

Conservative Caries Treatment
Adopting a minimally invasive approach and implementing evidence-based management protocols can preserve tooth structure and improve outcomes.
Adopting a minimally invasive approach and implementing evidence-based management protocols can preserve tooth structure and improve outcomes
It has been well over 100 years since G.V. Black advocated his principles of cavity preparation. Black’s approach to caries treatment was termed the “extension for prevention” concept,1 and showed little regard for the preservation of healthy tooth structure. The strategy was mainly surgical and followed a “see and treat” rationale.
Through advances in research and scientific innovations, new and more effective restorative materials and techniques have given clinicians more options for treatment. In addition to surgical intervention, research findings have introduced the concept of disease management as a viable approach to therapy.2 Black himself made this prophetic statement in 1896: “The day is surely coming … when we will be engaged in practicing preventive, rather than reparative, dentistry.”3 Today, new materials and an approach advocating disease management represent a paradigm shift in caries treatment.2 In the clinic and classroom, practitioners and dental students are being taught and encouraged to embrace minimally invasive strategies.4 Toward this goal, they can harness specialized tools, such as the International Caries Detection and Assessment System (ICDAS) and International Caries Classification and Management System (ICCMS), to more effectively manage lesions.
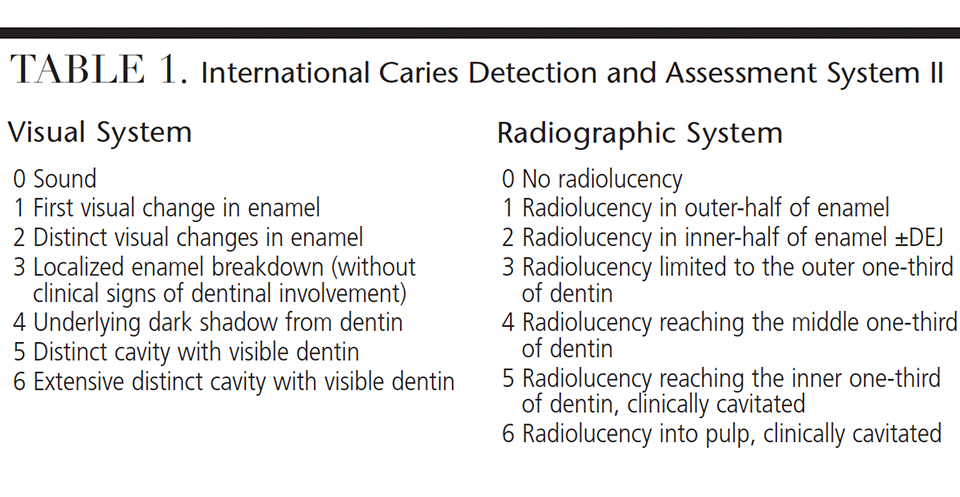
Evidence continues to be presented in support of a conservative approach that emphasizes the importance of establishing a dental home at an early age and the need for appropriate self-care. Preventive procedures — including prophylaxes, fluoride therapy and sealants — are key management tools, with early treatment rendered when necessary.4,5 Early diagnosis played an integral role in the minimally invasive model of treatment. Developed in 2002, ICDAS introduced a standardized method for assessing caries.6 The current system, ICDAS II, is evidence-based and provides a visual and radiographic means of caries assessment7 (Table 1); both systems are scaled from 0 to 6 and offer descriptive explanations at each level.8,9
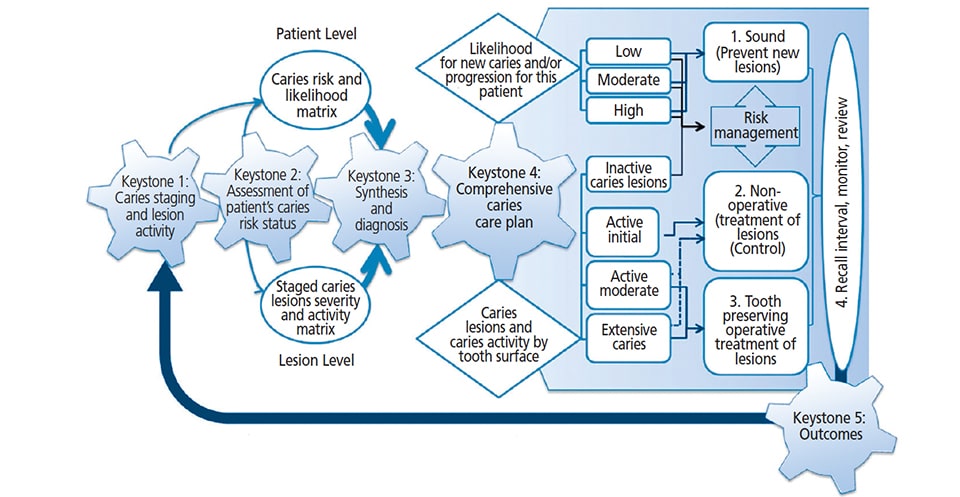
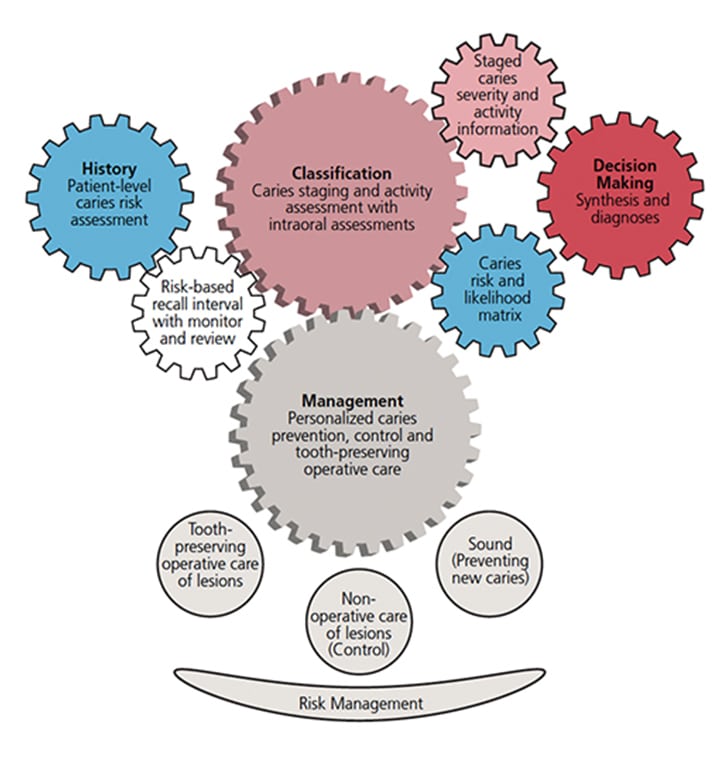
Although ICDAS II was developed for permanent teeth, its validation for use with primary teeth has also been established.10,11 Following the introduction of ICDAS, an international consensus workgroup proposed the ICCMS model (Figure 1), in which treatment is based on a key premise: “Preserve tooth structure and restore only when indicated.”9 There are four aspects to ICCMS: classification, management, history and decision-making (Figure 2).
- Classification entails diagnosing the extent and severity of caries.
- Management is customized for each patient and considers at the extent of the lesion, in conjunction with risk assessment, to determine the course of treatment — all while adhering to the principle of preserving tooth structure and incorporating preventive therapies.
- History involves gathering information to determine an individual’s risk assessment.
- Decision-making includes establishing a diagnosis, processing all information, and creating an individualized treatment plan that follows an established ICCMS pathway.9
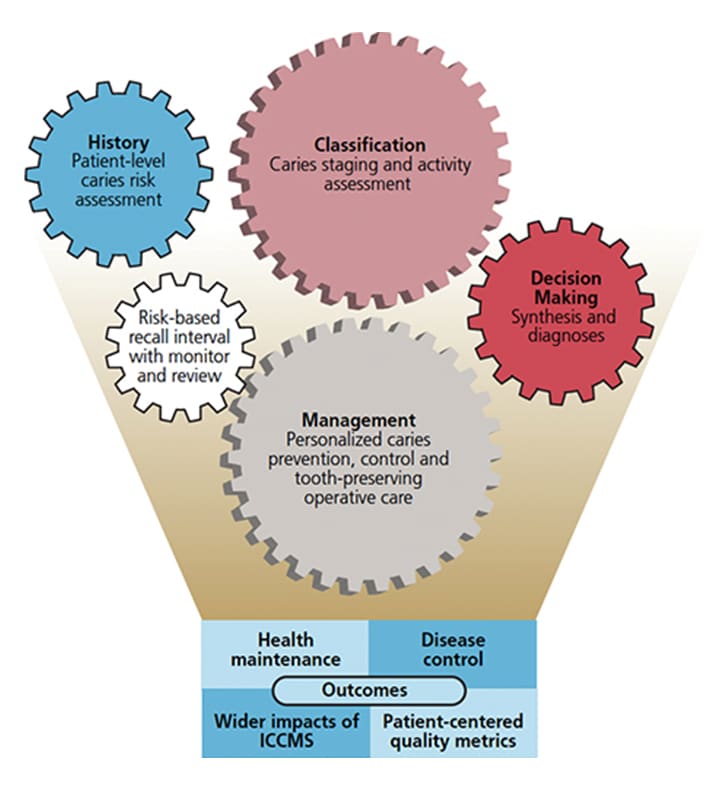
These four key aspects lead to outcomes, which include disease control, health maintenance, patient-centered quality metrics, and the impact of ICCMS (Figure 3).9
INDIVIDUALZED TREATMENT
Clinicians can choose from multiple caries risk assessment tools; in addition to the ICDAS and ICCMS protocols, these include those offered by the American Dental Association and American Academy of Pediatric Dentistry. Yet another tool is Caries Management by Risk Assessment (perhaps best known by its CAMBRA acronym).
Under both ICCMS and ICDAS, assessment classifications 1 and 2 are used for initial, early or minimal-stage lesions; ICDAS classifications 3 and 4 are considered to be at a moderate or established stage, while ICDAS classifications 5 and 6 describe extensive or severe-stage lesions.
Once a patient’s individual needs have been assessed using established methodologies and strategies, practitioners have numerous restorative approaches and techniques from which to select.9,12 By embracing an evidence-based customized pathway, clinicians can provide comprehensive preventive and restorative treatment tailored to the patient’s specific needs and circumstances.9,12
FLUORIDE VARNISH AND SEALANTS
The ICCMS protocol is linked to the concept of minimally invasive dentistry and follows an evidence-based approach.13 For lesions assessed as ICCMS class 1 or 2, clinically applied fluoride varnish can be effective as the first treatment modality for both permanent and primary teeth.9 Sealants are the next step in the treatment pathway for ICDAS stage 1 and 2 minimal lesions. As a form of restoration, sealants have been shown to significantly influence preservation of the occlusal surface of both primary and permanent molars.14 Clinicians can choose from resin-filled sealants, glass ionomer (GI) sealants, polyacid-modified-resin sealants, and resin-modified GI sealants. Resin-filled sealants are the more traditional and commonly used type. And while GI and resin-modified GI sealants contain fluoride, evidence has shown they are not the first choice for use on permanent teeth.15 Retention rates for GI and resin-modified GI sealants are lower than for modified-resin sealants; however, GI sealants are especially beneficial in cases of partial eruption of permanent molars, in which maintaining adequate moisture control could be an issue.16
The overall success rate of conventional sealants is dependent on maintaining adequate isolation and moisture control during application. However, less moisture-sensitive sealants are available and have proven effective.17 A recent systematic review and meta-analysis has shown the use of adhesive systems beneath fissure sealants can increase retention. It also demonstrated improved retention with the use of etch-and-rinse adhesive systems (as compared to self-etch adhesive systems).17 By forming a bonded protective layer, pit and fissure sealants act as a physical barrier. Minimal-stage caries that present in pits and fissures can be addressed by the application of sealants, which act to prevent bacterial contact with oral fluids. This seal essentially kills the pathogens and prevents caries progression.18
icdas.org/uploads/ICCMS-Guide_Full_Guide_UK.pdf. Accessed May 18, 2017.
Early on, sealants used in combination with resin-based composites proved efficacious in the concept of minimal invasive dentistry. They were an integral part of Simonsen’s19 introduction of the preventive resin restoration. Excavation was limited to removal of caries and surrounding dentin. Resin composite was placed as a restoration, with sealant material placed over the remaining occlusal surface. This conservative approach has proven itself as a successful form of minimally invasive dentistry.19
RESIN INFILTRATE AND GLASS IONOMERS
For smooth surface minimal lesions on interproximal surfaces, resin infiltrate has been shown to have similar effects in preventing bacterial progression.20 Application of resin infiltrate requires appropriate isolation and a dry field. Evidence has shown success using resin infiltrate in treating radiographically visible caries for stage 1, 2 and 3 lesions. The application of resin infiltrate has also been shown to be an effective, noninvasive approach for primary and permanent posterior teeth. Although early developing lesions traditionally would have been given a “watch” status, resin infiltrate allows successful treatment by preventing the opportunity for further progression and increased cavitation. As such, this noninvasive approach contributes to the preservation of tooth structure.20,21
The introduction of GI cements — and subsequent addition of resin-modified GIs — as restorative materials significantly impacted clinical treatment, as GI cement is considered the optimal restoration for minimally invasive dentistry and the ICCMS protocol.21 The advantages of GI and resin-modified GI cements are numerous: They are biocompatible, hydrophilic and bond to dentin and enamel; in addition, they offer thermal expansion similar to that of tooth structure. One of the most important features is their ability to release and recharge fluoride. There is also evidence that resin-modified GIs can perform successfully in small- to moderate-size Class II restorations.22
The ease of handling experienced with GIs, along with their ability to release fluoride, are key factors that led their use as an interim therapeutic restoration and with the atraumatic restorative technique (ART). The former is primarily used in young, uncooperative patients and those with special health care needs when placement of a definitive restoration is not possible. The latter was introduced in the 1900s, initially for caries management by providing a means of improving quality and access to oral health care for the underserved. Today, ART is an essential part of a minimally invasive approach, and is used throughout the world for preventing, treating and arresting further progression of caries. It is also a key component in treating minimal and moderate lesions in adherence with the ICCMS protocol.9
OTHER THERAPEUTIC SOLUTIONS
The use of resin-modified composites for certain moderate lesions permits what’s been termed “tooth-preserving operative care.”9 Successful placement of resin-based composites requires appropriate isolation and a dry field, as exposure to moisture during material placement could contribute to microleakage and, ultimately, restoration failure. Use of good technique and an adhesive system prior to placement are essential. The adhesive improves retention by optimizing the interface with dentin and enamel. Thus, less tooth structure needs to be removed for retention. In addition, adhesives help minimize microleakage and reduce sensitivity following treatment.23,24 Resin-based composites are not considered the material of choice for restorations in individuals at high caries risk, however, or in individuals who demonstrate poor oral hygiene and compliance.
For caries lesions that are considered moderate or extensive (ICDAS stage 4 and stage 5), less conservative treatment may be required. With the introduction of the Hall technique, stainless steel crowns have a role in minimally invasive dentistry for primary posterior teeth. Introduced in 1988 in Scotland, this technique involves cementing a stainless steel crown over a caries-affected primary molar, without caries removal, tooth preparation or administration of local anesthesia.25 Light finger pressure is used for crown placement, with full seating of the crown accomplished by instructing patient to bite down. Initial success rates were reported as 73.4% after three years and 67.6% after five years. Subsequent studies also showed favorable results. Even so, the Hall technique is controversial and has not gained wide acceptance.26 Nonetheless, it is considered to be a minimally invasive technique for managing early to moderately advanced active dentinal lesions in primary molars.13
In cases in which definitive treatment is not possible, consideration should be given to the use of silver diamine fluoride,27 as research has shown its effectiveness as an interim approach in arresting and hardening dentinal caries and preventing new lesions in treated teeth.28
FINAL THOUGHTS
When treating pediatric or adult patients, minimally invasive dentistry and utilization of the ICCMS or ICDAS protocols lets practitioners follow an evidence-based pathway in creating comprehensive, individualized treatment plans. This allows for the disease process to be managed not only effectively, but also early. With the ultimate goal of preserving maximum tooth structure, embracing preventive therapy and early intervention helps ensure optimal oral health.
KEY TAKEAWAYS
- In addition to surgical intervention, research findings have introduced the concept of disease management as a viable approach to treatment.
- Practitioners and dental students are encouraged to embrace minimally invasive strategies for caries management4 — and preventive procedures, including prophylaxes, fluoride therapy and sealants, are key management tools.
- Early diagnosis and assessment of caries play an integral role in minimally invasive treatment.
- Following the introduction of the International Caries Detection and Assessment System in 2002, an international consensus workgroup proposed the International Caries Classification and Management System, which is based on the premise: “Preserve tooth structure and restore only when indicated.”9
- By embracing an evidence-based customized pathway, clinicians can provide comprehensive preventive and restorative treatment tailored to a patient’s specific needs and circumstances.9,12
REFERENCES
- Black GV. A Work on Operative Dentistry. 2nd ed. Chicago, Ill: Medico-Dental Publishing Co; 1908.
- Featherstone JD. Dental caries: a dynamic disease process. Aust Dent J. 2008;53:286–291.
- Joseph R. The father of modern dentistry — Dr. Greene Vardiman Black (1836–1915). J Conserv Dent. 2005;8:5–6.
- Frencken JE, Peters MC, Manton DJ, Leal SC, Gordan VV, Eden E. Minimal intervention dentistry for managing dental caries — a review: report of a FDI task group. Int Dent J. 2012,62:223–243.
- Slayton RL. Clinical decision-making for caries management in children: an update. Pediatr Dent. 2015;37:106–110.
- Ismail AI, Sohn W, Tellez M, et al. The International Caries Detection and Assessment System (ICDAS): an integrated system for measuring dental caries. Community Dent Oral Epidemiol. 2007;35:170–178.
- Banting D, Eggertsson H, Ekstrand KR, et al. Rationale and evidence for the International Caries Detection and Assessment System (ICDAS II). Available at: scribd.com/document/77330435/Rationale-and-Evidence-ICDAS-II-September-11. Accessed May 18, 2017.
- Ekstrand KR, Luna LE, Promisiero L, et al. The reliability and accuracy of two methods for proximal caries detection and depth on directly visible proximal surfaces: an in vitro study. Caries Res. 2011;45:93–99.
- ICDAS Foundation. ICCMS Guide for Practitioners and Educators. Available at: icdas.org/uploads/ICCMS-Guide_Full_Guide US.pdf. Accessed May 18, 2017.
- Shoaib L, Deery CM, Ricketts DN, Nugent ZJ. Validity and reproducibility of ICDAS II in primary teeth. Caries Res. 2009;43:442–448.
- Braga MM, Morais CC, Nakama RC, Leamari VM, Siqueira WL, Mendes FM. In vitro performance of methods of approximal caries detection in primary molars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:e35–e41.
- Ismail AI, Pitts NB, Tellez M, et al. The International Caries Classification and Management System (ICCMS), an example of a caries management pathway. BMC Oral Health. 2015;15(Suppl 1):S9.
- Ismail AI, Tellez M, Pitts NB, et al. Caries management pathways preserve dental tissues and promote oral health. Community Dent Oral Epidemiol. 2013;41:e12–e40.
- Innes NP, Frencken JE, Schwendicke F. Don’t know, can’t do, won’t change: barriers to moving knowledge to action in managing the carious lesion. J Dent Res. 2016;95:485–486.
- Wright JT, Tampi MP, Graham L, et al. Sealants for preventing and arresting pit-and-fissure occlusal caries in primary and permanent molars: A systematic review of randomized controlled trials — A report of the American Dental Association and the American Academy of Pediatric Dentistry. J Am Dent Assoc. 2016;147:631–645.
- Antonson SA, Antonson DE, Brener S, et al. Twenty-four month clinical evaluation of fissure sealants on partially erupted permanent first molars: glass ionomer versus resin-based sealant. J Am Dent Assoc. 2012;143:115–122.
- Khatri SG, Samuel SR, Acharya S, Patil S, Madan K. Retention of moisture-tolerant and conventional resin-based sealant in six-to nine-year-old children. Pediatr Dent. 2015;37:366–370.
- Bagherian A, Shirazi AS, Sadeghi R. Adhesive systems under fissure sealants: yes or no?: A systematic review and meta-analysis. J Am Dent Assoc. 2016;147:446–456.
- Simonsen RJ. Preventive resin restorations: three-year results. J Am Dent Assoc. 1980;100:535–539.
- Altarabulsi MB, Alkilzy M, Petrou MA, Splieth C. Clinical safety, quality and effect of resin infiltration for proximal caries. Eur J Paediatr Dent. 2014;15:39–44.
- Walsh LJ, Brostek AM. Minimum intervention dentistry principles and objectives. Aust Dent J. 2013;58(Suppl 1):3–16.
- Chadwick BL, Evans DJ. Restoration of class II cavities in primary molar teeth with conventional and resin modified glass ionomer cements: a systematic review of the literature. Eur Arch Paediatr Dent. 2007;8:14–21.
- Hikita K, Van Meerbeek B, De Munck J, et al. Bonding effectiveness of adhesive luting agents to enamel and dentin. Dent Mater. 2007;23:71–80.
- Cardoso MV, de Almeida Neves A, Mine A, et al. Current aspects on bonding effectiveness and stability in adhesive dentistry. Aust Dent J. 2011;56(Suppl 1):31–44.
- Innes NP, Stirrups DR, Evans DJ, Leggate M. A novel technique using preformed metal crowns for managing carious primary molars in general practice — a retrospective analysis. Br Dent J. 2006;200:451–454.
- Seale NS, Randall R. The use of stainless steel crowns: a systematic literature review. Pediatr Dent. 2015;37:145–160.
- Quock RL. Silver diamine fluoride: An operative dentistry perspective. J Oper Esthet Dent. 2016;1:6–9.
- Crystal YO, Niederman R. Silver diamine fluoride treatment considerations in children’s caries management. Pediatr Dent. 2016;38:466–471.
The authors have no commercial conflicts of interest to disclose.
Featured Image by BANANASTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. June 2017;3(6):22—24,26—27.
