

Analysis of the Two-Stage Injection Technique
The evidence supporting this approach to minimizing pain during local anesthesia administration is limited.
The evidence supporting this approach to minimizing pain during local anesthesia administration is limited
PURCHASE COURSE
This course was published in the December 2016 issue and expires December 2019.The author has no commercial conflicts of interest to disclose.This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Define the two-stage injection technique.
- Identify the characteristics of local anesthetics.
- Discuss the available evidence on the efficacy of the two-stage injection technique.
One of the most important aspects of dental practice is to ensure patients are free from pain during therapy. Because of this, numerous techniques, agents and equipment have been introduced to improve the patient and clinician experience with local anesthetic administration. Individual dental practices often use a unique blend of methodology, anesthetics and devices when administering local anesthesia. These approaches are typically based on differences in patient populations, clinician gender, practice location, provider and staff training, and business operations.1–3 This article presents an analysis of the two-stage injection technique that is designed to minimize pain associated with local anesthesia administration.
When pain is experienced, the central nervous system detects and processes tissue damage and/or bodily danger (with the goal of removing the body from harm).4 Generally, type A and type C nerve fibers are involved during the dental injection process. The type A nerve fibers respond to mechanical stimulation and relay the sensation of pain described as sharp or vivid, while type C nerve fibers respond to thermal or chemical stimuli and are associated with dull or burning sensations.5 The process of local anesthetic injection and nerve fiber activation includes the needle penetrating mucosa and advancing to the target area (type A); anesthetic deposition (type A and type C); and removal of the needle (type A and type C).4
Introduction of the needle into the mucosa is the first step of the injection pain experience. Previous analysis of pain perception during this stage demonstrated a 14% to 22% incidence of moderate to severe pain with standard injection protocols. 6 Considered the more painful stage of an anesthetic injection, the deposition of solution elicits intense responses due to the expansion of tissue, the rich sensory innervation seen intraorally, and the chemical complexion and pH of the local anesthetic.4 Pain analyses for anesthetic deposition found an 18% to 56% incidence of moderate to severe pain during the anesthetic deposition stage.7–10 Additionally, needle withdrawal can be associated with postoperative pain due to tissue damage or an expedited removal of the anesthetic delivery device.4 Postoperative pain has also been associated with the pH of the anesthetic, multiple injections, inadequate needle design, and poor injection technique.4,11–13
ISTOCK.COM/ JAKE OLIMB AND JON FRAZE
TWO-STAGE INJECTION TECHNIQUE
Because injection technique is part of patients’ evaluation of care, oral health professionals are advised to deliver the least painful injection possible.4,14 This led Levine to propose the “one-two injection” (or two-stage injection) technique in 1968, using two stages of anesthetic deposition to reduce pain. The first deposition is shallow, and the second is directed at the targeted area.15 More recently, Walton and Torabinejad16 suggested the technique may decrease injection pain for any operative dental encounter, with specific indications for apprehensive or anxious patients.
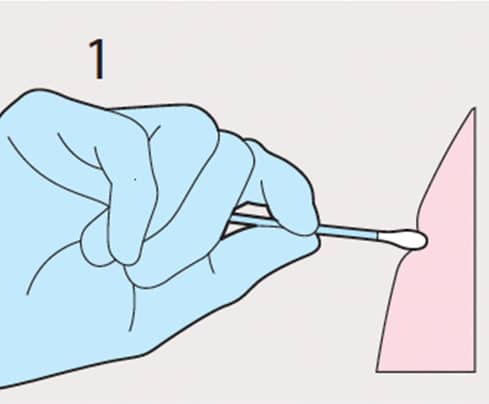
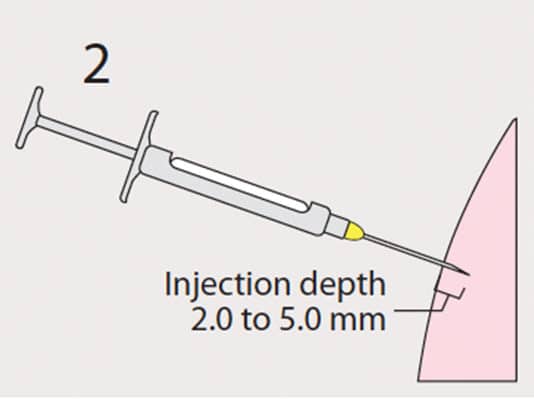
The first step in the two-stage injection technique is to prepare the mucosa by thoroughly drying the area (using gauze and air) and applying a topical anesthetic gel (Figure 1). The next step is to introduce the needle into the mucosa at a depth of 2.0 to 5.0 mm, depositing 0.3 to 0.5 ml of anesthetic (Figure 2). After waiting five to 10 minutes (Figure 3), the delivery device is reintroduced at the previous puncture zone (Figure 4), advanced slowly to the target area for completed anesthetic deposition, and withdrawn.
Although it can be applied at several injection sites, the two-stage injection technique is most often used with inferior alveolar nerve blocks (IANB). Compared to the traditional Halstead method, anecdotal reports suggest the two-stage injection technique is a superior alternative for IANB. These reports propose the two-stage injection technique as a solution to the unreliable effect of topical anesthetic for IANB injections. Nakanishi et al,17 Meechan et al,18 and Nusstein et al,6,10 reported that benzocaine (20%) topical gel did not consistently reduce the pain of needle-mucosa penetration with IANB injections. While current evidence points to an unreliability of topical benzocaine anesthetic for IANB injections, some reports have found a psychological connection with topical anesthetics as it relates to reducing the expectation of pain and a belief the clinician is doing everything possible to minimize pain.10,19
Clinical studies evaluating the success of the two-stage injection technique to reduce pain are limited. Nusstein, Steinkruger et al10 did not find a difference in pain between men and women when employing the twostage injection technique for IANB needle insertion or fluid deposition using 2.2 ml of 2% lidocaine with 1:100,000 epinephrine. The investigators reported a difference, however, in the pain response (less discomfort with the two-stage injection technique) during needle placement (advancing the needle through the mucosa) for women. In another study
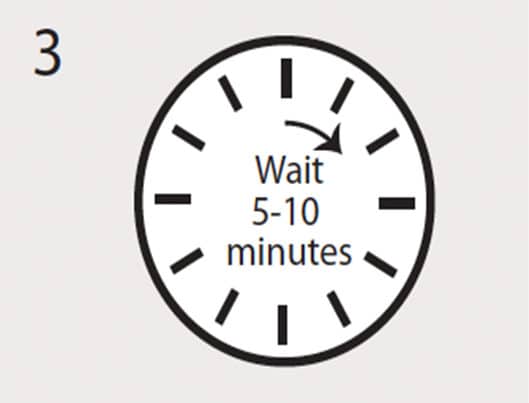
Photo courtesy of JON FRAZE
using 2% lidocaine with 1:100,000 epinephrine to evaluate the patient pain experience, the investigators did not find that two-stage deposition of 0.2 to 0.4 ml significantly reduced the pain experience during needle placement for men or women.20 Sandeep et al21 found the two-stage injection technique with 2.5 ml 2% lidocaine with 1:80,000 epinephrine produced a lower pain response from children when anesthetic administration included infiltration or IANB injections. The authors also provided a modification to the technique described as the minimal deposition of anesthetic agent ahead of needle advancement and placement. Additional research is needed to validate the two-stage injection technique and reach professional consensus.
ANESTHETIC SELECTION
Anesthetic selection for the two-stage injection technique depends on provider preference and patient characteristics. The technique is often associated with 4% prilocaine plain as the primary agent used for the shallow injection, followed by lidocaine or articaine for the target site anesthetic deposition.22
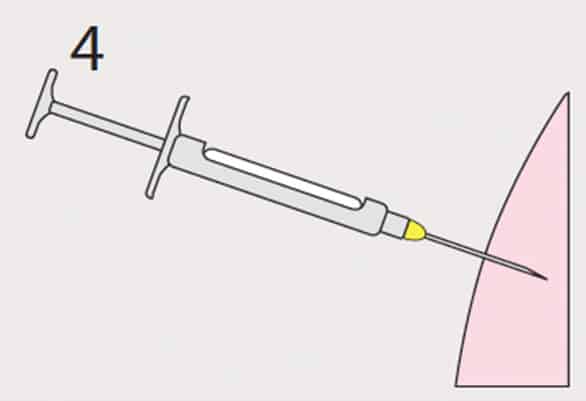
Photo courtesy of JON FRAZE
Local anesthetics vary in their characteristics and effects. The use of 4% prilocaine plain is proposed as the primary agent for the two-stage injection technique due to the solution’s pH value of 6.0 to 7.0.23 Several authors have proposed that the more acidic the anesthetic solution, the more likely a patient will report a higher pain score.24–26 Anesthetics with vasoconstrictors have a lower pH value (3.0 to 5.0), while 4% prilocaine plain possesses the highest pH value (6.0 to 7.0), followed by 3% mepivacaine plain (4.5 to 6.8).26
In an analysis of pain response and anesthetic administration, Nydegger27 did not report any statistical difference between epinephrine- containing anesthetics and needle insertion pain across both genders (4% articaine with 1:100,000 epinephrine, 4% prilocaine with 1:200,000 epinephrine, and 4% lidocaine with 1:100,000 epinephrine). Of the study subjects, 86.1% reported no-to-mild (NM) pain for all anesthetics, and 13.9% reported moderate-to-severe pain (MS) with needle insertion. Additionally, the analysis did not find significant pain reporting difference with needle placement (84.5% NM/15.5% MS) or deposition of anesthetic (women 60% NM/40% MS; and men 81.1% NM/18.9% MS) between the agents used. Abdulwahab et al28 evaluated anesthetics and pain response with mandibular buccal infiltration for six local anesthetic formulations. Pain at the injection site was evaluated using the Visual Analog Scale for Pain (VAS Pain), and a mean measurement was used to assess pain perception. All anesthetics demonstrated a mean VAS Pain score that correlated with mild pain response: 0.5% bupivacaine with 1:200,000 epinephrine (32.2 mm of VAS Pain 100 mm); 2% lidocaine with 1:100,000 epinephrine (26.2 mm); 4% articaine with 1:100,000 epinephrine (24.1 mm); 4% articaine with 1:200,000 epinephrine (24.1 mm); 3% mepivacaine, plain (22.9 mm); and 4% prilocaine with 1:200,000 epinephrine (21 mm).
Specific to analysis of 4% prilocaine plain and injection pain, Wahl, Schmitt, et al29 found that 4% prilocaine plain caused significantly less pain than bupivacaine for maxillary buccal infiltration, posterior palatal infiltration and IANB injections. In an earlier study that compared 2% lidocaine with 1:100,000 epinephrine and 4% prilocaine plain and pain reporting, Wahl, Overton, et al30 did not find a statistically significant difference between the two agents and injection pain reported during maxillary buccal infiltration or inferior alveolar injections. Kramp et al31 demonstrated that administration of 4% prilocaine plain resulted in the least perceived pain when compared to 2% mepivacaine with 1:20,000 levonordefrin and 2% lidocaine with 1:100,000 epinephrine. In a 2005 study, the investigators reported that use of 4% prilocaine plain resulted in significantly lower pain scores than 2% lidocaine with 1:100,000 epinephrine, 3% mepivacaine plain, and 4% articaine, with 1:100,000 epinephrine.32
TECHNIQUE CONSIDERATIONS
Many variables affect the success of the two-stage injection technique. Anesthetic selection should be a controllable variable, but conclusive information on the best agent(s) is limited. Twenty-four studies were evaluated for this article. The majority (17 of 24 studies or 70.8%) found no significant difference between the anesthetics tested. Out of 17 studies that investigated different anesthetics with vasoconstrictors, 13 papers (76.5%) found no significant differences between the agents. Three of 14 studies (21.4%) that evaluated lidocaine found 2% lidocaine with 1:100,000 epinephrine elicited the least discomfort of the agents compared, while three of five analyses (60%) involving 4% prilocaine plain determined that agent provided the least painful experience during injection. In one study comparing 2% lidocaine with 1:80,000 epinephrine and 4% articaine with 1:100,000 epinephrine, articaine was found to produce the least pain response.33 Additionally, some correlation was observed with vasoconstrictor presence and higher discomfort. The completion of a comprehensive meta-analysis is needed to evaluate these observations and expand the evidence base for best practice.
Differences between pain response and gender have been proposed. Studies found that women reported more pain than men for many injection types, especially during needle advancement.10,27,34,35 A patient population with increased pain response will require a higher level of pain and anxiety management, as well as augmented techniques to provide the least painful encounter possible. Providers will need to evaluate the possible patient response to a second injection and address any concerns or fears the individual may have. If a patient is needle phobic, alternative methods should be considered, such as profound topical anesthetic agents, needleless syringes, anxiety/behavior management or sedation.
Additionally, some reports have shown the location of the injection site may be associated with higher pain perception (periodontal ligament and maxillary infiltrations are usually reported as less painful than IANB and palatal injections).36–38 Other considerations with the two-stage injection technique include the presence of dental and/or needle phobias, a patient’s ability to cooperate, and his or her medical and dental history. Every oral health professional needs to understand the risks, benefits, recommendations and regulations with the anesthetic agents and anesthesia techniques used in dental care.39
Unfortunately, the available science supporting the two-stage injection technique, as well as the best anesthetic agents and pain response, is limited. VAS Pain scoring with anesthetic agent comparisons is usually a secondary finding, if evaluated. There are also too few studies and reviews to achieve professional consensus on the benefits, risks and best practices of the two-stage injection technique. In addition, no studies were found that evaluated within one cohort all anesthetics available in the United States.
CONCLUSION
While the majority of dental patients report mild to no pain during dental injections, a significant percentage finds the process to be moderately to severely painful. Used in dentistry for more than 45 years, the two-stage injection technique has been proposed to reduce the pain response to local anesthetic injections. Although anecdotal reports and dental professional opinions represent a favorable view of the technique, the evidence base to validate the methodology is fragmented. While many oral health professionals favor this technique, there is currently a lack of professional consensus as to best practices for the two-stage injection technique
REFERENCES
- Riley JL, Gordan VV, Rouisse KM, McClelland J, Gilbert GH. Dental Practice- Based Research Network Collaborative Group. Differences in male and female dentists’ practice patterns regarding diagnosis and treatment of dental caries: findings from the Dental Practice-Based Research Network. J Am Dent Assoc. 2011;142:429–440.
- Bader JD, Shugars DA. Variation in dentists’ clinical decisions. J Public Health Dent. 1995;55:181–188.
- Correa MB, Peres MA, Peres KG, Horta BL, Barros AJ, Demarco FF. Do socioeconomic determinants affect the quality of posterior dental restorations? A multilevel approach. J Dent. 2013;41:960–967.
- Boynes SG. Evaluating the advances and use of hypodermic needles in dentistry. Compendium. 2014;35:649–654.
- Dionne RA, Phero J, Becker DG. Management of Pain and Anxiety in the Dental Office. Philadelphia: WB Saunders; 2002.
- Nusstein JM, Beck M. Effectiveness of 20% benzocaine as a topical anesthetic for intraoral injections. Anesth Prog. 2003;50:159–163.
- Nist R, Reader A, Beck M, Meyers W. An evaluation of the incisive nerve block and combination inferior alveolar and incisive nerve blocks in mandibular anesthesia. J Endod. 1992;18:455–459.
- Ridenour S, Reader A, Beck M, Weaver J. Anesthetic efficacy of a combination of hyaluronidase and lidocaine with epinephrine in inferior alveolar nerve blocks. Anesth Prog. 2001;48:9–15.
- Mikesell P, Nusstein J, Reader A, Beck M, Weaver J. A comparison of articaine and lidocaine for inferior alveolar nerve blocks. J Endod. 2005;31:265–270.
- Nusstein J, Steinkruger G, Reader A, Beck M, Weaver J. The effects of a 2-stage injection technique on inferior alveolar nerve block injection pain. Anesth Prog. 2006;53:126–130.
- Kaufman E, Epstein JB, Naveh E. A survey of pain, pressure and discomfort induced by commonly used oral local anesthetic injections. Anesth Prog. 2005;52:122–127.
- Oikarinen VJ, Ylipaavalniemi P, Evers H. Pain and temperature sensations related to local anesthesia. Int J Oral Surg. 1975;4:151–156.
- Malamed SF. Handbook of Local Anesthesia. 6th ed. St. Louis: Elsevier Mosby; 2012.
- De St Georges J. How dentists are judged by patients. Dent Today. 2004;23:96–98.
- Levine AH. Preventing pain: the onetwo injection. TIC. 1968;27:6–9.
- Walton RE, Torabinejad M. Principles and Practice of Endodontics. 3rd ed. Philadelphia: WB Saunders Co; 2002:102.
- Nakanishi O, Haas D, Ishikawa T, Kameyama S, Nishi M. Efficacy of mandibular topical anesthesia varies with the site of administration. Anesth Prog. 1996;43:14–19.
- Meechan JG, Gowans A, Wellbury R. The use of patient controlled transcutaneous electronic nerve stimulation (TENS) to decrease the discomfort of regional anesthesia in dentistry: a randomized controlled clinical trial. J Dent. 1998;26:417–420.
- Martin MD, Ramsay D, Whitney C, Fiset L, Weinstein P. Topical anesthesia: differentiating the pharmacological and psychological contributions to efficacy. Anesth Prog. 1994;41:40–47.
- McCartney M, Reader A, Beck M. Injection pain of the inferior alveolar nerve block in patients with irreversible pulpitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104:571–575.
- Sandeep V, Kumar M, Jyostna P, Duggi V. Evaluation of 2-stage injection technique in children. Anesth Prog. 2016;63:3-7.
- Bernstein J. Give your patients a wow experience — don’t hurt them! Dental Economics. 2015;105:12.
- Bassett K, DiMarco A, Naughton D. Local Anesthesia for Dental Professionals. 2nd ed. St. Louis: Pearson; 2014.
- Frank SG, Lalonde DH. How acidic is the lidocaine we are injecting, and how much bicarbonate should we add? Can J Plast Surg. 2012;20:71–73.
- Whitcomb M, Drum M, Reader A, Nusstein J, Beck M. A prospective, randomized, double-blind study of the anesthetic efficacy of sodium bicarbonate buffered 2% lidocaine with 1:100,000 epinephrine in inferior alveolar nerve blocks. Anesth Prog. 2010;57:59–66.
- Goodchild JH, Donaldson M. Comparing the pH change of local anesthetic solutions using two chairside buffering techniques. Compendium. 2016;37:e6.
- Nydegger BJ. Anesthetic efficacy of 4% articaine with 1:100,000 epinephrine, 4% prilocaine with 1:200,000 epinephrine, and 4% lidocaine with 1:100,000 epinephrine as a primary buccal infiltration of the mandibular first molar. Doctoral Dissertation. The Ohio State University, 2013.
- Abdulwahab M, Boynes S, Moore P, et al. The efficacy of six local anesthetic formulations used for posterior mandibular buccal infiltration anesthesia. J Am Dent Assoc. 2009;140:1018–1024.
- Wahl MJ, Schmitt MM, Overton DA, Gordon MK. Injection pain of bupivacaine with epinephrine vs. prilocaine plain. J Am Dent Assoc. 2002;133:1652–1656.
- Wahl MJ, Overton D, Howell J, Siegel E, Schmitt MM, Muldoon M. Pain on injection of prilocaine plain vs. lidocaine with epinephrine: a prospective doubleblind study. J Am Dent Assoc. 2001;132:1396–1401.
- Kramp LF, Eleazer PD, Scheetz JP. Evaluation of prilocaine for the reduction of pain associated with transmucosal anesthetic administration. Anesth Prog. 1999;46:52.
- Wahl MJ, Schmitt MM, Overton DA. Injection pain of prilocaine plain, mepivacaine plain, articaine with epinephrine, and lidocaine with epinephrine. Gen Dent. 2005;54:168–171.
- Kanaa MD, Whitworth JM, Meechan JG. A comparison of the efficacy of 4% articaine with 1:100,000 epinephrine and 2% lidocaine with 1:80,000 epinephrine in achieving pulpal anesthesia in maxillary teeth with irreversible pulpitis. J Endod. 2012;38:279–282.
- Pabst L, Nusstein J, Drum M, Reader A, Beck M. The efficacy of a repeated buccal infiltration of articaine in prolonging duration of pulpal anesthesia in the mandibular first molar. Anesth Prog. 2009;56:128–34.
- Otto MW, Dougher MJ. Sex differences and personality factors in responsivity to pain. Percept Mot Skills. 1985;61:383–390.
- Marin MK. Intraseptal anesthesia in the general dental practice. Compendium. 1987;8:202–209.
- Mansour MS, Adawy AM. The periodontal ligament injection. Egyp Dent J. 1985;31:109–119.
- Kaufman E, Epstein JB, Naveh E, Gorsky M, Gross A, Cohen G. A survey of pain, pressure, and discomfort induced by commonly used oral local anesthesia injections. Anesth Prog. 2005;52:122–127.
- Boynes SG. Dental Anesthesiology: The Rules and Regulations of the United States. 5th ed. Chicago: No-No Orchard Publications; 2013.
Featured image courtesy of OCSKAYMARK/ISTOCK/ THINKSTOCK
From Decisions in Dentistry. December 2016;2(12):46-49.

