

Addiction and Oral Health Care
Dental providers should be knowledgeable about commonly misused drugs and the oral consequences of substance abuse.
Dental providers should be knowledgeable about commonly misused drugs and the oral consequences of substance abuse.
PURCHASE COURSE
This course was published in the January 2018 issue and expires January 2021. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
Substance misuse and abuse are serious problems in the United States. In 2015, more than 27 million American reported being current users of illicit drugs or having misused prescription drugs.1 The misuse of a drug occurs when it is used for purposes for which it was not intended, or it is used in excessive amounts. Substance misuse and abuse costs Americans approximately $442 billion annually in crime, health issues and lost productivity.1
This course was published in the January 2018 issue and expires January 2021. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
- Explain the extent and approximate costs of the substance abuse problem in the United States.
- Describe the signs of substance abuse, and the prevailing theory of addiction.
- List common oral health risks and manifestations of substance abuse, and strategies for treating this patient population.
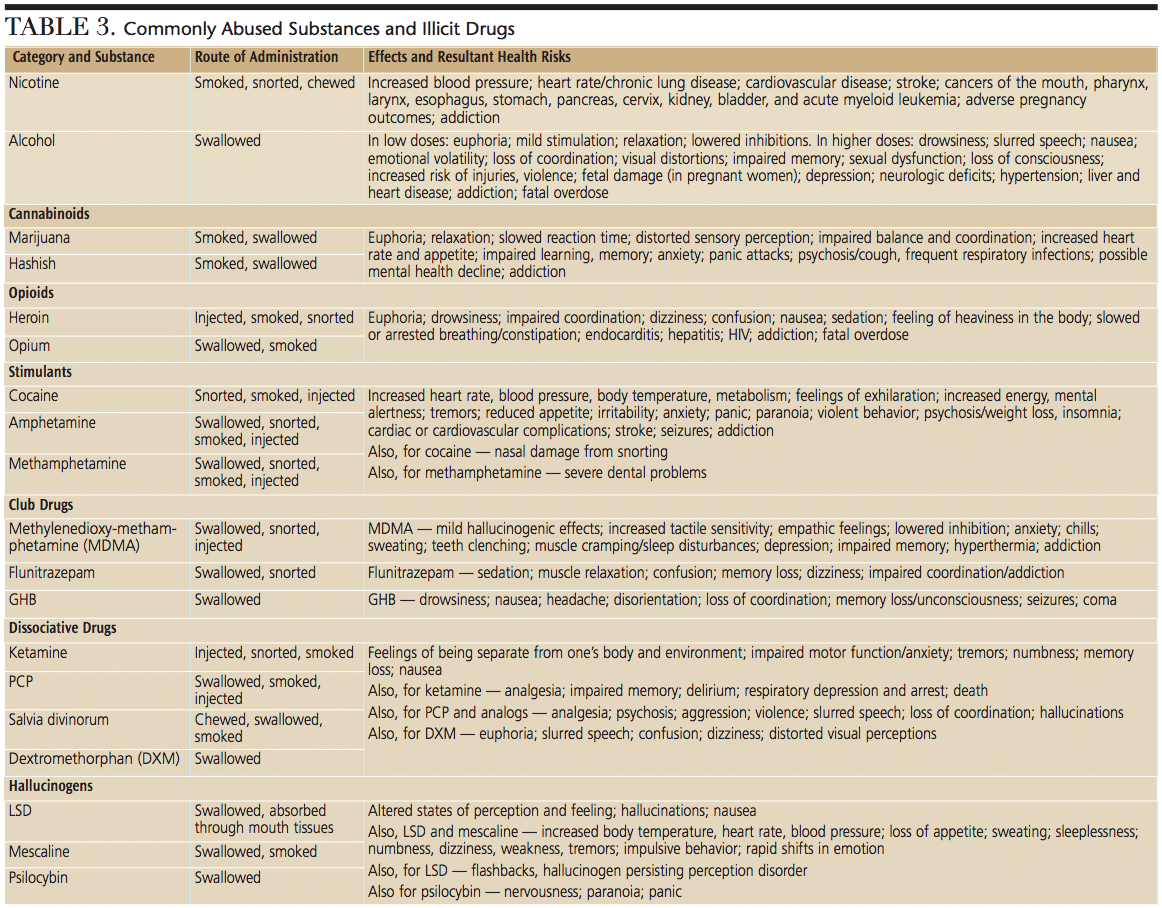
Substance abuse is using any psychoactive compound with the potential to cause health and social problems.1 Drugs of abuse include marijuana, hashish, cocaine (including crack), heroin, hallucinogens, inhalants, or prescription-type psychotherapeutics (e.g., pain relievers, tranquilizers, stimulants and sedatives used for nonmedical reasons). The most severe manifestation of substance abuse disorders is known as addiction.
It is important to note that simply misusing a substance does not mean that someone has a substance use disorder. Substance misuse, however, can put the user and individuals around them at risk of harm. Risk factors include early initiation to substance misuse and the misuse of multiple substances.1 Substance misuse, and substance use disorders are associated with a variety of negative consequences, including deteriorating relationships, poor school performance, loss of employment, diminished mental health, and increases in sickness and death (e.g., motor vehicle crashes, poisoning, violence or accidents).1 No single risk factor can predict an individual’s likelihood of abusing substances or becoming addicted. Addictive substances produce feelings of pleasure, and these feelings increase the likelihood of repeated substance abuse.1
The most widely accepted theory of addiction is the disease model, which defines drug addiction as a brain disease over which the individual has no control.2–4 Some psychoactive drugs (including marijuana, cocaine and methamphetamines) change the structures and/or functions of the brain.3,4 It is important to remember, however, that in addition to illicit drugs, abuse also occurs with legal drugs, such as alcohol, nicotine and prescription medications.
Recently, there has been increased attention on the opioid addiction crisis. Of the 52,404 U.S. deaths attributed to drug overdoses in 2015, 63.1% involved the use of an opioid.5 In addition, approximately half of all opioid-related deaths involve the use of a prescription opioid. In 2015, 2 million Americans were addicted to a prescription opioid.5 Besides the morbidity and mortality associated with opioid abuse, there are significant financial costs in terms of health care and lost productivity.
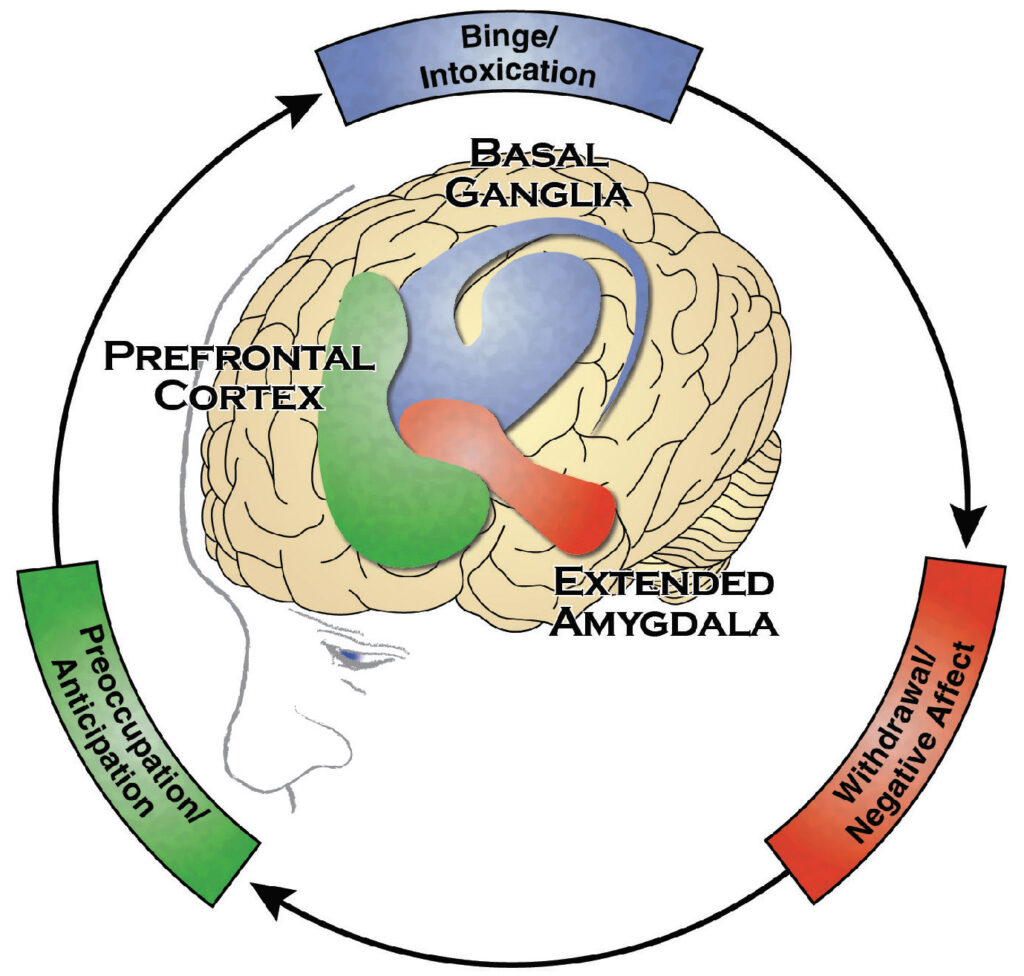
Addictive drugs directly or indirectly activate the brain’s reward system by markedly increasing the release of dopamine, which is a neurotransmitter that regulates emotion, cognition, movement, motivation and pleasure.1 Overstimulation of the brain’s reward pathway with dopamine produces intense euphoric effects and sensations that are further reinforced or strengthened by continued drug use.3,4,6 Figure 1 illustrates the areas of the brain impacted by addiction, and long-term substance abuse can cause brain dysfunction.1
SIGNS AND SYMPTOMS

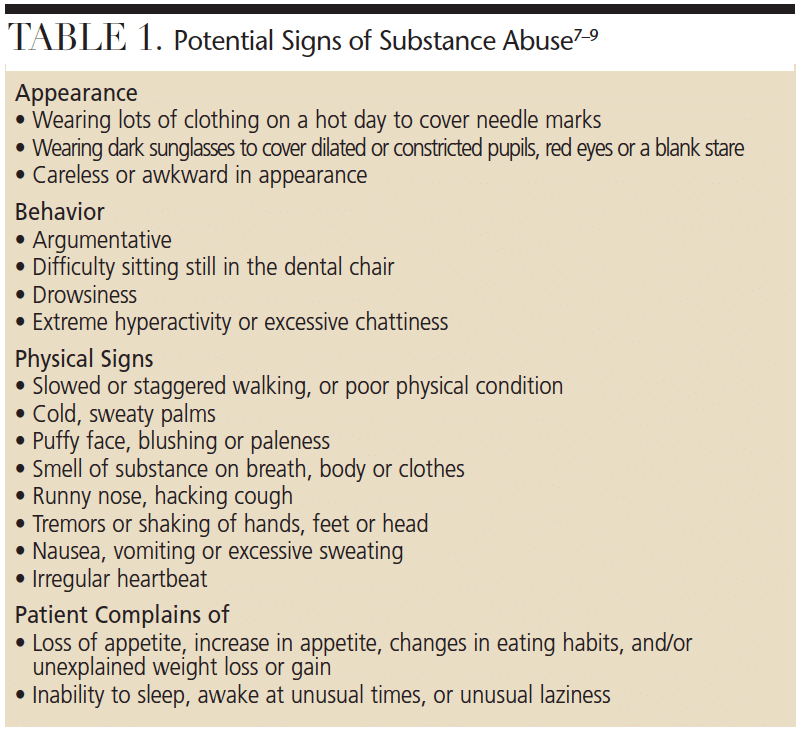
Drug abusers often present with telltale signs of their addiction. Some symptoms may not be apparent during a dental appointment — such as loss of appetite and sleeplessness — but others may be quite noticeable, even during routine examinations. Table 1 (page 52) lists some of the most obvious signs of potential substance abuse.7–9 Oral problems of drug abuse can be complex and include not only the direct effects of the drug, but also the results of poor dietary and oral hygiene habits.10–12 Patients with substance abuse disorders experience more severe caries and periodontal disease than the general population, and are less likely to receive dental care.13
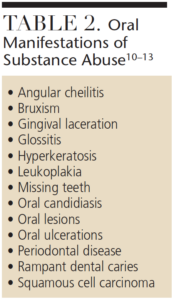
Table 2 (page 52) lists some common oral manifestations of substance abuse,10–13 a behavior that may cause suppression of the immune system, making patients susceptible to additional health problems. Diminished self-esteem, depression, and lack of motivation are also signs of drug abuse, and may negatively affect patients’ ability to adequately perform oral hygiene and regularly visit their dental provider.14–15 Diminished financial status may preclude dental treatment. When treatment becomes possible, the only financially viable alternative may be tooth extraction.
Xerostomia is often a side effect of using opiates, amphetamines, barbiturates, hallucinogens, marijuana or alcohol (Figure 2, page 52). The resulting decreased salivary flow makes users more susceptible to caries and periodontal disease. Furthermore, chemically dependent patients often crave sugar, which leads to the consumption of large quantities of sweetened beverages (for example, a dozen soft drinks per day), thereby increasing enamel erosion.16–18 Not only are large quantities of sugar consumed but, in some instances, the frequency of the sugar exposure and poor oral hygiene combined produces a devastating result.
Compared to the general population, substance abusers are at increased risk of bruxism, dentinal hypersensitivity and necrotizing ulcerative gingivitis.1,13 They also have a higher incidence of oral lesions or ulcerations and oral candidiasis. Leukoplakia, leukoedema, hyperkeratosis (Figure 3, page 52), angular cheilitis and stomatitis are more common among illicit drug users. The use and abuse of alcohol and tobacco also greatly increases the risk of oral cancer.13,19
ORAL HEALTH CARE
All patient medical history forms should include past and present drug use. There are a range of effective strategies and services available to identify, treat and manage substance abuse problems. For individuals in treatment, tandem treatment planning should be conducted with the appropriate medical providers. For patients suspected of drug abuse or addiction, oral health professionals should encourage patients to see their primary physician or make a referral to an addiction treatment specialist. (Addiction treatment specialists can be located through the American Society of Addiction Medicine at asam.org.)

Regardless of the substance being abused, the first step toward early intervention is screening to identify behaviors that put the individual at risk for harm or for developing a substance abuse disorder. It is imperative that patients receive treatment because of the degenerative effects of continued drug use increase the risk of hepatitis, human immunodeficiency virus infection, and infective endocarditis.1
At this stage, strategies for dental disease treatment and prevention can be determined. Due to the development of cross tolerance (defined as decreased pharmacological effects of a drug due to previous exposure to similar drugs), chemically-dependent patients may respond to local anesthetics differently.20 Drugs that depress the brain, such as narcotics, sedative-hypnotics and antihistamines, may enhance the effects of local anesthetics. Stimulants, such as cocaine and methamphetamine, may reduce the effects of local anesthetics. Therefore, the patient may require more local anesthesia during a dental procedure — though the maximum amount of local anesthesia that can be administered remains unchanged.21 Because chemically dependent patients are at increased risk of cardiovascular complications with epinephrine, a local anesthetic preparation without a vasoconstrictor, such as 3% mepivacaine, can be used.
Nitrous oxide analgesia should be avoided in chemically dependent patients because it is a mood-altering drug and may increase the potential for further drug abuse by creating the same or similar pleasurable sensations.2,22,23 Likewise, the use of benzodiazepines should be avoided because they, too, will create the pleasurable sensations associated with addiction. If a chemically dependent patient requires sedation with nitrous oxide or benzodiazepines for dental treatment, they should be referred to practitioners with experience in treating such patients. Individuals with a significant substance abuse history and the need for extensive dental treatment may require care in a hospital setting or an operating room.
PAIN CONTRACT
Pain history and management strategies should be discussed and thoroughly documented prior to initiating dental treatment. Postoperative pain strategies should only include acetaminophen or nonsteroidal anti-inflammatory agents, such as aspirin.23,24 These medications are contraindicated, however, in patients with liver dysfunction, gastrointestinal disorders or blood dyscrasia.23,24 A “pain contract” that outlines the specific pain management strategies may be indicated. The pain contract defines the roles and responsibilities of the provider and patient, including the termination of the relationship, without the legal concern of patient abandonment, if there is a breach of the agreement. Dentists may also prefer to work with the patient’s primary care physician in addressing the patient’s need for pain management. The patient may already have a pain contract established with his or her physician. In these instances, the dentist, after consultation with the physician, may instruct the patient to work directly with the medical provider regarding pain management needs.
Dentists should be aware of, and follow, local, state and federal regulations when prescribing controlled substances. Some states now require dentists to verify a patient’s identity (via photo identification), complete a thorough health and dental history, secure necessary radiographs or tests, establish a diagnosis, and consult a statewide prescription database prior to providing a controlled-substance prescription. Noncompliance with the prescribing regulations may result in professional liability, state licensure reviews or law enforcement investigations.
The oral manifestations of drug dependency often include rapid deterioration of the dentition and supporting structures of the oral cavity. Therefore, the immediate implementation of disease prevention strategies is recommended. For patients experiencing xerostomia, mouthrinses containing alcohol should be avoided and saliva substitutes and oral lubricant sprays can be recommended. When caries is a concern, the daily use of a 0.05% sodium fluoride mouthrinse may benefit patients. For individuals at high risk of xerostomia, high doses of topical fluoride or the use of silver diamine fluoride to arrest caries, as well as the use of chlorhexidine mouthrinse, may be the best treatment.25,26
In discussions with the patient, effective oral hygiene should be stressed, as should the importance of consistent exposure to topical fluorides, including fluoridated drinking water. Likewise, a 5% sodium fluoride varnish application is recommended at 4- to 6-month intervals to reduce caries risk.25 Diet modification is an alternative strategy to assist chemically dependent patients. Dietary changes, such as eliminating carbonated beverages, avoiding highly acidic foods and limiting overall sugar consumption, will improve oral health. Oral health professionals can assist patients in identifying healthy foods and beverages.
SUMMARY
By recognizing that substance abuse and drug addiction are serious health issues, dental professionals can promote early intervention and preventive strategies. Patients experiencing drug addiction can be treated in a general dental office setting. Dentists can — and should — address the oral health needs of patients dealing with substance abuse or addiction problems by understanding the signs and symptoms of addiction, partnering with medical teams to ensure the smooth and successful provision of care, and preventing further oral deterioration through effective preventive measures and treatment.
BONUS WEB CONTENT
REFERENCES
- U.S. Department of Health and Human Services, Office of the Surgeon General. Facing Addiction in America: The Surgeon General’s Report on Alcohol, Drugs, and Health Available at: ncbi.nlm.nih.gov/books/NBK424860/. Accessed December 4, 2017.
- National Institute on Drug Abuse. Drugs, Brains, and Behavior: the Science of Addiction. Available at: drugabuse.gov/publications/drugs-brains-behavior-science-addiction/preface. Accessed December 4, 2017.
- Nestler EJ, Malenka RC. The addicted brain. Sci Am. 2004; 290:78–85.
- Hart CL, Ksir C, Ray Oakley. Drugs, Society & Human Behavior. 13th ed. New York: McGraw–Hill; 2009.
- Guy GP, Zhang K, Bohm MK, et al. Vital signs: changes in opioid prescribing in the United States, 2006-2015. MMWR Morb Mortal Wkly Rep. 2017; 66:697–704.
- Fung EY, Giannini P. Implications of drug dependence on dental patient management. Gen Dent. 2010;58:236–241.
- Helms RA, Quan DJ, Herfindal ET, Gourley DR. Textbook of Therapeutics Drug and Disease Management. 8th ed. Philadelphia: Lippincott Williams & Wilkins; 2006.
- Byrd PB. Do you know if your patients, coworkers, friends, family, or you have an addiction? J Dent Hyg. 2001;75:65–75.
- American Council for Drug Education. Signs and Symptoms of Substance Abuse. Available at: phoenixhouse.org/prevention/signs-and-symptoms-of-substance-abuse/. Accessed December 4, 2017.
- Curtis E. Meth mouth: a review of methamphetamine abuse and its oral manifestations. Gen Dent. 2006;54:125–129.
- Morio KA, Marshall TA, Qian F, Morgan TA. Comparing diet, oral hygiene and caries status of adult methamphetamine users and nonusers: a pilot study. J Am Dent Assoc. 2008;139:171–176.
- Shetty V, Mooney LJ, Zigler CM, Belin TR, Murphy D, Rawson R. The relationship between methamphetamine use and increased dental disease. J Am Dent Assoc. 2010;141:307–318.
- Baghaie H, Kisely S, Forbes M, Sawyer E, Siskind, DJ. A systematic review and meta-analysis of the association between poor oral health and substance abuse. Addiction. 2017;112:765–779.
- Alan R. Stigma of addiction and mental health in dental settings: patients’ experiences. Available at: open.library.ubc.ca/cIRcle/collections/ubctheses/24/items/1.0167504. Accessed: December 4, 2017.
- Rasinski KA, Woll P, Cooke A. Stigma and substance use disorders. In: Corrigan PW, ed. On The Stigma of Mental Illness: Practical Strategies for Research and Social Change. Washington, DC: American Psychological Association. 2005;219–236.
- Murphy DA, Harrell L, Fintzy R, Vitero S, Gutierrez A, Shetty V. Soda consumption among methamphetamine users in the USA: impact on oral health. Oral Health Prev Dent. 2016;14:227–234.
- McFarland KK, Fung EY. The complexity of addiction. How to address the oral health needs of patients experiencing drug abuse and addiction problems. Dimensions of Dental Hygiene. 2011; 9(4):76–81.
- Goodchild JH, Donaldson M, Mangini DJ. Methamphetamine abuse and the impact on dental health. Dent Today. 2007;26:124,128–131.
- Gupta B, Bray F, Kumar N, Johnson NW. Associations between oral hygiene habits, diet, tobacco and alcohol and risk of oral cancer: a case-control study from India. Cancer Epidemiol. 2017;51:7–14.
- Friedlander AH, Mills MJ. The dental management of the drug-dependent patient. Oral Surg Oral Med Oral Pathol. 1985;60:489–492.
- The ADA/PDR Guide to Dental Therapeutics. 4th ed. Montvale, NJ: Thomson PDR;2006.
- National Institute on Drug Abuse. Principles of Drug Addiction Treatment: A Research-Based Guide. Available at: drugabuse.gov/publications/principles-drug-addiction-treatment-research-based-guide-third-edition/principles-effective-treatment. Accessed December 4, 2017.
- Moore PA, Hersh EV. Principles of pain Management in Dentistry. In: O’Neil M, ed. The ADA Practical Guide to Substance Use Disorders and Safe Prescribing. John Wiley & Sons; Hoboken, NJ:2015:33–34.
- Aminoshariae A, Kulild JC, Donaldson M. Short-term use of nonsteroidal anti-inflammatory drugs and adverse effects: an updated systematic review. J Am Dent Assoc. 2016;147:98–110.
- Beltrán-Aguilar ED, Goldstein JW, Lockwood SA Fluoride varnishes a review of their clinical use, cariostatic mechanism, efficacy and safety J Am Dent Assoc. 2000;131:589–596.
- Friedman PK, Isfeld D. Tips for treating xerostomia. Dimensions of Dental Hygiene. 2011;9(1):50–53.
The authors have no commercial conflicts of interest to disclose.
FEATURED IMAGE BY KATARZYNABIALASIEWICZZ/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. January 2018;4(1):50-53.

