

Caries Prevention Protocols
Implementing proactive management strategies can help reduce the prevalence of this ubiquitous — and preventable — disease.
Implementing proactive management strategies can help reduce the prevalence of this ubiquitous — and preventable — disease
PURCHASE COURSE
This course was published in the July 2017 issue and expires July 2020. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Discuss caries transmission and prevalence, as well as the basic premise of caries management by risk assessment (CAMBRA).
- Identify risk factors for caries development, and detail natural protective factors.
- List preventive and therapeutic strategies for caries management.
Dental caries is a transmissible bacterial disease that is frequently spread from mother to child — a process called vertical transmission.1 According to the U.S. Centers for Disease Control and Prevention (CDC), caries is the most common chronic disease of children ages 6 to 11 and adolescents ages 12 to 19.2 And while the prevalence of caries has been decreasing among older children, growing numbers of toddlers are presenting with decay.3 Dentists and dental hygienists are key players in the fight against caries in pediatric patients — and winning this fight hinges upon the successful implementation of an effective caries prevention strategy.
Caries management by risk assessment (CAMBRA) is an evidence-based protocol designed to prevent, reverse and/or treat caries before the disease process causes irreversible damage to tooth structure.4 CAMBRA is unique because it considers the entire caries disease process, instead of just progression of the lesion itself. This protocol treats caries as a highly infectious and transmissible bacterial disease that can be effectively treated and/or reversed.1 While traditional therapy has emphasized restorative care, CAMBRA focuses on prevention and early intervention by identifying at-risk patients and implementing strategies to prevent or reduce caries development.
CAMBRA is based on Featherstone’s5 caries balance theory, and uses risk assessment to determine treatment decisions. At the time CAMBRA was developed, the science supporting it was not new, but implementing the protocol into clinical practice was stalled until the formation of the Western CAMBRA Coalition in 2002. Dental professionals from five California dental schools met informally to discuss how to improve caries management standards.4 The group branched out to create a consortium that included constituents representing education, research and clinical practice. These efforts furthered CAMBRA’s reach through conferences, journal articles and public/private partnerships that promoted a clinical management philosophy in which the caries process is managed following a medical model.4
Since its introduction, CAMBRA has contributed to a new paradigm in caries treatment and management. Rather than isolating a single factor or condition, CAMBRA evaluates the presence of disease indicators and assesses the patient’s risk based on biological, behavioral and medical history factors. As a result, patient care is enhanced through use of a comprehensive, long-term customized approach.6
CARIES RISK ASSESSMENT
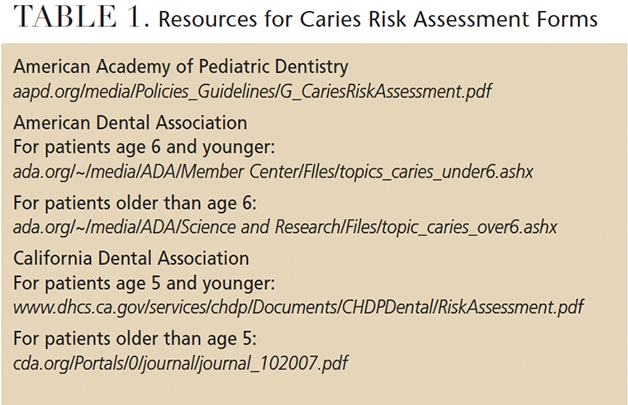
Today, caries risk assessment forms are easily accessed via the American Academy of Pediatric Dentistry, American Dental Association (ADA) and California Dental Association (Table 1). These tools provide a standardized format for assessing and documenting caries risk. Divided by age, each patient’s risk factors are noted on the form. The results are tallied, and the patient is categorized as low, moderate or high risk. Prevention and treatment plans are implemented based on designated risk. As a result of CAMBRA’s impact, in 2014 the ADA added three distinct Current Dental Terminology diagnostic codes — D0601, D0602 and D0603, representing low, moderate and high risk — for caries risk assessment reporting.
An important indicator of future caries risk is previous caries experience; and while this is key when treating children and adolescents, it has limitations when treating infants and toddlers.7 Caries risk factors are identified as biological (e.g., susceptible host, diet, microflora levels and socioeconomic status), and clinical (e.g., plaque accumulation, white spot lesions, precavitated lesions and caries).8–13 Additional factors include the presence of orthodontic appliances, xerostomia (disease-related or medication induced), special health care needs, bottle or nursing habits, incipient lesions (both radiographic and clinical), and caries within the first three years of life.14–16
The evaluation of the bacterial levels present in saliva is an important factor in caries risk assessment.9 Saliva serves many functions, including lubrication of the mucosa and helping in mastication, swallowing and speech. Saliva also protects teeth by acting as a buffer and neutralizing acids produced during the intake of foods and beverages, thus aiding in the remineralization of the tooth surface.17 The presence of Streptococcus mutans in saliva and plaque — regardless of whether caries is present — is an indicator of risk.18 A number of commercially available kits are available to help clinicians analyze the microflora present in a patient’s saliva.
The frequency of food and liquid intake, especially snacks and sugary drinks, must be evaluated, as the consumption of fermentable carbohydrates significantly contributes to the caries process. Bacteria produce acids that feed on fermentable carbohydrates, leading to enamel breakdown.14 In order to promote better oral health, oral hygiene and self-care must be assessed and appropriate instruction provided. The type of toothbrush, amount of fluoride-containing toothpaste used, frequency of brushing and flossing — as well as the use of irrigation devices, fluoride supplements and rinses — should be evaluated for each patient. Previous caries experience of patients, siblings and their caregivers (mainly mothers) must also be considered.14
PREVENTIVE TOOLS AND TREATMENT
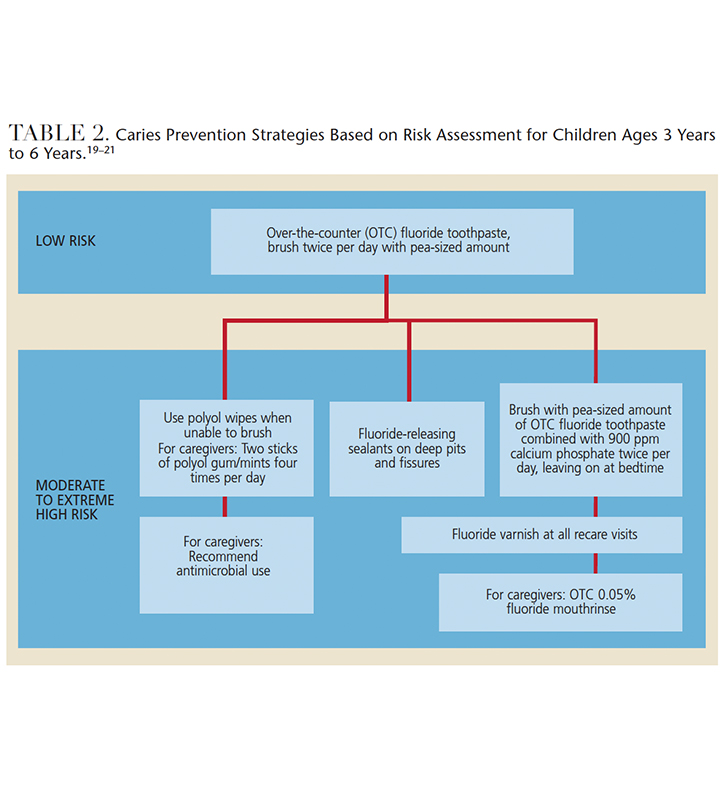
An aggressive preventive approach should be part of routine recare visits for all children — regardless of caries risk status — and may include salivary analysis, diet assessment and patient/parent education. Table 2 provides a description of caries prevention strategies based on risk assessment for children ages 3 to 6.19–21 Dietary analysis and recommendation tools are available through the U.S. Department of Agriculture’s website — choosemyplate.gov — which provides information aimed at health care professionals and consumers.22
Prevention-based office visits include professional prophylaxis, topical fluoride treatment or application of fluoride varnish.23–25 Pit and fissure sealants are also effective approach.26 Sealants can be placed on noncavitated primary and permanent posterior teeth, or early noncavitated lesions on permanent posterior teeth.26 Detecting early minimal caries and placing a sealant over the lesion can inhibit pathogens and arrest lesion progression. This is key in the quest to avoid restorative care.27,28 Research into the use of silver diamine fluoride has shown it to be an effective management tool in arresting certain active caries.29 Resin-infiltration technology is another minimally invasive approach that fills and reinforces demineralized enamel in incipient lesions without the need to reduce tooth structure or provide anesthesia.30 In respect to overall caries management, CAMBRA has been embraced as a key component of minimally invasive dentistry.31
The American Academy of Pediatric Dentistry (AAPD) and International Caries Detection and Assessment System (ICDAS) Foundation have published caries management protocols that embrace CAMBRA.14,32 The AAPD protocols were introduced in 2006 and the ICDAS Foundation’s system was introduced in 2014. Both encourage treatment to be customized for each patient. The AAPD system is divided in three distinct protocols: patients 1–2 years of age, 3–5 years of age, and 6 years and older. The ICDAS Foundation system is known as the International Caries Classification and Management System (ICCMS) and has separate protocols for primary and permanent teeth.
The AAPD system considers patient risk as low moderate or high; in addition, moderate and high classifications are subdivided depending on whether or not a parent/caregiver is involved. Recommendations are based according to risk factors. The ICCMS classification is based on preservation of tooth structure and utilizes four components: history, classification, decision-making and management. Management divides lesions into initial, moderate or extensive categories. Lesions in each category are further subdivided as inactive or active. Recommended treatment protocols are determined according to the size and activity level of lesions. In addition to supporting minimally invasive dentistry, the significance of each of these systems is that they are evidence-based and incorporate multiple factors in establishing an individualized treatment plan.
Preventive therapy for patients outside of professional settings includes the recommendation of gum, hard candies or lozenges containing polyols (such as xylitol or sorbitol) for children older than 5 years. The gum should be chewed for at least 10 minutes following meals. To maximize benefits, a dose of 5 to 8 grams per day divided over two or three doses must be ingested.28 Patients at low to moderate risk of caries should use over-the-counter fluoride rinses at 0.05% concentrations.
Although research shows that use of chlorhexidine-containing products is effective in preventing root caries, they may not significantly reduce coronal caries; consequently, their implementation should be on a case-by-case basis.33 Fluoride supplementation in areas without community water fluoridation should be considered.34 For individuals at high risk of caries, high-dose-fluoride prescription topical pastes or dentifrices may be helpful during self-care routines.34 Recommending products that contain calcium and phosphate technologies to the self-care routine may also help support caries prevention.1,21
CONCLUSION
Substantial evidence-based data demonstrate the efficacy and usefulness of CAMBRA and other caries risk and management protocols in dental practice, yet many clinicians have yet to implement these strategies.14,35 Studies support evidence that CAMBRA is beneficial in shifting the balance of protective and pathological factors that affect caries risk and thus contributes to optimal oral health.
Successful intervention results from clinical consideration of multiple factors and preventive components, rather than implementing any single approach. Rather than simply treating conditions, the multifactorial evidence provided under CAMBRA facilitates the effective management of patients’ oral health. This demonstrates how significantly dentistry has progressed from the “cutting into the tooth for the prevention of disease” philosophy introduced by Hyatt36 nearly 100 years ago.
Undoubtedly, implementation of CAMBRA by more dental practices will lead to significant improvements in the oral health of patients — and thus contribute to positive changes in not only oral health, but quality of life, as well.
REFERENCES
- Featherstone JD. Dental caries: a dynamic disease process. Aust Dent J. 2008;53:286–291.
- U.S. Centers for Disease Control and Prevention. Hygiene-related Diseases: Dental Caries (Tooth Decay). Available at: cdc.gov/healthywater/hygiene/disease/dental_caries.html. Accessed May 31, 2017.
- U.S. Centers for Disease Control and Prevention. Oral Health Improving for Most Americans, But Tooth Decay Among Preschool Children on the Rise: Trends in Oral Health Status: United States, 1988–1994 and 1999–2004. Available at: cdc.gov/nchs/data/series/sr_11/sr11_248.pdf. Accessed May 31, 2017.
- Young DA, Buchanan PM, Lubman RG, Badway NN. New directions in interorganizational collaboration in dentistry: the CAMBRA Coalition model. J Dent Educ. 2007;71:595–600.
- Featherstone JD. The science and practice of caries prevention. J Am Dent Assoc. 2000;131:887–899.
- Cheng J, Chaffee BW, Cheng NF, Featherstone JD. Understanding treatment effect mechanisms of the CAMBRA randomized trial in reducing caries increment. J Dent Res. 2015;94:44–51.
- Zero D, Fontana M, Lennon AM. Clinical applications and outcomes of using indicators of risk in caries management. J Dent Educ. 2001;65:1126–1132.
- Litt MD, Reisine S, Tinanoff N. Multidimensional causal model of dental caries development in low-income preschool children. Public Health Rep. 1995;110:607–617.
- Nicolau B, Marcenes W, Bartley M, Sheiham A. A life course approach to assessing causes of dental caries experience: the relationship between biological, behavioural, socio-economic and psychological conditions and caries in adolescents. Caries Res. 2003;37:319–326.
- Featherstone JD. The caries balance: The basis for caries management by risk assessment. Oral Health Prev Dent. 2004;2(Suppl 1):259–264.
- Vargas CM, Crall JJ, Schneider DA. Sociodemographic distribution of pediatric dental caries: NHANES III, 1988–1994. J Am Dent Assoc. 1998;129:1229–1238.
- Vadiakas G. Case definition, aetiology and risk assessment of early childhood caries (ECC): a revisited review. Eur Arch Paediatr Dent. 2008;9:114–125.
- Alaluusua S, Malmivirta R. Early plaque accumulation — a sign for caries risk in young children. Community Dent Oral Epidemiol. 1994;22:273–276.
- American Academy of Pediatric Dentistry. Guideline on Caries-risk Assessment and Management for Infants, Children, and Adolescents. Available at: aapd.org/media/Policies_Guidelines/G_CariesRiskAssessment.pdf. Accessed May 31, 2017.
- American Dental Association. Caries Risk Assessment Forms. Available at: http://www.ada.org/~/media/ADA/Science%20and%20Research/Files/topic_caries_over6.ashx. Accessed May 31, 2017.
- California Dental Association. Caries Risk Assessment Form. Available at: cda.org/Portals/0/journal/journal_102007.pdf. Accessed May 31,2017.
- Pedersen AM, Bardow A, Jensen SB, Nauntofte B. Saliva and gastrointestinal functions of taste, mastication, swallowing and digestion. Oral Dis. 2002,8:117–129.
- Thenisch NL, Bachmann LM, Imfeld T, Leisebach TM, Steurer J. Are mutans streptococci detected in preschool children a reliable predictive factor for dental caries risk? A systematic review. Caries Res. 2006;40:366–374.
- Jenson L, Budenz AW, Featherstone JD, Ramos-Gomez FJ, Spolsky VW, Young DA. Clinical protocols for caries management by risk assessment. J Calif Dent Assoc. 2007;35:714–723.
- Francisco E, Azevedo S, Young DA. Caries management for the whole family. Dimensions of Dental Hygiene. 2009;7(2):34–37.
- Ramos-Gomez F, Crystal YO, Ng MW, Tinanoff N, Featherstone JD. Caries risk assessment, prevention, and management in pediatric dental care. Gen Dent. 2010;58:505–517.
- U.S. Department of Agriculture. SuperTracker and Other Tools. Available at: choosemyplate.gov/supertracker-tools.html. Accessed May 31, 2017.
- American Dental Association Council on Scientific Affairs. Professionally applied topical fluoride: evidence-based clinical recommendations. J Am Dent Assoc. 2006;137:1151–1159.
- Rozier RG, Adair S, Graham F, et al. Evidence–based clinical recommendations on the prescription of dietary fluoride supplements for caries prevention: a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2010;141:1480–1489.
- Weyant RJ, Tracy SL, Anselmo TT, et al. Topical fluoride for caries prevention: executive summary of the updated clinical recommendations and supporting systematic review. J Am Dent Assoc. 2013;144:1279–1291.
- Wright JT, Tampi MP, Graham L, et al. Sealants for preventing and arresting pit-and-fissure occlusal caries in primary and permanent molars: A systematic review of randomized controlled trials-a report of the American Dental Association and the American Academy of Pediatric Dentistry. J Am Dent Assoc. 2016;147:631–645.e18.
- Griffin SO, Oong E, Kohn W, et al. The effectiveness of sealants in managing caries lesions. J Dent Res. 2008;87:169–174.
- Oong EM, Griffin SO, Kohn WG, Gooch BF, Caufield PW. The effect of dental sealants on bacteria levels in caries lesions: a review of the evidence. J Am Dent Assoc. 2008;139:271–278.
- Milgrom P. Management of patients with active caries. J Calif Dent Assoc. 2014;42:449–453.
- Meyer-Lueckel H, Paris S. Improved resin infiltration of natural caries lesions. J Dent Res. 2008;87:1112–1116.
- Young DA, Buchanan PM, Lubman RG, Badway NN. New directions in interorganizational collaboration in dentistry: The CAMBRA Coalition model. J Dent Educ. 2007;71:595–600.
- ICCMS Guide for Practitioners and Educators. Available at: icdas.org/uploads/ICCMS-Guide_Full_Guide _US.pdf. Accessed May 31, 2017.
- Rethman MP, Beltrán-Aguilar ED, Billings RJ, et al. Nonfluoride caries–preventive agents: executive summary of evidence–based clinical recommendations. J Am Dent Assoc. 2011;142:1065–1071.
- American Academy of Pediatric Dentistry. Guideline on Fluoride Therapy. Available at: aapd.org/media/Policies_Guidelines/G_FluorideTherapy.pdf. Accessed May 31, 2017.
- Ismail AI, Tellez M, Pitts NB, et al. Caries management pathways preserve dental tissues and promote oral health. Community Dent Oral Epidemiol. 2013;41:e12–e40.
- Hyatt TP. Prophylactic odontology — The cutting into the tooth for the preventional of disease. Dent Cosmos. 1922;66:234–241.
FEATURED IMAGE BY LUCKYBUSINESS/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. July 2017;3(7):52–55.

