

Digital Technologies for Restorative Care
The key to successful implementation is a clinical understanding of the advantages and limitations of these modalities as they relate to each individual patient.
The key to successful implementation is a clinical understanding of the advantages and limitations of these modalities as they relate to each individual patient
Improvements in communication and quality of care, as well as integration of digital datasets and diagnosis, are just some of many benefits that computer aided design/computer aided manufacturing (CAD/CAM) brings to dentistry.1 This article will provide an overview of CAD/CAM applications in restorative care. The follow-up article in this series will explore patient treatment examples that involve the use of CAD/CAM technology. In general, the CAD/CAM process involves:
- Hardware that can scan a physical object and produce digital data
- Software that can process this data and allow design for production purpose
- Hardware that can produce the desired prosthesis, based on the digital design.2
It is generally accepted that CAD/CAM dentistry started with the desire to provide same-day, chairside restorations. In the early 1970s, Francois Duret, DDS, DSO, PhD, MS, MD-PhD, developed the concept of using digital technology to obtain impressions of teeth and for milling restorations.3 This led to the first functional three-dimensional (3D) intraoral scanner (IOS) in 1985 (Sirona; Bensheim, Germany).3 This technology, named Chairside Economical Restoration of Esthetic Ceramics (CEREC), paved the way for the development of chairside CAD/CAM systems and digital dentistry as a whole.
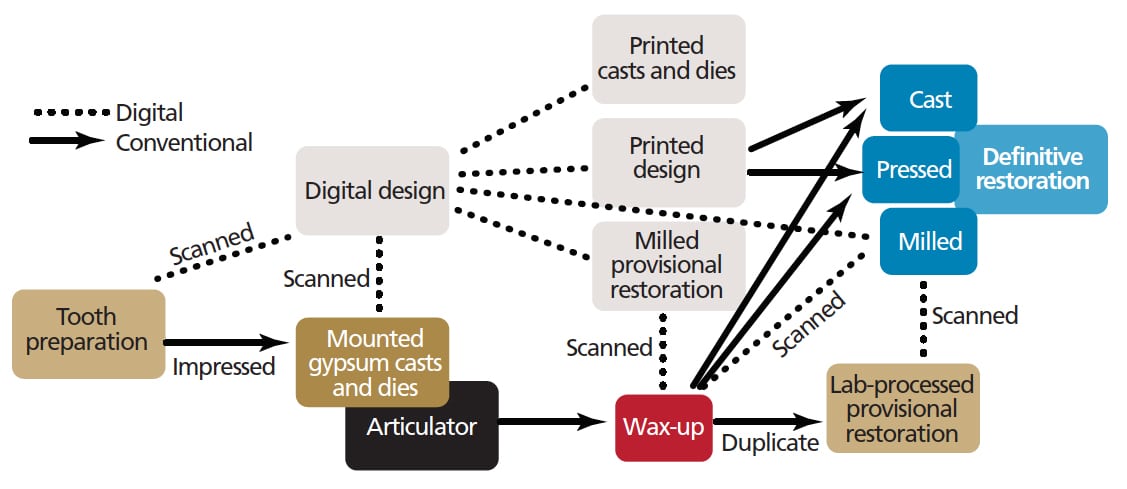
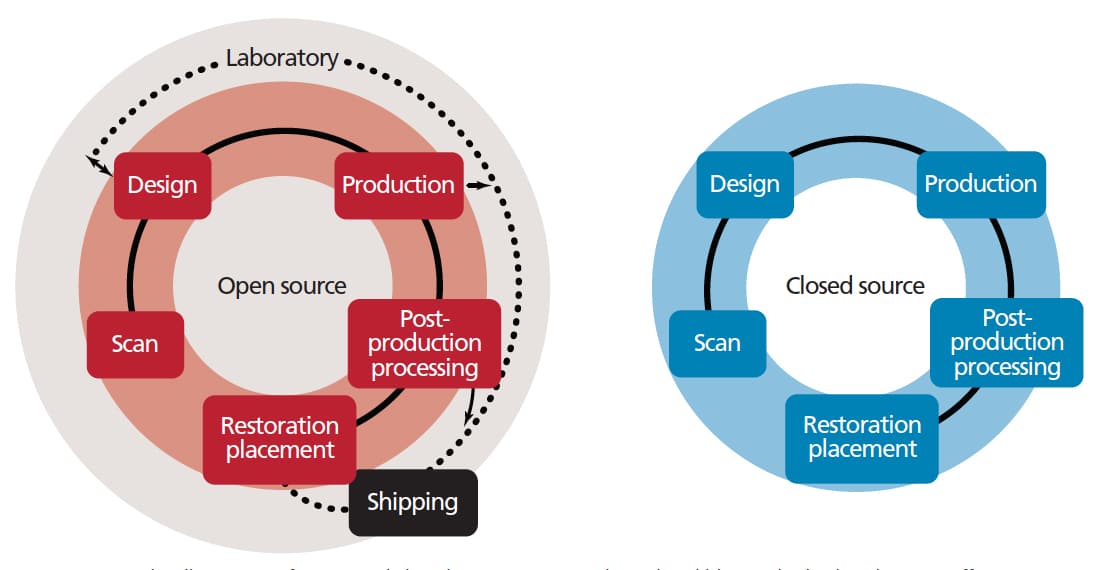
Following the introduction of chairside CAD/CAM dentistry, various systems now offer clinicians, laboratory technicians and patients the opportunity to choose different treatment paths, based on available conventional and digital methods (Figure 1). This versatility stems from the advent of open-access-file or “open-source” systems. For example, an open-source IOS allows clinicians to access and export files (e.g., standard tessellation language or STL files) to compatible in-office hardware to fabricate the desired prosthesis. If the clinical situation requires laboratory support, the provider has the option to send the design file to the lab for fabrication (Figure 2). An important consideration is that clinicians do not have to invest in all of the components of CAD/CAM system in order to embrace digital dentistry.
MILLING VERSUS PRINTING
Regarding fabrication methods, milling is an example of subtractive manufacturing technology. For most of the commercially available technology, it is categorized as either soft or hard milling. Soft milling is performed on materials that are not yet in their final form (either precrystallized or partially sintered), so they tend to be softer than their final state. The soft ceramic blocks or blanks are often said to be in “blue” or “white” state (lithium disilicate and zirconia, respectively). These softer materials are gentler to the milling unit in terms of tool wear than if they were milled in their final form.3 Once the milling is complete, however, the blocks require crystallization (lithium disilicate) or sintering (zirconia) in an appropriate furnace in order to fuse the ceramic particles. During this step, material shrinkage is a consideration, especially for zirconia, which can shrink approximately 20% (precrystallized lithium disilicate does not undergo such significant shrinkage during crystallization).3 For this reason, milling of the zirconia blocks in their final state (i.e., hard milling) avoids shrinkage and ensures accurate margins.3 Hard milling has become unpopular, however, because structural flaws and cracks can be introduced during fabrication.3
Unlike milling, 3D printing is an example of additive manufacturing technology. Printers based on stereolithography utilize a laser to cure liquid resin layer by layer into hardened plastic (via photopolymerization); such units are commonly used in dental offices and laboratories. The smoothness and accuracy of the printed resin varies depending on the thinness of the layers (known as “print resolution”), which can be as thin as 25 microns. The hardness and translucency of the resin can also vary, allowing different resins to be used for a range of indications. For example, a rigid and clear resin pattern printed at a high print resolution (e.g., 25 microns) is suitable for implant surgical guide, while an opaque, colored resin at an average print resolution of 50 to 100 microns may be sufficient for diagnostic casts.
MILLED DENTAL MATERIALS
Currently, milling is the generally preferred method of manufacturing ceramic restorations. Lithium disilicate and zirconia can cover a range of clinical situations and are commonly used for single crowns, whether they are tooth- or implant-supported. These materials can be used for anterior or posterior restorations due to their esthetics and strength. Implant abutments and full-arch prostheses (e.g., fixed complete dentures or “hybrid” prostheses) can be made out of these materials, as well.
As noted, an additional heat treatment step is needed after soft milling the precrystallized or “blue stage” lithium disilicate blocks, but clinicians have a chance to try the precrystallized restorations in the patient’s mouth to verify form and occlusion — and make necessary adjustments — prior to crystallization.
Soft milling of zirconia restoration can be accomplished predictably by making a larger design — either a die or restoration — to be milled. Zirconia coping pressed on the die and milled restoration will undergo uniform and controlled shrinkage.3 An appropriate coloring solution can be applied before sintering.3 These steps may be all that is required for fabricating monolithic zirconia restorations in the posterior region, thus eliminating veneering porcelain, which has been known to raise issues in terms of chipping.3
For 3D printing, development of printable resin has helped clinicians and laboratory technicians obtain the necessary prosthetic components for patient treatment. For cast alloy and pressed ceramic restorations, printed resin patterns (an equivalent in milling would be milled wax patterns) can replace conventional wax patterns that are subject to a dimensional change during handling and temperature fluctuations.3 Compared to conventional waxes, printed patterns can be highly accurate, strong and resistant to temperature changes. Appropriate investment materials for the printed patterns are available that can be processed in burnout ovens for casting metal alloy and pressing ceramic restorations. Until metal alloys can be printed predictably, these printed patterns can be used to produce clinically acceptable restorations.
Of course, materials continue to evolve. One example is zirconia-reinforced lithium disilicate that combines the esthetic quality of lithium disilicate and mechanical properties of zirconia.4
APPLICATIONS IN IMPLANT DENTISTRY
Like many areas of dentistry, implant dentistry greatly benefited from CAD/CAM technology. Improvements in imaging from two-dimensional to 3D images (i.e., cone beam computed tomography or CBCT) have improved diagnostic capabilities, planning, and patient education for implant treatment.
Various presurgical situations and treatment needs can indicate different protocols (e.g., single- versus double-scan) when planning implant surgery. In the single-scan protocol, only one CBCT scan is obtained (either with or without a radiographic guide). The double-scan protocol involves two CBCT scans: first, on the patient with a radiographic guide, and second, on the radiographic guide itself. Once obtained and processed with planning and design software, the digital impression data can be merged with the CBCT scan (the former is commonly an STL file, and the latter a digital imaging and communications in medicine or DICOM file). Next, the clinician can perform a digital wax-up or design representing the restoration and simulate a restoration-driven implant position. The digital workflow can continue with design and fabrication of a surgical guide and an immediate implant provisional restoration in the esthetic region for contouring the soft tissue early and ensuring patient satisfaction.
A definitive restoration can be designed and fabricated by obtaining a postsurgical impression digitally (again, using either an extraoral scan of a stone cast from an elastomeric impression, or an intraoral scan of the scan body indexing the implant position).
Thus, much of the implant treatment process can involve a digital workflow for the partially edentulous patient, especially if the clinician has an IOS and/or a desktop scanner, 3D printer and a milling unit. During this process, the need for a radiographic guide, impression materials, dental stone, wax-ups, and shipment of the necessary physical components to the dental laboratory can be obviated, increasing the efficiency, predictability and cost-effectiveness of therapy.
REMOVABLE PROSTHODONTICS
The use of CAD/CAM also offers advantages when it comes to removable prosthodontics. This technology can reduce the number of visits needed in the denture treatment process to two or three appointments, which can be beneficial to patients who rely on others for transportation. It also aids recordkeeping through the digital storage of scanned and designed data. Clinically, it provides prostheses that offer fit and strength superior to conventionally fabricated prostheses, and it helps decrease costs while increasing productivity.3
Clinicians experienced in using CAD/CAM denture systems can obtain the needed records (impression, interocclusal records and tooth selection) in one appointment.3 If a tooth setup try-in or trial denture is desired, a second appointment can be scheduled. Otherwise, with a successful first appointment, patients could receive their dentures at the second appointment.
Although printed dentures and record bases may be available in the near future, currently, CAD/CAM dentures are fabricated by milling prepolymerized acrylic resin. Milling is done on resin “pucks” or blanks that have been prepolymerized, so there is no shrinkage during or after milling — resulting in dentures that offer excellent fit.3 The milled denture has the potential to be more biohygienic than conventionally processed denture due to less residual monomer and increased hydrophobicity in the milled version.3 The teeth and denture base can also be milled as one (i.e., monolithic dentures), improving fracture resistance.3
For removable partial dentures (RPDs), clinicians can send a working cast of the impression to a laboratory that is equipped with appropriate hardware (scanner and printer) and software for designing and fabricating RPD metal frameworks. Once cast or scanned, a digital design of the framework can be made based on the clinician’s prescription. Next, a wax or resin pattern can be copy-printed or conventionally cast for a try-in, after which conventional denture processing takes place, with tooth setup and denture acrylic.3 New polymer materials, such as aryl-ketone polymers, are considered as a possible alternative to cast metal RPD frameworks, as these offer the potential to improve patient satisfaction with function and esthetics.5
DISCUSSION
According to the literature, the accuracy of intraoral digital impressions is comparable to, if not better than, conventional impressions.6 The marginal fit of CAD/CAM restorations also demonstrates clinically acceptable outcomes.7 Studies of CAD/CAM implant surgical guides indicate the use of a guide simplifies the surgical procedure and improves the precision of implant placement.8 Overall, numerous studies support the benefits of using CAD/CAM technology in various aspects of dentistry.
That noted, a common thread among the areas of dentistry influenced by CAD/CAM is that the technology is relatively new. Consequently, there is a lack of long-term, large-scale studies supporting (or challenging) the use of the technology and associated materials. The strength of the available evidence could also use improvement, as much of the study findings are based on in vitro methodology. Currently, there is no true evidence suggesting one material, method or equipment — or combination of these elements — is the best in any given situation. Therefore, the strengths and weaknesses of this ever-changing technology must be understood before making a decision to incorporate these processes into patient care.
RAMIFICATIONS AND CONCLUSION
“I do not need to learn how to do a wax-up.” Such a statement may have been unthinkable to dental students in the past, but the way students value some of the conventional methods in dentistry may be changing. As dental schools increasingly adopt CAD/CAM and other digital technology in their preclinical and clinical settings, a paradigm shift in education appears inevitable. What is not likely to change, however, is that thorough diagnosis, prognosis, treatment planning, and understanding of patient needs all come from a well-trained, experienced and thoughtful clinician — or sometimes, a team of clinicians.
Students and educators should keep in mind that CAD/CAM and other digital technology cannot replace the years of experience and training needed to provide patients with the care they deserve. Ultimately, the goal of digital dental technology, like any proven conventional method, is improving treatment outcomes for patients — not merely adding convenience or efficiency to the treatment process.
Without a doubt, CAD/CAM workflows are an integral part of dentistry today. Not only will these technologies continuously improve, they are also likely to present new solutions for complex and demanding situations. As with all modalities, the key to successful outcomes is a clinical understanding of the advantages and limitations of the technology, and how these relate to the specific case and patient’s best interests.
KEY TAKEAWAYS
- Clinicians do not have to invest in all components of a computer aided design/computer aided manufacturing (CAD/CAM) system in order to embrace digital dentistry.
- Soft milling is performed on dental materials that are not yet in their final form (either precrystallized or partially sintered), so they tend to be softer than their final state.
- Once soft milling is complete, the blocks require crystallization (lithium disilicate) or sintering (zirconia) in an appropriate furnace in order to fuse the ceramic particles.
- Milling of zirconia blocks in their final state (known as hard milling) avoids shrinkage issues and ensures accurate margins, but can introduce structural flaws and cracks.3
- The development of printable resin has helped clinicians and laboratory technicians obtain the necessary prosthetic components for treatment via the use of three-dimensional printers.
- While studies support CAD/CAM’s benefits, because most of these modalities are relatively new, there is a lack of long-term, large-scale studies supporting (or challenging) the use of these technologies and materials in dentistry.
References
- Cooper LF, Ludlow ME. American College of Prosthodontists. The Current Impact of Digital Technology in Prosthodontics. Available at: prosthodontics.org/assets/1/7/Digital_White_Paper_r1.pdf. Accessed April 16, 2018.
- Beuer F, Schweiger J, Edelhoff D. Digital dentistry: an overview of recent developments for CAD/CAM generated restorations. Br Dent J. 2008;204:505–511.
- Masri R, Driscoll CF, eds. Clinical Applications of Digital Dental Technology. Hokobken, NJ: John Wiley & Sons; 2015:28,76,80,81,83,109,110,135.
- Denry I, Kelly JR. Emerging ceramic-based materials for dentistry. J Dent Res. 2014;93:1235–1242.
- Campbell SD, Cooper L, Craddock H, Hyde TP, Nattress B, Pavitt SH, Seymour DW. Removable partial dentures: The clinical need for innovation. J Prosthet Dent. 2017;118:273–280.
- Chochlidakis KM, Papaspyridakos P, Geminiani A, Chen CJ, Feng IJ, Ercoli C. Digital versus conventional impressions for fixed prosthodontics: a systematic review and meta-analysis. J Prosthet Dent. 2016;116:184–190.
- Contrepois M, Soenen A, Bartala M, Laviole O. Marginal adaptation of ceramic crowns: a systematic review. J Prosthet Dent. 2013;110:447–454.
- Geng W, Liu C, Su Y, Li J, Zhou Y. Accuracy of different types of computer-aided design/computer-aided manufacturing surgical guides for dental implant placement. Int J Clin Exp Med. 2015;8:8442–8449.
Featured image by MARKO RUPENA/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. May 2018;4(5):33-36.

[…] Choi SK. Digital technologies for restorative care. Decisions in Dentistry. […]