

Accelerated Orthodontic Tooth Movement
The use of adjunctive surgical or noninvasive techniques and devices can help shorten treatment time, thus minimizing risk of complications.
The use of adjunctive surgical or noninvasive techniques and devices can help shorten treatment time, thus minimizing risk of complications
PURCHASE COURSE
This course was published in the February 2017 issue and expires February 2020. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Explain the clinical benefits of accelerated orthodontic treatment, and the physiologic responses to continuous pressure against a tooth.
- Identify various adjunctive surgical approaches used to accelerate tooth movement during orthodontic therapy.
- Discuss noninvasive techniques that have been used as adjuncts to speed tooth movement and the evidence that supports their use.
A perfect smile in a harmonic face associated with healthy periodontium and a functional and esthetic occlusion — coupled with long-term stability — is the desired outcome of all orthodontic treatment. Achieving these goals, however, involves potential side effects, such as root resorption, white spot lesions and periodontal problems. These risks increase as treatment time lengthens. Thus, decreasing the time required for orthodontic treatment, while achieving optimum results, would be beneficial for patients and clinicians alike.
During orthodontic therapy, forces are applied to a tooth, or group of teeth, in an attempt to achieve a better functional and/or esthetic position. The sequence of physiologic responses to a continuous pressure against a tooth begins almost immediately after application of pressure.1 These physiologic responses continue even after the tooth has been moved. When moving a tooth, the orthodontist must know the correct amount — and direction — of force necessary for the desired movement to occur. Increasing the force applied to a tooth beyond the ideal physiologic level does not result in faster tooth movement. Accelerating orthodontic tooth movement, and subsequently decreasing treatment time, is an area of keen interest to orthodontists.
Many techniques have been suggested to reduce treatment time. Some are related to the biomechanics of tooth movement, treatment approaches and appliance prescriptions. Some adjunct techniques are surgical in nature and considered to be invasive or minimally invasive (that is, they cause direct trauma to the alveolar and/or basal bone). Other adjunct techniques are noninvasive; these include lowl-level laser therapy, pharmacologic approaches, resonance vibration, ultrasound, pulsed electromagnetic fields and electrical currents. Based on the evidence in the literature, this article will focus on variations on corticotomy, lasers, pharmacology, resonance vibration and ultrasound as adjunctive techniques to help accelerate tooth movement.
CORTICOTOMY AND ITS VARIATIONS
Prior to introduction of the corticotomy technique in the late 1950s by Kole,2 the only surgical technique available to accelerate tooth movement was an osteotomy — moving either a single tooth, or group of teeth, with the associated alveolar process. Kole suggested a less invasive procedure, called a corticotomy, which consists of cuts or perforations in the cortical bone, without the need to penetrate the medullary bone. He contended that corticotomy of maxillary and mandibular bone facilitates dental movement during orthodontic therapy, reducing treatment time and chance of relapse. Since his paper, others have investigated the efficacy of corticotomy treatment.3–6 Wilcko et al7 suggested a variation of the corticotomy, later called accelerated osteogenic orthodontics, or periodontally accelerated osteogenic orthodontics (PAOO).8,9 This is also known as Wilckodontics (Figures 1A and 1B). Their technique involved labial and lingual full thickness flaps, with selective decortication and bone grafting in these areas.
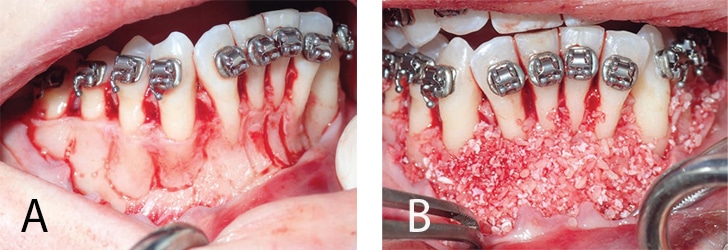
FIGURES 1A–1B COURTESY MICHEL FURTADO, BDS, MS, AND LEE SHELDON, DMD, PA
Wilcko et al proposed a time window of four months, in which the teeth can be moved more rapidly following the surgical procedure. It has also been suggested the PAOO technique can make orthodontic treatment three to four times faster.9,10 Patients must be extremely compliant, however, because orthodontic visits must occur biweekly following the surgical procedure in order to achieve maximum reduction in treatment time.
Due to the invasive surgical nature and associated sequelae of PAOO, alternatives have been proposed. One approach, introduced by Dibart et all,11 is called piezocision. This is a minimally invasive technique that combines microincisions with selective tunneling that allows hard- or soft-tissue grafting and piezoelectric incisions. Another approach involves making micro-osteoperforations through the gingiva into the interproximal alveolar bone. Although few studies have evaluated this technique, limited research indicates that such procedures reduce the time needed for tooth movement.12,13 A study by Alikhani et al13 concluded the use of micro-osteoperforation during orthodontic treatment may accelerate tooth movement by twofold or threefold, subsequently reducing the length of orthodontic treatment.
A recent systematic review concluded that “combining conventional orthodontic treatment with corticotomy reduces the duration of orthodontic treatment by accelerating tooth movement.”14 The same review indicates that few sound clinical trials have been conducted on this topic, however, and that the efficiency/safety ratio is not conclusive.
NONSURGICAL ADJUNCT PROCEDURES
Low Level Laser Therapy (LLLT): Also known as cold laser, LLLT irradiation does not increase tissue temperature by more than 1 degree C.15 It initiates a cascade of events that culminates in an increase in the cellular metabolic processes: Osteoblastic and osteoclastic activity is increased and collagen production is stimulated.15 For this reason, it was hypothesized that LLLT could accelerate tooth movement during orthodontic therapy. Yet few papers have investigated its efficacy related to orthodontic tooth movement, and the results are ambiguous. Some studies, including animal models, concluded that LLLT could accelerate movement and reduce orthodontic treatment time by up to 30%.16–18 Others, however, found no difference in time needed for tooth movement when compared to a control group.19,20 A systematic review of the efficacy of LLLT in accelerating tooth movement concluded that, due to the lack of consistency in study design and uniformity of the laser technique, it was difficult to determine whether LLLT is effective in increasing the rate of movement during orthodontic treatment.21 It is known, however, that LLLT does not harm the periodontium or increase the chance of root resorption.22,23
Pharmacological Approaches: A study investigating the effect of the protein hormone relaxin on tipping movement of the maxillary central incisors found no difference in treatment time or posttreatment relapse.24 Four animal studies investigated the administration of dihydroxyvitamin D3 (1,25-(OH)2D3),25 parathyroid hormone,26 prostaglandin E2 (PGE2)27 and osteocalcin28 to accelerate tooth movement. Due to their systemic effect on human metabolism, however, it is difficult to justify use for accelerated orthodontic treatment. At present, pharmacological approaches are not suggested due to applicability, efficacy, general health, and safety-related issues.24,29,30
Resonance Vibration: It is known that mechanical vibration can enhance bone healing and bone strength, as well as reduce undesirable effects of catabolic processes.31 Some companies have reported the use of vibrational devices can accelerate tooth movement during orthodontic therapy. Patients are instructed to use these devices for 20 minutes per day (Figure 2), the rationale being that vibration stimulates cell differentiation and maturation, resulting in faster bone remodeling and more rapid tooth movement.1 Aldrees32 notes that one sponsored study used only animal subjects, without human clinical trials, to support the idea that vibrational forces can accelerate tooth movement.

Another animal study by Nishimura et al33 demonstrated that eight minutes of resonance vibrational activity applied weekly for three weeks increased the rate of tooth movement by 15% (and with 0.18 mm greater tooth movement than the control group). Receptor activation of nuclear factor-κB ligand (RANKL) is essential for osteoclast formation and differentiation, and their production from periodontal ligament cells greatly contributes to orthodontic tooth movement.34,35 Nishimura’s team concluded that “the application of resonance vibration might accelerate orthodontic tooth movement via enhanced RANKL expression in the periodontal ligament, without additional damage to periodontal tissues, such as root resorption.”33
A retrospective, nonrandomized study by Bowman36 notes that when compared to the control group, dental alignment in the vibration device study group was 27 days faster on average, and leveling (removal or flattening of the curve of Spee) was 48 days faster. The findings were criticized since the alignment and leveling were based on the subjective decision of the clinician, who was not calibrated.32
In a more recent prospective randomized clinical trial by Woodhouse et al,37 the use of vibrational forces to reduce the time needed to achieve tooth alignment did not present significantly better results than the control group. The study used a nonfunctional device in the control group, and the authors only investigated the rate of tooth alignment. Aldrees states that more reliable, independent, randomized and controlled trials are necessary in order to investigate the efficiency of orthodontic treatment facilitated by vibrational devices.32
Ultrasound: With a frequency above the limit of perception by the human ear, ultrasound waves can be transmitted into biological tissues and are widely used in medicine for diagnostic, as well as therapeutic, purposes.38 Low-intensity pulsed ultrasound (LIPUS) has been utilized effectively as a therapeutic modality for bone regeneration and fracture healing.39 Introducing ultrasound to the alveolar process during orthodontic treatment, in theory, facilitates tooth movement by altering periodontal biology.1 Histological studies suggest that LIPUS influences osteoblasts, osteoclasts, chondrocytes and mesenchymal stem cells, which are all involved in the bone-healing mechanism.40
Using a rat orthodontic tooth movement model, Xue et al41 demonstrated that LIPUS promotes alveolar bone remodeling by stimulating the HGF/Runx2/BMP-2 signaling pathway and RANKL expression. The researchers noted that LIPUS was able to accelerate orthodontic tooth movement by 45% after 14 days of treatment. Conversely, using a dog model, Al-Daghreer et al42 found no difference in tooth movement, even after using LIPUS 20 minutes per day during four weeks of orthodontic treatment. Clearly, more research is needed to adequately evaluate the efficacy of LIPUS on the rate of orthodontic tooth movement.
SUMMATION
This article presents the most common techniques for accelerating tooth movement during orthodontic treatment. Among the modalities discussed, corticotomy has demonstrated the most encouraging, evidence-supported results — although additional clinical trials are needed, and an efficiency/safety ratio has not been established.
Following corticotomy is LLLT, a technique that appears to be safe, but for which data on accelerated tooth movement is inconclusive. Ultrasound and vibrational devices still require additional research in order to evaluate their efficacy in shortening treatment time. Lastly, and based on the evidence, pharmacological approaches are not yet safely applicable in an orthodontic setting as a method of accelerating tooth movement to reduce treatment time.
REFERENCES
- Proffit W, Fields H. Sarver D. Contemporary Orthodontics. 5th ed. St. Louis: Mosby; 2013.
- Kole H. Surgical operations on the alveolar ridge to correct occlusal abnormalities. Oral Surg Oral Med Oral Pathol. 1959;12:515–529.
- Duker J. Experimental animal research into segmental alveolar movement after corticotomy. J Maxillofac Surg. 1975;3:81–84.
- Generson RM, Porter JM, Zell A, Stratigos GT. Combined surgical and orthodontic management of anterior open bite using corticotomy. J Oral Surg. 1978;36:216–219.
- Fitzpatrick BN. Corticotomy. Aust Dent J. 1980;25:255–258.
- Bhattacharya P, Bhattacharya H, Anjum A, et al. Assessment of corticotomy facilitated tooth movement and changes in alveolar bone thickness — A CT scan study. J Clin Diagn Res. 2014;8:ZC26–ZC30.
- Wilcko WM, Wilcko T, Bouquot JE, Ferguson DJ. Rapid orthodontics with alveolar reshaping: two case reports of decrowding. Int J Periodontics Restorative Dent. 2001;21:9–19.
- Murphy KG, Wilcko MT, Wilcko WM, Ferguson DJ. Periodontal accelerated osteogenic orthodontics: a description of the surgical technique. J Oral Maxillofac Surg. 2009;67:2160–2166.
- Wilcko MT, Wilcko WM, Pulver JJ, Bissada NF, Bouquot JE. Accelerated osteogenic orthodontics technique: a 1-stage surgically facilitated rapid orthodontic technique with alveolar augmentation. J Oral Maxillofac Surg. 2009;67:2149–2159.
- Sebaoun JD, Ferguson DJ, Wilcko MT, Wilcko WM. [Alveolar osteotomy and rapid orthodontic treatments]. Orthod Fr. 2007;78:217–225.
- Dibart S, Sebaoun JD, Surmenian J. Piezocision: a minimally invasive, periodontally accelerated orthodontic tooth movement procedure. Compend Contin Educ Dent. 2009;30:342– 344,346,348–350.
- Tsai CY, Yang TK, Hsieh HY, Yang LY. Comparison of the effects of microosteoperforation and corticision on the rate of orthodontic tooth movement in rats. Angle Orthod. 2016;86:558–564.
- Alikhani M, Raptis M, Zoldan B, et al. Effect of micro-osteoperforations on the rate of tooth movement. Am J Orthod Dentofacial Orthop. 2013;144:639–648.
- Fernández-Ferrer L, Montiel-Company JM, Candel-Martí E, Almerich-Silla JM, Peñarrocha-Diago M, Bellot-Arcís C. Corticotomies as a surgical procedure to accelerate tooth movement during orthodontic treatment: A systematic review. Med Oral Patol Oral Cir Bucal. 2016;21:e703–e712.
- Chung H, Dai T, Sharma SK, et al. The nuts and bolts of low-level laser (light) therapy. Ann Biomed Eng. 2012;40:516–533.
- Doshi-Mehta G, Bhad-Patil WA. Efficacy of low-intensity laser therapy in reducing treatment time and orthodontic pain: a clinical investigation. Am J Orthod Dentofacial Orthop. 2012;141:289–297.
- Genc G, Kocadereli I, Tasar F, et al. Effect of low-level laser therapy (LLLT) on orthodontic tooth movement. Lasers Med Sci. 2013;28:41–47.
- Shirazi M, Ahmad Akhoundi MS, Javadi E, et al. The effects of diode laser (660 nm) on the rate of tooth movements: an animal study. Lasers Med Sci. 2015;30:713–718.
- Heravi F, Moradi A, Ahrari F. The effect of low level laser therapy on the rate of tooth movement and pain perception during canine retraction. Oral Health Dent Manag. 2014;13:183–188.
- Altan BA, Sokucu O, Ozkut MM, Inan S. Metrical and histological investigation of the effects of low-level laser therapy on orthodontic tooth movement. Lasers Med Sci. 2012;27:131–140.
- Sonesson M, De Geer E, Subraian J, Petren S. Efficacy of low-level laser therapy in accelerating tooth movement, preventing relapse and managing acute pain during orthodontic treatment in humans: a systematic review. BMC Oral Health. 2016;17:11.
- Cruz DR, Kohara EK, Ribeiro MS, Wetter NU. Effects of low-intensity laser therapy on the orthodontic movement velocity of human teeth: a preliminary study. Lasers Surg Med. 2004;35:117–120.
- Sousa MV, Scanavini MA, Sannomiya EK, Velasco LG, Angelieri F. Influence of low-level laser on the speed of orthodontic movement. Photomed Laser Surg. 2011;29:191–196.
- McGorray SP, Dolce C, Kramer S, Stewart D, Wheeler TT. A randomized, placebo-controlled clinical trial on the effects of recombinant human relaxin on tooth movement and short-term stability. Am J Orthod Dentofacial Orthop. 2012;141:196–203.
- Kawakami M, Takano-Yamamoto T. Local injection of 1,25-dihydroxyvitamin D3 enhanced bone formation for tooth stabilization after experimental tooth movement in rats. J Bone Miner Metab. 2004;22:541–546.
- Soma S, Iwamoto M, Higuchi Y, Kurisu K. Effects of continuous infusion of PTH on experimental tooth movement in rats. J Bone Miner Res. 1999;14:546–554.
- Yamasaki K, Shibata Y, Fukuhara T. The effect of prostaglandins on experimental tooth movement in monkeys (Macaca fuscata). J Dent Res. 1982;61:1444–1446.
- Hashimoto F, Kobayashi Y, Mataki S, et al. Administration of osteocalcin accelerates orthodontic tooth movement induced by a closed coil spring in rats. Eur J Orthod. 2001;23:535–545.
- Bartzela T, Turp JC, Motschall E, Maltha JC. Medication effects on the rate of orthodontic tooth movement: a systematic literature review. Am J Orthod Dentofacial Orthop. 2009;135:16–26.
- Qamruddin I, Alam MK, Khamis MF, Husein A. Minimally invasive techniques to accelerate the orthodontic tooth movement: A systematic review of animal studies. Biomed Res Int. 2015;2015:608530.
- Xie L, Rubin C, Judex S. Enhancement of the adolescent murine musculoskeletal system using low-level mechanical vibrations. J Appl Physiol. 2008;104:1056–1062.
- Aldrees AM. Do customized orthodontic appliances and vibration devices provide more efficient treatment than conventional methods? Korean J Orthod. 2016;46:180–185.
- Nishimura M, Chiba M, Ohashi T, et al. Periodontal tissue activation by vibration: intermittent stimulation by resonance vibration accelerates experimental tooth movement in rats. Am J Orthod Dentofacial Orthop. 2008;133:572–583.
- Yasuda H, Shima N, Nakagawa N, et al. Osteoclast differentiation factor is a ligand for osteoprotegerin/osteoclastogenesisinhibitory factor and is identical to TRANCE/RANKL. Proc Natl Acad Sci U S A. 1998;95:3597–3602.
- Garlet TP, Coelho U, Silva JS, Garlet GP. Cytokine expression pattern in compression and tension sides of the periodontal ligament during orthodontic tooth movement in humans. Eur J Oral Sci. 2007;115:355–362.
- Bowman SJ. The effect of vibration on the rate of leveling and alignment. J Clin Orthod. 2014;48:678–688.
- Woodhouse NR, DiBiase AT, Johnson N, et al. Supplemental vibrational force during orthodontic alignment: a randomized trial. J Dent Res. 2015;94:682–689.
- Maylia E, Nokes LD. The use of ultrasonics in orthopaedics — a review. Technol Health Care. 1999;7:1–28.
- Mundi R, Petis S, Kaloty R, Shetty V, Bhandari M. Low-intensity pulsed ultrasound: Fracture healing. Indian J Orthop. 2009;43:132–140.
- Claes L, Willie B. The enhancement of bone regeneration by ultrasound. Prog Biophys Mol Biol. 2007;93:384–398.
- Xue H, Zheng J, Cui Z, et al. Low-intensity pulsed ultrasound accelerates tooth movement via activation of the BMP-2 signaling pathway. PLoS One. 2013;8:e68926.
- Al-Daghreer S, Doschak M, Sloan AJ, et al. Effect of low-intensity pulsed ultrasound on orthodontically induced root resorption in beagle dogs. Ultrasound Med Biol. 2014;40:1187–1196.
Featured photo by CREATAS IMAGES/CREATAS/THINKSTOCK
From Decisions in Dentistry. February 2017;3(2):36–39.

