

Bilateral Multiple Hyperdontia With Nonsyndromic Association
A case report of a nonsyndromal adult with multiple supernumerary teeth in all four quadrants, and only three of 10 supernumerary teeth impacted.
A case report of a nonsyndromal adult with multiple supernumerary teeth in all four quadrants, and only three of 10 supernumerary teeth impacted
Hyperdontia is a developmental abnormality resulting in an increase in the number of teeth that normally occur.1 Multiple supernumerary teeth are not common and usually present as part of a complex syndrome, as this presentation is rare in nonsyndromal patients. The prevalence for nonsyndromal multiple hyperdontia is often reported in patients prior to the third decade of life, with higher predilection in males. Few, if any, of these extra teeth are found erupted. The occurrence of erupted supernumerary teeth occurring in all four quadrants with no syndrome is rare. This case report introduces an adult nonsyndromal female with multiple supernumerary teeth in all four quadrants, with no anterior maxilla supernumerary and only three of 10 supernumerary teeth impacted.
As this case illustrates, unexpected findings of multiple supernumerary teeth require a unique approach to treatment planning and self-care. In addition, a multidisciplinary approach is warranted with late-term therapy. Risk/benefits and patient desires must be carefully evaluated when formulating a treatment plan.
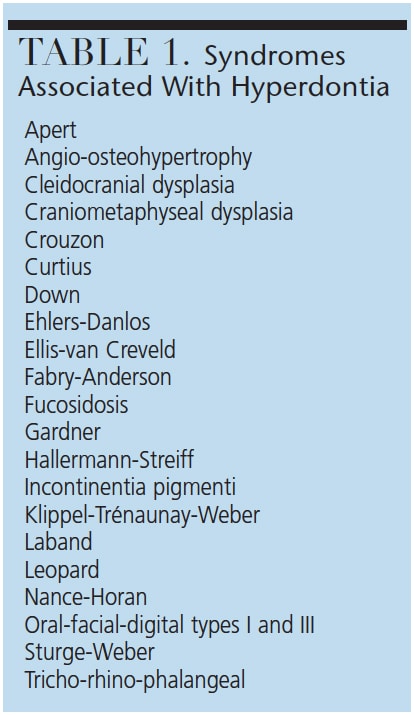 Abnormalities of teeth can be divided into environmental alterations and developmental alterations. Hyperdontia falls under the developmental category. An alteration in tooth number, though somewhat common, occurs when there is a tooth count exceeding the normally occurring dentition of either 20 succedaneous teeth or 32 permanent teeth.2 An extra single tooth is the most common presentation of hyperdontia, representing approximately 76% to 86% of cases, while two teeth represent 12% to 23%, and cases of three or more extra teeth represent less than 1%.1 Multiple supernumerary teeth are not as common, and usually present as part of a complex syndrome — such as those found in Table 1 — that has been linked to this abnormal increase in dentition.1 The extra teeth found in the majority of supernumerary cases are found impacted.3–6 Even rarer is the presence of multiple supernumerary teeth in nonsyndromal patients,4 and those observed appear most often in the premolar region of the mandible.7,8 The prevalence for nonsyndromal multiple hyperdontia (i.e., more than five or more supernumerary teeth9) typically is reported in adolescents and young adults prior to completion of the third decade of life, and includes an overwhelming predilection for males; clinically, most cases reported tend to have few, if any, erupted supernumerary teeth,4,10,11 a finding consistent with reports by Leco-Berrocal et al,2 Rajab and Hamdan,3 Açikgöz et al8 and Esenlik et al.12
Abnormalities of teeth can be divided into environmental alterations and developmental alterations. Hyperdontia falls under the developmental category. An alteration in tooth number, though somewhat common, occurs when there is a tooth count exceeding the normally occurring dentition of either 20 succedaneous teeth or 32 permanent teeth.2 An extra single tooth is the most common presentation of hyperdontia, representing approximately 76% to 86% of cases, while two teeth represent 12% to 23%, and cases of three or more extra teeth represent less than 1%.1 Multiple supernumerary teeth are not as common, and usually present as part of a complex syndrome — such as those found in Table 1 — that has been linked to this abnormal increase in dentition.1 The extra teeth found in the majority of supernumerary cases are found impacted.3–6 Even rarer is the presence of multiple supernumerary teeth in nonsyndromal patients,4 and those observed appear most often in the premolar region of the mandible.7,8 The prevalence for nonsyndromal multiple hyperdontia (i.e., more than five or more supernumerary teeth9) typically is reported in adolescents and young adults prior to completion of the third decade of life, and includes an overwhelming predilection for males; clinically, most cases reported tend to have few, if any, erupted supernumerary teeth,4,10,11 a finding consistent with reports by Leco-Berrocal et al,2 Rajab and Hamdan,3 Açikgöz et al8 and Esenlik et al.12
Supernumerary teeth can occur either unilaterally or bilaterally and sometimes involve both jaws.13 The occurrence of supernumerary teeth in all four quadrants with no syndrome is very uncommon.8,14–16 Although Diaz et al17 reported on a 20-year-old female with 17 supernumerary teeth, unlike the case presented here, severe malocclusion was not present, and there were no other other associated abnormalities. This case report introduces a rare glimpse of a nonsyndromal adult female approaching her fourth decade of life who presented with 10 supernumerary teeth occurring bilaterally in both jaws; additionally, a majority (seven) of the supernumerary teeth were not impacted.
HISTORY AND EXAMination
A 29-year-old Nigerian female presented to Western Kentucky University’s dental hygiene clinic for a routine preventive visit. Her medical history was noncontributory during a review, and only slight vision impairment was noted, which was corrected with the use of contact lenses. In an effort to determine the patient’s risk of periodontal disease and systemic sequelae, she completed a periodontal risk assessment questionnaire.18 Her risk factors included a family history of diabetes and heart disease, and a history of father and siblings who had gingival issues in the past. The patient also affirmed that she had infrequent oral care during previous pregnancies.
Extraoral examination showed the facies and skeletal arrangement presented with good bilateral symmetry and no abnormalities suggestive of a systemic syndrome. No palpable lymph nodes or extraoral lesions were noted. Prior to an intraoral exam, the patient performed a preprocedural rinse with an antimicrobial essential oils mouthwash to reduce the number of oral microorganisms present.19 Intraoral examination of hard tissues revealed 39 teeth clinically visible. No other dental anomalies were found. Family history related to supernumerary teeth was noncontributory. In addition to a full complement of teeth, seven supplemental supernumerary teeth were noted in the clinical exam (Figures 1A through 1C). Angle’s Class II occlusion, a slight open bite, a 2-mm overjet and a 5-mm left shift of midline were noted.
The periodontal classification was determined to be gradual-onset, generalized slight chronic periodontitis, modified by dentition (tooth anatomic factors). Clinical examination revealed no restorations and a large caries lesion on the distal of the upper left second molar, and incipient lesions on the occlusal surfaces of lower-left first and second molars, and lower-right second molar. Panoramic and full-mouth radiographic surveys revealed a lower-left impacted distomolar and lower-right supplemental premolar, and lower-right distomolar (Figure 2 and Figure 3), bringing the number of supernumerary teeth to 10. The patient was noted to have minimal supragingival calculus and generalized heavy subgingival calculus. The visual exam and a disclosing solution revealed only minimal plaque/biofilm accumulation.
TREATMENT PLAN AND OUTCOME
A formalized treatment plan was developed with the goal of improving the health of the periodontium. Intraoral photographs and a full-mouth radiographic series would be used during patient education. A 5-day food diary was given to the patient to evaluate the adequacy of intake of essential food groups. Calculus removal was performed with an ultrasonic scaler, followed by hand scaling and selective polishing. Subsequent tray-delivered 1.23% acidulated-phosphate fluoride completed the patient’s oral hygiene treatment. A follow-up reevaluation was scheduled to assess the periodontal response and discuss the patient’s 5-day food diary. Informed consent was obtained for the sequential oral hygiene treatment plan.
After initial treatment, the patient was scheduled for a periodontal reevaluation in five weeks. A patient hygiene performance20 was conducted prior to instrumentation at each appointment to assess the extent of biofilm, materia alba and debris on tooth surfaces. Based on good oral hygiene findings, the patient was instructed to use a soft-bristled toothbrush and trained on the use of floss holders to aid in flossing.
Five weeks following the completion of periodontal debridement and scaling, the patient returned for periodontal reevaluation. Her medical history and vitals were reassessed and the patient again prerinsed with an antimicrobial rinse. The patient’s periodontal status was reevaluated via visual exam and periodontal probing. Bleeding sites had increased slightly, although probing depths remained relatively unchanged. The patient reported a decrease in bleeding while brushing and flossing. The completed 5-day food diary indicated an inadequate intake of all food groups except for fats and sweets. The patient’s total daily minutes of acid attack were calculated at 52 minutes. She was counseled to decrease the number of fats and sweets, and incorporate more fruits, vegetables, dairy and meats into her diet. In light of her periodontal diagnosis, the patient was placed on a three-month recare visit.

In addition, referrals were made for dental restorations and consultation regarding treatment options for both the impacted and erupted supernumerary teeth. The patient was reticent about any removal of teeth, as they were not causing pain. Her only complaint was that food occasionally wedged in between the extra teeth; thus, she declined further investigation of treatment options. In light of recent studies regarding autosomal dominant transmission and familial occurrence of supernumerary teeth,21–23 the patient was counseled to have her children evaluated at the earliest date for delayed eruption patterns and to rule out the presence of supernumerary teeth.
The patient returned for follow-up in six months rather than recommended three-month visit, and failed to follow through with any recommended referrals. Her periodontal health showed little change and personal hygiene performance20 was found to be fair. A power toothbrush was recommended. The referrals regarding restorative care and supernumerary teeth were reiterated. Unwanted related sequelae, such as abscesses, chronic periodontitis and dentigerous cysts related to supernumerary teeth (both erupted and impacted),1 were also emphasized.

DISCUSSION
Although variations such as an increase in the normal numerical complement of teeth are common, it is rare to find multiple supernumerary teeth that are not associated with a complex syndrome.3,4,7 Yagüe-García et al4 suggested that supernumerary teeth with no other dental anomalies “should be regarded as a distinct pathological entity.”
Supernumerary teeth can be divided into supplemental (eumorphic or toothlike) or rudimentary (dysmorphic or having abnormal shape and size) types, with the latter group being divided further into conical, tuberculated and molariform types.1 Approximately 76% to 86% of cases represent single tooth hyperdontia.1 The mesiodens (or palatodens, as suggested by Yoon et al24) located in the anterior maxillary midline area account for the majority of these single-tooth hyperdontia cases (reportedly, up to 80%, according to Leco-Berrocal et al2). In contrast, nonsyndromal multiple hyperdontia has a predilection for the premolar region of the mandible.7,8 Consistent with findings of Yusof7 and Açikgöz et al,8 this case had the majority of its supernumerary teeth located in the mandibular premolar region.
The exact etiology of supernumerary teeth is unclear; however, localized and independent hyperactivity of the dental lamina is the most widely accepted theory, according to Neville et al.1 Several studies seem to indicate a definitive genetic relationship with the origin of supernumerary teeth.11,21–23,25 A distinguishing feature of this case is that it does not fall in line with most of the commonly occurring observations of multiple hyperdontia. This case involves a nonadolescent female with no associated complex syndrome who presented with multiple supernumerary teeth in all four quadrants. There was no anterior maxilla involvement and only three of 10 supernumerary teeth were impacted. Additionally, there was no occurrence in family history, no complaint of pain, and no severe malocclusion-related issues.
Treatment options for multiple supernumerary teeth are varied, and include observation or extraction, depending on whether they are erupted or impacted, and whether or not they have additional clinical issues. When patients present with multiple supernumerary teeth, clinicians inherently face a variety of clinical issues. Crowding, malocclusion and periodontitis are associated with erupted supernumerary teeth, whereas delayed eruption, resorption of adjacent teeth, odontogenic cysts, and displacement of teeth often accompany the impacted variety.17,22,26
Treatment for erupted teeth lends itself to a multidisciplinary approach. These treatment regimens include, but are not limited to, oral and maxillofacial surgery, orthodontics and periodontal intervention — especially with treatment in later decades of life. Appropriate radiographic technique, and possibly even cone beam computed tomography for exact localization regarding any surgical approach, is essential.27

CONCLUSION
As noted at the outset, it is rare to find multiple supernumeraries that are not associated with a complex syndrome. When they are found, they tend to occur in males more than females, and tend to be found impacted. Most case reports are in adolescents and young adults. As Yagüe-García et al4 note, the prevalence of multiple hyperdontia (comprising five or more teeth) appears to be the least common presentation. Multiple supernumerary teeth affecting all four quadrants (as detailed in this case report) are extremely rare.15,16
Overall management requires practitioners to consider multidisciplinary care, including orthodontic, periodontal and surgical teams working closely to achieve optimal outcomes. Treatment planning should weigh the risks and benefits of observation versus a surgical approach. Untoward related sequelae, such as the occurrence of gingivitis, periodontitis, abscess formation and possible development of various odontogenic cysts and tumors,1 need to be addressed with the patient. Finally, radiographic surveillance is appropriate because unexpected problems related to supernumerary teeth — such as the formation of new supernumerary teeth —have been known to develop over time.14,26,28
KEY TAKEAWAYS
- Clinicians inherently face a variety of clinical issues when patients present with multiple supernumerary teeth.
- Consequently, findings of multiple supernumerary teeth require a unique approach to treatment planning and self-care recommendations.
- Multiple supernumerary teeth usually present as part of a complex syndrome that has been linked to this abnormal increase in dentition.1
- Clinically, most cases reported tend to have few, if any, erupted supernumerary teeth.4,10,11
- Nonsyndromal multiple hyperdontia has a predilection for the premolar region of the mandible.7,8
- Supernumerary teeth can occur either unilaterally or bilaterally and sometimes involve both jaws.13
- The exact etiology of supernumerary teeth is unclear; however, localized and independent hyperactivity of the dental lamina is the most widely accepted theory.1
- Treatment options for multiple supernumerary teeth are varied, and include observation or extraction, depending on whether they are erupted or impacted, and whether or not the teeth have additional clinical issues.
References
- Neville B, Damm D, Allen C, Bouquot J. Oral and Maxillofacial Pathology. 3rd ed. St. Louis, Mo: Elsevier; 2008:77–82.
- Leco-Berrocal MI, Martín-Morales JF, Martínez-González JM. An observational study of the frequency of supernumerary teeth in a population of 2000 patients. Med Oral Patol Oral Cir Bucal. 2007; 12:E134–E138.
- Rajab LD, Hamdan MA. Supernumerary teeth: review of the literature and a survey of 152 cases. Int J Paediatr Dent. 2002;12:244–254.
- Yagüe-García J, Berini-Aytés L, Gay-Escoda C. Multiple supernumerary teeth not associated with complex syndromes: a retrospective study. Med Oral Patol Oral Cir Bucal. 2009;14:E331–E336.
- Celikoglu M, Kamak H, Oktay H. Prevalence and characteristics of supernumerary teeth in a non-syndrome Turkish population: associated pathologies and proposed treatment. Med Oral Patol Oral Cir Bucal. 2010;15:E575–E578.
- Nazif MM, Ruffalo RC, Zullo T. Impacted supernumerary teeth: a survey of 50 cases. J Am Dent Assoc. 1983;106:201–204.
- Yusof WZ. Non-syndrome associated multiple supernumerary teeth: literature review. J Can Dent Assoc. 1990;56:147–149.
- Açikgöz A, Açikgöz G, Tunga U, Otan F. Characteristics and prevalence of non-syndrome multiple supernumerary teeth: a retrospective study. Dentomaxillofac Radiol. 2006;35:185–190.
- Gündüz K, Muğlali M. Non-syndrome multiple supernumerary teeth: a case report. J Contemp Dent Pract. 2007;8:81–87.
- Santos AP, Ammari MA, Moliterno LF. First report of bilateral supernumerary teeth associated with both primary and permanent maxillary canines. J Oral Sci. 2009;51:145–150.
- Umweni AA, Osunbor GE. Non-syndrome multiple supernumerary teeth in Nigerians. Odontostomatol Trop. 2002;25:43–48.
- Esenlik E, Sayin MO, Atilla AO, Ozen T, Altun C, Başak F. Supernumerary teeth in a Turkish population. Am J Orthod Dentofacial Orthop. 2009;136:848–852.
- Sood PB, Patil B, Godhi S, Shetty DC. Multiple supernumerary teeth and odontoma in the maxilla: a case report. Contemp Clin Dent. 2010;1:45–46.
- Anegundi RT, Tavargeri A, Indushekar KR, Sudha P. Sequential development of multiple supplemental premolars. Four-year follow-up report. NY State Dent J. 2008;74:46–49.
- Ramsaran AS, Barclay S, Scipio E, Ogunsalu C. Non-syndromal multiple buried supernumerary teeth: report of two cases from the English-speaking Caribbean and a review of the literature. West Indian Med J. 2005;54:334–336.
- Refoua Y, Arshad M. An unusual case of bilateral maxillary and mandibular supernumerary teeth. J Dent. 2006;3:140–142.
- Diaz A, Orozco J, Fonseca M. Multiple hyperodontia: report of a case with 17 supernumerary teeth with nonsyndromic association. Med Oral Patol Oral Cir Bucal. 2009;14:E229–E231.
- Schutte DW, Donley TG: Determining periodontal risk factors in patients presenting for dental care. J Dental Hyg.1996;70:230–234.
- Miller CH, Palenik DJ. Aseptic Techniques. In: Miller CH, Palenik DJ, eds. Infection Control and Management of Hazardous Materials for the Dental Team. 4th ed. St. Louis, Mo: Mosby; 2010:201–206.
- Podshadley AG, Haley JV. A method for evaluating oral hygiene performance. Public Health Rep. 1968;83:259–264.
- Batra P, Duggal R, Parkash H. Non-syndromic multiple supernumerary teeth transmitted as an autosomal dominant trait. J Oral Pathol Med. 2005; 34:621–625.
- Orhan AI, Özer L, Orhan K. Familial occurrence of nonsyndromal multiple supernumerary teeth. A rare condition. Angle Orthod. 2006;76:891–897.
- Wang XX, Zhang J, Wei FC. Autosomal dominant inherence of multiple supernumerary teeth. Int J Oral Maxillofac Surg. 2007;36:756–758.
- Yoon RK, Chussid S, Davis MJ. Impacted maxillary anterior supernumerary teeth: a survey of forty-two cases. NY State Dent J. 2008;74:24–27.
- Van der Merwe AE, Steyn M. A report on the high incidence of supernumerary teeth in skeletal remains from a 19th century mining community from Kimberley, South Africa. SADJ. 2009;64:162,164–166.
- Mason C, Rule DC, Hopper C. Multiple supernumeraries: the importance of clinical and radiographic follow-up. Dentomaxillofac Radiol. 1996;25:109–113.
- Brauer HU. Case report: non-syndromic multiple supernumerary teeth localized by cone beam computed tomography. Eur Arch Paediatr Dent. 2010;11:41–43.
- Cochrane SM, Clark JR, Hunt NP. Late developing supernumerary teeth in the mandible. Br J Orthod. 1997;24:293–296.
Featured image by СЕРГЕЙ ВАСИЛЬКОВ/WIKIMEDIA.ORG
From Decisions in Dentistry. March 2018;4(3):25-28,31.
