obstruction is quite common, and the patient may cough and report that something “went down the wrong way.”14 The seriousness of the emergency elevates when the patient cannot get airflow and the partial obstruction becomes a complete airway obstruction.7,14 The universal sign of placing the hands over the throat is the hallmark sign of a complete obstruction.7
The first phase of a complete airway obstruction lasts one to three minutes and is characterized by the universal sign and an elevation in vital signs.7 The second phase involves a decrease in vital signs and, eventually, loss of consciousness. This phase lasts two to five minutes.7 The final phase occurs when vital signs cannot be measured. It is imperative the emergency is managed immediately upon onset due to the possibility of rapid progression. Clinicians are advised to conduct a visual exam and maintain the patient’s airway, breathing and circulation. Emergency assistance should be requested if the obstruction cannot be removed. A patient with a complete airway obstruction should be placed upright until the individual loses consciousness, at which point he or she should be placed in a supine position.7,14
According to American Red Cross guidelines, a series of five back blows, followed by five abdominal thrusts, should be administered to a person with a complete airway obstruction until the object is forced out or the patient becomes unconscious.16 If the patient is unconscious, a rescue breath, followed by chest compressions, should be delivered.16 The clinician should then look for an object in the mouth.16
Angina and Myocardial Infarction: Heart disease is the leading cause of death in the United States.7 For this reason and due to licensing requirements, all dental professionals are advised to be certified in cardiopulmonary resuscitation (CPR) with AED training (i.e., Basic Life Support training or CPR/AED certification). Atherosclerosis increases risk for myocardial infarction. In more mild cases of atherosclerosis, the patient may experience angina, which occurs when the heart experiences a decrease in oxygen.7 Angina can be categorized as stable or unstable.14 Stable angina usually occurs during physical activity because the heart experiences increased oxygen demand.14 Unstable angina occurs when plaques rupture or a blood clot forms, thereby reducing blood flow to the heart.14
Patients who have a history of angina may carry nitroglycerin tablets or spray. Dental teams are cautioned to ask these patients how frequently they use their nitroglycerin and place it on the counter near the working area in case it is needed during an appointment. A patient who experiences angina will complain of a dull, aching chest pain that is not localized. The pain may be steady and often the patient will remain still in hopes of alleviating the pain. The patient should be positioned upright and allowed to administer his or her own nitroglycerin sublingually.7,15 Supplemental oxygen and an additional dose can be delivered.15 If the pain continues without relief, a myocardial infarction should be suspected and 911 summoned.
A patient who is having a heart attack should be administered aspirin and supplemental oxygen immediately, and emergency protocols activated. A dental team member should retrieve the AED and call 911.10 If the patient loses consciousness and experiences cardiac arrest, the team should proceed with CPR and use the AED. Clinicians are cautioned to oversee the use of the AED until paramedics arrive and patient care is transferred.13
CONCLUSION
Medical emergencies can and do happen in dental settings. While it is always best to prevent an emergency, this is not always possible. Patients expect oral health professionals to take precautions to prevent medical emergencies and be prepared to manage situations that arise.17 Unfortunately, each year there are reports of dental office personnel not managing an emergency effectively.13 Emergencies must be managed using a team approach, and team members must be trained and comfortable in their roles. When professionals understand what is expected of them, action should overcome the fear and stress associated with a medical emergency.
Clinicians should follow the office emergency plan and document the event on the proper form and patient record. The team must also be familiar with all medical emergency equipment, supplies and medications in the office emergency kit. As noted, preparation is key, and toward this goal the office should conduct regular (at least annual) training drills and hold a debriefing after the exercises.
REFERENCES
- Malamed S. Knowing your patients. J Am Dent Assoc. 2010;141:S3–S7.
- De Bedout T, Kramer K, Blanchard S, et al. Assessing the medical emergency preparedness of dental faculty, residents, and practicing periodontists: an exploratory study. J Dent Educ. 2018;82:492–500.
- Ahamed A. Knowledge, attitude, and perceived confidence in handling medical emergencies among dental students. J Pharm Sci Res. 2016;8:645–649.
- Albelaihi A, Alweneen A, Ettish A, Alshahrani F. Knowledge, attitude, and perceived confidence in the management of medical emergencies in the dental office: A survey among the dental students and interns. J Int Soc Prev Community Dent. 2017;7:364–371.
- Kumarswami S, Tiwari A, Parmar M, Shukla M, Bhatt A, Patel M. Evaluation of preparedness for medical emergencies at dental offices: a survey. J Int Soc Prev Community Dent. 2015;5:47–51.
- Pickett F, Gurenlian J. The Medical History: Clinical Implications and Emergency Prevention in Dental Settings. Philadelphia: Lippincott, Williams and Wilkins; 2005.
- Malamed S. Medical Emergencies in the Dental Office. 7th ed. St. Louis, Mo: Elsevier; 2015.
- Wilkins EM. Clinical Practice of the Dental Hygienist. 12th ed. Philadelphia: Wolters Kluwer; 2017.
- Reboussin DM, Allen NB, Griswold ME, et al. Systematic review for the 2017 ACA/ AHA/ AAPA/ ABC/ ACPM/ AGS/ APhA/ ASH/ ASPC/ NMA/ PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: A report of the American College of Cardiology/ American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71:e116–e135.
- Rosenberg M. Preparing for medical emergencies: The essential drugs and equipment for the dental office. J Am Dent Assoc. 2010;141(Suppl 5):14S–19S.
- Fonner A, Reed K. Be prepared: How to handle a medical emergency in the dental office. Dimensions of Dental Hygiene. 2013;11(5):48–51.
- Haas D. Preparing dental office staff members for emergencies: developing a basic action plan. J Am Dent Assoc. 2010;141(Suppl 5):8S–13S.
- Rayner C, Ragan M. Are you ready for emergency medical services in your oral and maxillofacial surgery office? Oral Maxillofac Surg Clin North Am. 2018;30:123–135.
- Grimes E, Vermont Technical College. Medical Emergencies: Essentials for the Dental Professional. 2nd ed. Upper Saddle River, NJ: Pearson; 2014.
- Lawson L. Medical emergency preparedness in dental practice. Available at: https:/ / www.dentalacademyofce.com/ courses/ 3305%2FPDF%2F1706cei_ Lawson_ web.pdf. Accessed January 7, 2019.
- American Red Cross. Adult First Aid/ CPR/ AED: Ready Reference. Available at: https:/ / www.redcross.org/ content/ dam/ redcross/ atg/ PDF_ s/ Health_ _ _ Safety_ Services/ Training/ Adult_ ready_ reference.pdf. Accessed January 7, 2019.
- Sangrik, LJ. Malpractice Issues Surrounding Medical Emergency Preparedness in Dentistry. Available at: https:/ / www.dentaleconomics.com/ articles/ print/ volume-108/ issue-1/ practice/ malpractice-issues-surrounding-medical-emergency-preparedness-in-dentistry.html. Accessed January 7, 2019.
Featured image by KATARZYNABIALASIEWICZ/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. February 2019;5(2):36—39.

