

Comprehensive Approach to Early Childhood Caries
Identifying high-risk individuals, providing patient-specific education, and embracing interprofessional care can help support pediatric oral health.
Identifying high-risk individuals, providing patient-specific education, and embracing interprofessional care can help support pediatric oral health
PURCHASE COURSE
This course was published in the December 2017 issue and expires December 2020. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the December 2017 issue and expires December 2020. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
- Define early childhood caries and its etiology.
- Discuss the role of risk assessment in caries prevention and management.
- Identify the importance of establishing a dental home in promoting oral health.
- Explain appropriate therapeutic and restorative approaches for caries management.
- Outline the role of medical providers in identifying caries risk in pediatric patients.
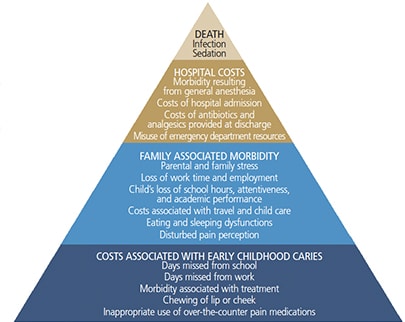
Dental caries remains a national and global public health epidemic, affecting children and adults from all races, ethnicities and socioeconomic levels.1–3 The signs and symptoms associated with caries include pain and infection from active lesions, nutritional deficiencies, learning and speech problems, and, rarely, death (Figure 1).2–5 Among children in the United States, caries is the most common unmet health need, with a prevalence of more than 25% among children age 24 months to 60 months.3
Caries is typically caused by disruptions in the balance between cariogenic bacteria and host factors, including enamel susceptibility, salivary flow and composition.2,6 Family culture, as well as economic and social status, also impact caries development.2,6 Current research demonstrates that multiple risk factors are responsible for caries, including frequent sugar consumption, improper or lack of oral hygiene, high levels of oral bacteria, socioeconomic status, race/ethnicity, and inconsistent access to oral health care.2,5,7–11
The American Academy of Pediatric Dentistry (AAPD) defines early childhood caries (ECC) as the presence of one or more decayed (noncavitated or cavitated lesions), missing (due to caries), or filled tooth surfaces (dmft) in any primary tooth in a child age 71 months or younger.12 In children younger than 36 months, any sign of smooth-surface caries is indicative of severe early childhood caries (S-ECC).12 Children age 36 months to 60 months who have one or more cavitated teeth, missing (due to caries), or filled smooth surfaces in primary maxillary anterior teeth, or a decayed, missing or filled score of ≥ 4 surfaces (36 months), ≥ 5 surfaces (48 months), or ≥ 6 surfaces (60 months) have S-ECC.12
Children between the ages of 12 months and 30 months have a unique pattern of caries development that differs from older children.7 Within this age group, ECC is distinguished by lesions found on the maxillary primary incisors and first primary molars, reflecting the pattern of eruption.1,2,4,13
ETIOLOGY AND RISK ASSESSMENT
Caries occurs when cariogenic bacteria colonize a susceptible tooth surface in the presence of carbohydrates.14 While more than 800 species of bacteria have been found in dental plaque,15–17 the four primary oral bacteria associated with caries are Streptococcus mutans, Lactobacilli, Streptococcus sobrinus, and Bifidobacteria.18
When carbohydrates and fermentable sugars are ingested, the pH of the oral cavity decreases, dropping from a neutral pH of 7.0 to an acidic pH of approximately 5.0 to 5.5.19 This increased acidity is also found within the biofilm fluid. If cariogenic bacteria are already present, the carbohydrates and fermentable sugars are metabolized by these acid-producing bacteria.19 Acid produced at the biofilm level diffuses into the enamel, causing structural demineralization.19 However, the enamel can remineralize once the carbohydrate exposure has ended.19 These cycles of demineralization/remineralization continue as long as cariogenic bacteria, fermentable carbohydrates and saliva are present. If this cycle occurs frequently, the demineralization eventually surpasses saliva’s remineralizing abilities, creating initial white-spot or incipient lesions that may progress to cavitation.14,19,20
A child’s risk of developing caries lesions is influenced by many factors and can change over time.14 Dietary patterns of carbohydrate consumption and other genetic, personal and social factors — such as oral hygiene habits, socioeconomic status and ethnicity — all affect caries development.2,6,7,20 Identifying a child’s caries risk is an effective and evidence-based approach to disease prevention and management. Caries management by risk assessment enables oral health professionals to recommend individually tailored therapeutic, restorative, oral hygiene, educational and nutritional approaches for pediatric patients and their parents or caregivers.21 This chairside assessment measures each child’s disease indicators, risk factors and protective factors, which help providers determine current and future caries disease status and risk.21
Through risk assessment, clinicians can identify cariogenic feeding patterns, assess the child’s use of fluoride toothpaste and frequency of fluoride varnish applications, and communicate to parents/caregivers the presence of active lesions or plaque. A caries risk assessment evaluation can be performed during any routine dental examination or prophylaxis.
ESTABLISH A DENTAL HOME
The AAPD defines a dental home as, “the ongoing relationship between the dentist and patient, inclusive of all aspects of oral health care delivered in a comprehensive, continuously accessible, coordinated and family-centered way. The dental home should be established no later than age 12 months and includes referral to specialists when appropriate.”22 An anticipatory approach emphasizing oral health promotion through guidance and parental/caregiver education is likely to have the greatest impact on children’s oral health.3,23 Preventive care visits can be used to reinforce the necessity and importance of maintaining routine dental examinations and prophylaxes. They also provide an opportunity to educate parents/caregivers about proper oral hygiene techniques, as well as behavioral and social risk factors.8 Nutritional education should be provided in order to ensure cariogenic feeding practices are avoided and proper dietary guidelines that support optimal oral and systemic heath are followed.
The goal of providing anticipatory guidance for parents/caregivers is to modify or eliminate practices and behaviors known to increase caries risk.3,24 According to the AAPD, care within a dental home should include comprehensive assessment, individualized preventive care based on caries risk, anticipatory guidance related to growth and development (including care of the child’s soft and hard tissues), education of parents/caregivers about management of acute dental trauma; nutritional assessment and counseling, and referral to specialists, if needed.22
A recent cross-sectional study explored the association of an established dental home on ECC prevalence and cariogenic feeding practices in high-risk populations.24 The caries disease status (dmft score), incidence of plaque and gingivitis, and the practice of high-risk dietary behaviors were compared among two groups of children (age 24 months to 60 months) differentiated by the presence of an established dental home. The study demonstrated significant relationships between higher dmft scores and frequent consumption of sticky snacks and sugary drinks, as well as prolonged drinking sessions of sugary beverages.24 Children with an established dental home had a lower prevalence of caries and lower rates of biofilm and gingivitis than children who did not have an established dental home. These findings add further evidence to support the effectiveness of oral hygiene education and anticipatory guidance in the prevention of adverse oral health outcomes.24
On the other hand, a recent study examining early prevention in the reduction of dental caries among Medicaid-enrolled children in Alabama did not find any benefits to the practice.25 Results showed that children who received preventive dental care before age 2 were more likely to need treatment for dental caries over several years. However, the study had significant limitations, including the use of claims data that did not consider quality of life improvement. Another was the lack of accounting for oral health behaviors that may have contributed to the increased need for follow-up dental care. Lastly, the investigators were not able to account for community water fluoridation, which may have impacted caries rates.25 Reasons as to why the study found no evidence supporting early prevention in caries reduction may be that more children sought early care simply because they had a dental home. In contrast, the rate of undiagnosed and untreated caries in children who did not receive early preventive care may be high. According to the Alabama Department of Public Health, approximately 20% of Alabama’s children aged 6 to 9 have untreated dental caries.26
THERAPEUTIC AND RESTORATIVE APPROACHES
Protective modalities, specifically topical fluoride, should be employed to inhibit demineralization, promote remineralization, and obstruct the formation of cariogenic plaque — especially in high-risk patients. The AAPD recommends that all children use fluoride toothpaste twice daily, regardless of caries risk.27 For children age 36 months and younger, no more than a “smear or rice-sized” amount should be used. For children between the ages of 36 months and 60 months, a pea-size amount is indicated. Using more than the recommended amount can increase the risk of fluorosis.27 The frequency of fluoride varnish (5% NaF) application is determined by the child’s caries risk; application intervals for pediatric patients at high-caries risk are typically every three to six months.
Multiple factors should be considered when determining restorative treatment for pediatric patients with ECC. Clinicians need to consider the child’s age and future caries risk, engagement of parents/caregivers, and severity of the lesions to determine an evidence-based course of action.28–32 Some children may be placed on “active surveillance,” a nonsurgical approach in which providers carefully monitor the progression of lesions through a specific plan of follow-up and behavior change. This approach includes active parental/caregiver engagement, frequent recare appointments with fluoride varnish applications, and consistent self-care measures, including brushing with fluoride toothpaste and improving dietary behaviors.30–32
If a pediatric patient requires restorative treatment, permanent restorations or interim therapeutic restorations — such as glass ionomer or resin-modified glass ionomer cement — can be considered.28 Silver diamine fluoride is a topical agent that has been shown to arrest caries; it can be used to address lesions in primary teeth.33–35
INTERPROFESSIONAL CARE
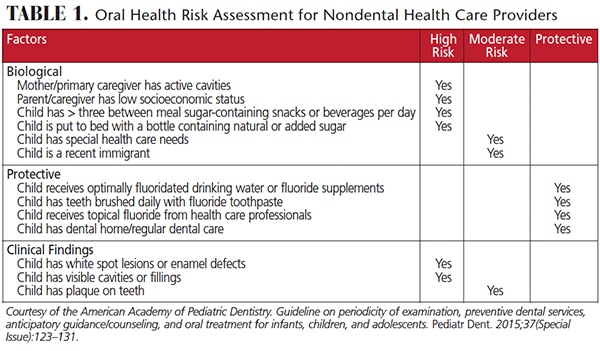
The role of pediatricians and allied medical providers in children’s oral health continues to grow as the oral/systemic connection becomes better understood. In response, schools are creating programs that incorporate oral/systemic health content, as well as clinical competencies, into nurse practitioner curricula; an example of this approach is New York University’s Rory Meyers College of Nursing’s Oral Health Nursing Education and Practice Program. Considering that nurse practitioners in pediatric settings have more frequent access to new mothers and infants than oral health professionals, improved oral health training can help them more efficiently recognize oral disease and identify high-risk cariogenic behaviors.36–38 According to the Medical Expenditure Survey, 89% of children younger than age 1 had routine physician visits annually, while only 1.5% of these children had dental visits.37 Another study indicates that 99% of Medicaid-enrolled children had well-baby visits before age 1, compared with only 2% who had a dental visit.36 Therefore, medical professionals need to incorporate oral health assessments into their preventive appointments (Table 1) to reinforce oral health-promoting behaviors, apply fluoride varnish, and facilitate the establishment of a dental home.36–38 In support of this, the majority of states reimburse nondental professionals for caries-prevention services performed during the medical appointment.39
The American Academy of Pediatrics recommends the first oral health risk assessment be performed by age 6 months, and continue at nine months, 18 months, 24 months, 30 months, 3 years and 6 years.40 The objective of performing caries risk assessment in the medical home is to prevent disease by identifying and decreasing contributory factors, while optimizing protective factors — specifically, fluoride exposure, proper oral hygiene and sealant placement.29,38,41 Risk assessment also enables medical providers to identify high-risk patients and refer them to oral health professionals.
A growing body of evidence suggests oral health is essential to systemic health. Considering that family, economic and social statuses significantly impact the development of ECC, emphasizing oral health-promoting behaviors is likely to have the greatest effect on children’s oral health.6,42,43 Dental professionals, as well as medical providers, play a critical role in identifying high-risk behaviors and providing patient-specific education and counseling that will prevent or mitigate caries lesions. For high-risk pediatric patients, educating parents/caregivers about the known risk factors associated with ECC is imperative.5,6,8–11
REFERENCES
- Arora A, Scott JA, Bhole S, Do L, Schwartz E, Blinkhorn AS. Early childhood feeding practices and dental caries in preschool children: a multi-centre birth cohort study. BMC Public Health. 2011;11:28.
- Kawashita Y, Kitamura M, Saito T. Early childhood caries. Int J Dent. 2011;2011:725320.
- Nunn ME, Dietrich T, Singh HK, Henshaw MM, Kressin NR. Prevalence of early childhood caries among very young urban Boston children compared with U.S. children. J Public Health Dent. 2009;69:156–162.
- Bugis BA. Early childhood caries and the impact of current U.S. Medicaid program: An overview. Int J Dent. 2012;2012:348237.
- Kagihara LE, Niederhauser VP, Stark M. Assessment, management, and prevention of early childhood caries. J Am Acad Nurse Pract. 2009;21:1–10.
- Harrison R. Oral health promotion for high-risk children: Case studies from British Columbia. J Can Dent Assoc. 2003;69:292–296.
- Nunn ME, Braunstein NS, Krall Kaye EA, et al. Healthy eating index is a predictor of early childhood caries. J Dent Res. 2009;88:361–366.
- Mobley C, Marshall TA, Milgrom P, et al. The contribution of dietary factors to dental caries and disparities in caries. Acad Pediatr. 2009;9:410–414.
- Palmer CA, Kent R Jr, Loo CY, et al. Diet and caries-associated bacteria in severe early childhood caries. J Dent Res. 2010;89:1224–1229.
- Warren JJ, Weber-Gasparoni K, Marshall TA, et al. A longitudinal study of dental caries risk among very young low SES children. Community Dent Oral Epidemiol. 2009;37:116–122.
- Prakash P, Subramaniam P, Durgesh BH, Konde S. Prevalence of early childhood caries and associated risk factors in preschool children of urban Bangalore, India: A cross-sectional study. Eur J Dent. 2012;6:141–152.
- American Academy of Pediatric Dentistry. Definition of Early Childhood Caries. Available at: aapd.org/assets/1/7/d_ecc.pdf. Accessed November 7, 2017.
- Losso EM, Tavares MC, da Silva JY, Urban CA. Severe early childhood caries: an integral approach. J Pediatr (Rio J). 2009;85:295–300.
- Caufield PW, Li Y, Dasanayake A. Dental caries: an infectious and transmissible disease. Compend Contin Educ Dent. 2005;26(Suppl 1):10–16.
- Aas JA, Paster BJ, Stokes LN, Olsen I, Dewhirst FE. Defining the normal bacterial flora of the oral cavity. J Clin Microbiol. 2005;43:5721–5732.
- Paster BJ, Boches SK, Galvin JL, et al. Bacterial diversity in human subgingival plaque. J Bacteriol. 2001;183:3770–3783.
- Preza D, Olsen I, Aas JA, Willumsen T, Grinde B, Paster BJ. Bacterial profiles of root caries in elderly patients. J Clin Microbiol. 2008;46:2015–2021.
- Mantzourani M, Gilbert SC, Sulong HN, et al. The isolation of bifidobacteria from occlusal carious lesions in children and adults. Caries Res. 2009;43:308–313.
- García-Godoy F, Hicks MJ. Maintaining the integrity of the enamel surface: the role of dental biofilm, saliva and preventive agents in enamel demineralization and remineralization. J Am Dent Assoc. 2008;139(Suppl):25S–34S.
- Filoche S, Wong L, Sissons CH. Oral biofilms: emerging concepts in microbial ecology. J Dent Res. 2010;89:8–18.
- Featherstone JD, Domejean-Orliaguet S, Jenson L, Wolff M, Young DA. Caries risk assessment in practice for age 6 through adult. J Calif Dent Assoc. 2007;35:703–713.
- American Academy of Pediatric Dentistry. The Dental Home. Available at: aapd.org/assets/1/7/DentalHomeNeverTooEarly.pdf. Accessed November 7, 2017.
- Edelstein B, Vargas CM, Candelaria D, Vemuri M. Experience and policy implications of children presenting with dental emergencies to U.S. pediatric dentistry training programs. Pediatr Dent. 2006;28:431–437.
- Kierce EA, Boyd LD, Rainchuso L, Palmer CA, Rothman A. Association between early childhood caries, feeding practices and an established dental home. J Dent Hyg. 2016;90:18–27.
- Blackburn J, Morrisey MA, Sen B. Outcomes associated with early preventive dental care among Medicaid-enrolled children in Alabama. JAMA Pediatr. 2017;171:335–341.
- Alabama Department of Public Health. The Oral Health of Alabama’s Kindergarten and Third Grade Children Compared to the General U.S. Population and Healthy People 2020 Targets. Available at: astdd.org/docs/al-3rd-grade-bss-2011-2013.pdf. Accessed November 7, 2017.
- American Academy of Pediatric Dentistry. Guideline on Fluoride Therapy. Available at: aapd.org/media/policies_guidelines/g_fluoridetherapy.pdf. Accessed November 7, 2017.
- American Academy of Pediatric Dentistry. Policy on Interim Therapeutic Restorations. Available at: aapd.org/media/policies_guidelines/p_itr.pdf. Accessed November 7, 2017.
- American Academy of Pediatric Dentistry. Guideline on Caries-Risk Assessment and Management for Infants, Children, and Adolescents. Available at: aapd.org/media/policies_guidelines/g_cariesriskassessment.pdf. Accessed November 7, 2017.
- American Academy of Pediatric Dentistry. Policy on Early Childhood Caries (ECC) Classifications, Consequences, and Preventive Strategies. Available at: aapd.org/media/policies_guidelines/p_eccclassifications.pdf. Accessed November 7, 2017.
- Arrow P KE. Minimum intervention dentistry approach to managing early childhood caries: A randomized control trial. Community Dent Oral Epidemiol. 2015;43:511–520.
- Edelstein BL. Chronic disease management strategies of early childhood caries: support from the medical and dental literature. Pediatr Dent. 2015;37:281–287.
- Horst JA, Ellenikiotis H, UCSF Silver Caries Arrest Committee, Milgrom PM. UCSF protocol for caries arrest using silver diamine fluoride: Rationale, indications, and consent. J Calif Dent Assoc. 2016;44:16–28.
- Shah S, Bhaskas V, Venkataraghavan K, Choudhary P, Ganesh M, Trivedi K. Efficacy of silver diamine fluoride as an antibacterial as well as antiplaque agent compared to fluoride varnish and acidulated phosphate fluoride gel: an in vivo study. Indian J Dent. 2013;24:575–581.
- Yee R, Holmgren C, Mulder J, Lama D, Walker D, van Palenstein Helderman W. Efficacy of silver diamine fluoride for arresting caries treatment. J Dent Res. 2009;88:644–647.
- Mouradian WE, Wehr E, Crall JJ. Disparities in children’s oral health and access to dental care. JAMA. 2000;284:2625–2631.
- Vargas CM, Ronzio CR. Disparities in early childhood caries. BMC Oral Health. 2006;6(Suppl 1):S3.
- Savage JS, Fisher JO, Birch LL. Parental influence on eating behavior: conception to adolescence. J Law Med Ethics. 2007;35:22–34.
- American Academy of Pediatrics. State Medicaid Payment for Caries Prevention Services by Non-Dental Professionals. Available at: paconnect.wpengine.netdna-cdn.com/wp-content/uploads/2013/07/AAP-OHReimbursementChart-2.pdf. Accessed November 7, 2017.
- Hale KJ, American Academy of Pediatrics Section on Pediatric Dentistry. Oral health risk assessment timing and establishment of the dental home. Pediatrics. 2003;111:1113–1116.
- Foster T, Perinpanayagam H, Pfaffenbach A, Certo M. Recurrence of early childhood caries after comprehensive treatment with general anesthesia and follow-up. J Dent Child (Chic). 2006;73:25–30.
- Oliveira AF, Chaves AM, Rosenblatt A. The influence of enamel defects on the development of ECC in a population with low socioeconomic status: A longitudinal study. Caries Res. 2006;40:296–302.
- Salone LR, Vann WF Jr, Dee DL. Breastfeeding: an overview of oral and general health benefits. J Am Dent Assoc. 2013;144:143–151.
FEATURED IMAGE BY CREDIT/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. December 2017;3(12):34—36,39.


[…] To learn more about a comprehensive approach to early childhood caries, click here: https://decisionsindentistry.com/article/comprehensive-approach-to-early-childhood-caries/ […]